Article Text

Abstract
Objectives Current guidelines for screening for blunt cerebrovascular injury (BCVI) are commonly based on the expanded Denver criteria, a set of risk factors that identifies patients who require CT-angiographic (CTA) screening for these injuries. Based on previously published data from our center, we have adopted a more liberal screening guideline than those outlined in the expanded Denver criteria. This entails routine CTA of the neck for all blunt trauma patients already undergoing CT of the cervical spine and/or CTA of the chest. The aim of this study was to analyze the incidence of patients with BCVI who did not meet any of the risk factors included in the expanded Denver criteria.
Methods A retrospective review of all patients diagnosed with BCVI between June 2014 and December 2019 at a Level I Trauma Center were identified from the trauma registry. Medical records were reviewed for the presence or absence of risk factors as outlined in the expanded Denver criteria. Demographic data, time to CTA and treatment, BCVI grade, Glasgow Coma Scale and Injury Severity Score were collected.
Results During the study period, 17 054 blunt trauma patients were evaluated, and 29% (4923) underwent CTA of the neck to screen for BCVI. 191 BCVIs were identified in 160 patients (0.94% of all blunt trauma patients, 3.25% of patients screened with CTA). 16% (25 of 160) of patients with BCVI had none of the risk factors outlined in the Denver criteria.
Conclusion Our findings indicate that reliance on the expanded Denver criteria alone for BCVI screening will result in missed injuries. We recommend CTA screening in all patients with blunt trauma undergoing CT of the cervical spine and/or CTA of the chest to minimize this risk.
Level of evidence Level III, therapeutic/care management.
- brain injuries, traumatic
- vertebral artery
- carotid artery injuries
- angiography
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Reliance on clinical screening criteria alone to screen for blunt cerebrovascular injury (BCVI), namely the expanded Denver criteria, has been shown to miss a substantial numbers of injuries.
What this study adds
This study shows that obtaining a CT angiography (CTA) of the neck in all patients who are already undergoing a CT of the cervical spine or CTA of the chest will capture substantially more injuries than reliance on clinical screening criteria alone.
How this study might affect research, practice or policy
The implementation of this guideline simplifies which patients warrant screening for BCVI and captures more injuries.
Introduction
Blunt cerebrovascular injuries (BCVIs) most commonly occur from either a direct injury or sudden stretching of the internal carotid or vertebral arteries resulting in disruption of integrity of the layers of the vessel wall.1–3 This is often a result of high impact mechanisms such as motor vehicle crash, which have been shown to account for nearly 50% of these injuries.4–7 However, recent data have suggested that lower mechanisms of injury can also result in BCVIs.8 Although these injuries are rare, with early studies reporting an incidence of around 1% of all blunt trauma victims,4 9 improving imaging technology and widespread screening has resulted in the identification of more injuries than previously described.3 10
Identifying patients at risk for these injuries has been the subject of debate since the release of the initial screening recommendations 20 years ago.9 Since publication of these initial recommendations, screening has commonly been based on the Denver criteria and its subsequent revision, the New Denver Health BCVI Screening Guidelines or expanded Denver criteria (figure 1).6 10–12 Despite advances in imaging technology and expansion of screening criteria, a number of studies have suggested that the current recommendations for screening for BCVIs, such as the expanded Denver criteria, fail to identify as many as 37% of injuries.7 13–16

The expanded Denver criteria.11 BCVI, blunt cerebrovascular injury; TIA, transient ischemic attack; TBI, traumatic brain injury; GCS, Glasgow Coma Scale.
Left untreated, BCVIs can have catastrophic consequences, with documented stroke rates of 9% to 11% and associated mortality of 16% to 27%.3 4 It has long been known that best way to improve patient outcome is with early detection and treatment of these injuries with antithrombotic and antiplatelet agents.17–19 A recent study has also suggested that a hypercoagulable state may be contributory to BCVI-related ischemic events.20 Choice of anticoagulant/antiplatelet therapy continues to be guided on the basis of the severity of the vessel injury and clinical situation. The standard remains in question, although studies have shown antiplatelet agents to be equivalent to systemic anticoagulation.17
With awareness of the increased incidence of these injuries, the question of which patients warrant screening remains. Recent publications have demonstrated both more liberal and universal screening guidelines to be beneficial in identifying these injuries7 13–15 and preventing subsequent strokes.21
Beginning in 2012, our institution implemented a new liberal BCVI screening guideline in which all blunt trauma patients evaluated by the trauma service with injuries significant enough to warrant a CT cervical spine and/or CT angiography (CTA) of the chest underwent a simultaneous CTA of the neck to assess for BCVI. The aim of this study was to analyze the incidence of patients with BCVI who did not meet any of the risk factors included in the expanded Denver criteria.
Methods
This study was performed at a suburban American College of Surgeons-verified Level I Trauma Center. It serves as the tertiary/quaternary referral center for a 25 hospital system within the state as well as several other hospitals in surrounding counties. Beginning in May of 2012, we implemented a clinical practice guideline for screening for BCVI. This guideline was continued after initial data from 2012 to 2014 showed that a significant number of BCVIs would not have been identified by the expanded Denver criteria.13 Under this screening guideline, all patients with injuries or a mechanism of injury significant enough to warrant CT of the cervical spine and/or CTA of the chest underwent simultaneous CTA of the neck to assess for BCVI.
CTA was performed using our GE VCT 64 slice, GE 750HD 64 slice, or GE Revolution 128 slice CT scanners. Imaging protocol was performed as previously described by our group13 with the goal of minimizing both the radiation and contrast load delivered. Patients were placed head-first in the CT scanner and secured with their arms at their sides. CT scans of the head and face were performed first if clinically indicated, followed by CT scan of the cervical spine and a CTA of the neck. The CT of the cervical spine and CTA of the neck were performed in a single run to minimize radiation exposure. CTA (arterial phase) of the chest, abdomen, and pelvis and CT of the abdomen and pelvis (venous phase) were performed last if clinically indicated.
Sixty mL of iohexol 350 at 4 mL/s followed by 20 mL of 0.9% normal saline was used for CTA of the neck. Imaging was begun once contrast was visualized entering the aortic arch. All images were obtained at 0.625 mm slice thickness at 0.625 mm intervals. Reformatted sagittal images were done at 2 mm by 2 mm. Coronal and sagittal reformats were performed in maximal intensity projection mode (10 mm × 2.5 mm).
CT scans of the cervical spine were performed simultaneously with the CTA of the neck. Sagittal and coronal images were manually reformatted in bone window at 2 mm by 2 mm, sagittal images were reformatted in standard window at 2 mm by 2 mm, and angled axial images were reformatted in both bone and standard window at 2.5 mm by 2.5 mm.
CTA of the chest was done using 90 mL of iohexol 350 at an injection rate of 4 mL/s. After contrast, patients received 20 mL of 0.9% sodium chloride. During the arterial phase, images were captured at 0.625 mm by 0.625 mm. Coronal and sagittal images were reformatted at 3 mm by 2 mm. Coronal and sagittal images were also reformatted in maximal intensity projection mode at 5 mm by 3 mm.
All studies were reviewed by a neuroradiologist. Patients found to have injuries were subsequently evaluated by neurosurgery. Carotid and vertebral artery injuries were graded using the Biffl Injury Grading Scale for BCVI.22 In this scale, a grade 1 injury had<25% luminal narrowing, grade 2 injury had>25% narrowing, grade 3 injury had a pseudoaneurysm, grade 4 had complete vessel occlusion, and grade 5 had vessel transection with extravasation. For patients with multiple carotid or vertebral injuries, all injuries were counted and recorded including their grade. Unless clinically contraindicated, treatment was initiated with an antiplatelet agent, systemic anticoagulation, or combination of the two at the discretion of the attending neurosurgeon.
This retrospective cohort study was reviewed and approved by our organization’s Institutional Review Board. All patients with documented BCVI from June of 2014 to December of 2019 were identified from our trauma registry, which is compliant with the American College of Surgeons Committee on Trauma’s National Trauma Data Standard. Medical records from the patients' encounters were then reviewed for the presence or absence of risk factors as outlined in the expanded Denver criteria (figure 1). Patient demographic data, mechanism of injury, presence of BCVI risk factor(s), initial Glasgow Coma Scale (GCS), Injury Severity Score (ISS), time from presentation to CTA neck and treatment, BCVI grade, anticoagulation type, occurrence of cerebral ischemic events, length of stay, and patient outcome were collected. The Research Electronic Data Capture (REDCap) collection software was used for the storage and subsequent filtering of the extracted patient information for analysis. The Equator Network STROBE guidelines were used to guide the content in this article.
Statistical analysis was performed in R V.4.0.1. Comparisons of covariates between patients who did and did not meet Denver criteria were tested for statistical significance using Student’s t-tests, two proportion z-tests, and Fisher’s exact tests as appropriate. A χ2 test of independence was used to analyze if patients’ mechanism of injury was related to their Denver criteria status.
Results
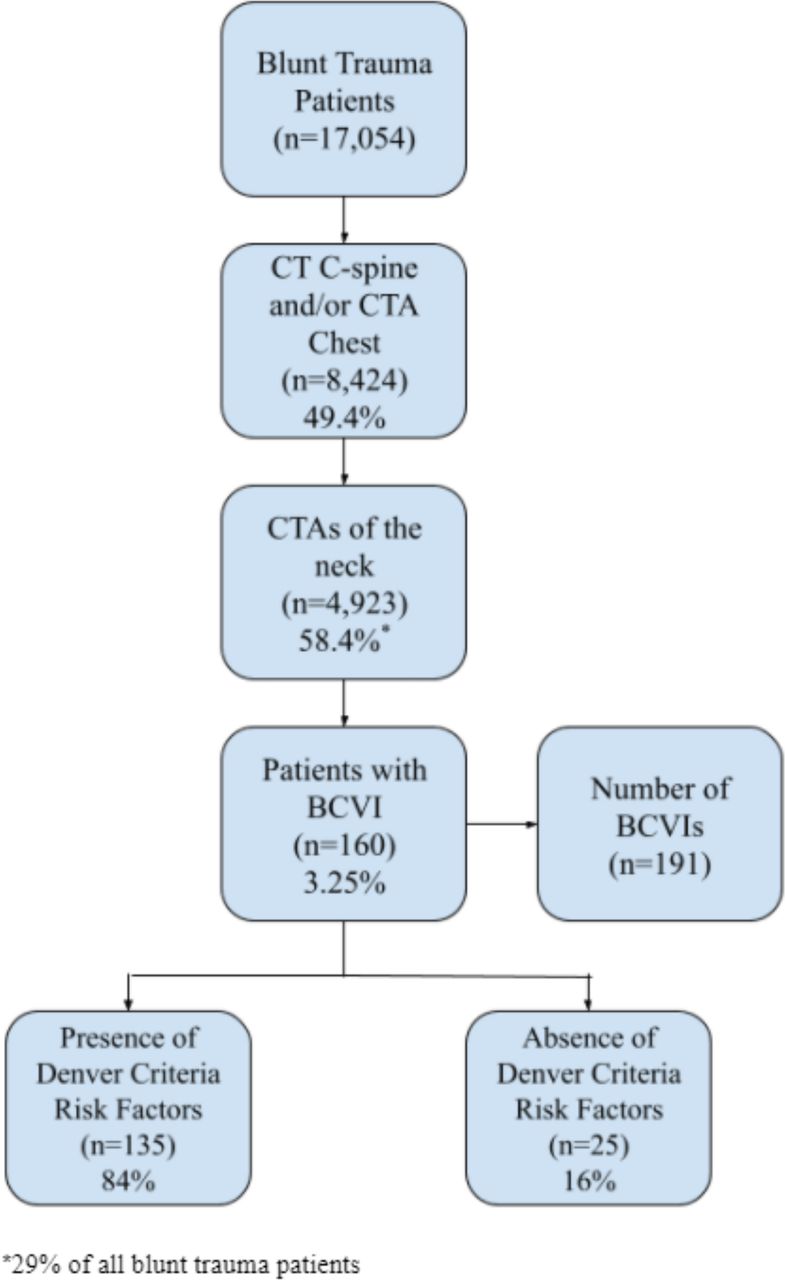
During the study period, 17 054 blunt trauma patients were evaluated, and 29% (4923) underwent CTA of the neck to screen for BCVI (figure 2). There were 191 BCVIs identified in 160 patients (0.94% of all blunt trauma patients, 3.25% of patients screened with CTA). Overall, 135 (84%) had at least one of the risk factors outlined in the Denver criteria. However, in 25 (16%), none of the risk factors outlined in the expanded Denver criteria were present.
{kind=link}
{kind=link}
Overview of BCVI screening in all blunt trauma patients: overview of BCVI screening for the study period where n=number of patients. BCVI, blunt cerebrovascular injury; CTA, CT angiography.
Variables in patients with BCVI are outlined in table 1 by presence or absence of expanded Denver criteria. Patients who met one of the Expanded Denver Criteria were more severely injured as indicated by a lower initial GCS (11.6 vs 13.6, p=0.018), higher average ventilator days (5.4 vs 1.8, p= <0.001), intensive care unit length of stay (6.6 vs 3, p=0.003), overall length of stay (11.6 vs 7, p=0.001), and ISS (22.1 vs 14.7, p=0.004). There was wide variability in the time to CTA neck and time to treatment between these two groups and therefore differences were not statistically significant. The number of strokes and deaths were small and differences in these variables were also not statistically significant.
Variables in patients with BCVI by presence or absence of expanded Denver criteria
There were 16 patients with BCVI who suffered strokes and the hospital course of these patients was analyzed in detail. Of these patients, five (31.2%) were felt to be unrelated to the BCVI: four were related to diffuse anoxic brain injury and one was due to a depressed skull fracture with extensive shear injury not in the distribution of the BCVI.
Mechanism of injury by presence or absence of expanded Denver criteria is shown in table 2. In both groups, the most common mechanism of injury was motor vehicle collisions (68.7%), followed by falls (13.7%). Of the 22 falls, 12 (54%) were from standing and 4 (18%) did not have any of the clinical risk factors outlined from the expanded Denver criteria. The distribution of mechanism of injury was independent of the presence or absence of any of the expanded Denver criteria as demonstrated by a χ2 test (χ2=4.57, df=8, p=0.802).
Patient mechanism of injury by presence or absence of expanded Denver criteria
The distribution of injury grade by presence or absence of expanded Denver criteria is outlined in table 3. Of the 25 patients who did not have risk factors outlined in the expanded Denver criteria, 13 (52%) had grade 2 or higher injuries. Of the 135 patients who had risk factors present in the expanded Denver criteria 39 (66%) had grade 2 or higher injuries.
Biffl injury grade by presence or absence of expanded Denver criteria
The occurrence of stroke comparing internal carotid and vertebral artery injuries is outlined in table 4. There were 191 vessels injured, resulting in 11 strokes (5.8%). The difference in incidence of stroke between internal carotid and vertebral injuries was not statistically significant. Of the 11 strokes related to BCVI, 5 occurred after the initiation of treatment and can be considered treatment failures. For those who had a stroke after admission, the average time from admission to stroke was 3.66 days. Among patients who experienced a stroke related to BCVI, the mortality rate was 18%.
Injured vessels and stroke rates
Discussion
Several studies have demonstrated that the current screening guidelines for BCVI fail to identify 17% to 37% of these injuries.7 13–15 Recognizing the limitations of relying on risk factors alone to identify patients in whom CTA screening for BCVI is warranted, we implemented a more liberal screening guideline for BCVI in 2012 in which all blunt trauma patients who underwent a CT of the cervical spine and/or CTA of the chest underwent a simultaneous CTA of the neck to assess for these injuries. Prior to implementation of this guideline, only 1.5% of all blunt trauma patients were evaluated with a CTA of the neck.13 After implementation, this rate initially increased to 19% between 2012 and 201413 and in the current study has increased to 29% (4923 of 17 054). During the earlier time period, the incidence of BCVI increased from 0.2% to 1.1% of all blunt trauma patients. In the current study, the incidence of BCVI was 0.94% (160 of 17 054) of all blunt trauma patients and 3.25% (160 of 4923) of patients who underwent CTA of the neck. This incidence is in line with several recent studies using various iterations of ‘liberal’ or ‘universal’ screening for BCVI.7 14 15 We also identified that 16% of BCVI had none of the clinical or radiological risk factors outlined in the expanded Denver criteria. In all likelihood, these injuries are being missed in centers relying solely on these criteria. This finding confirms our hypothesis that use of screening criteria fails to identify a significant percentage of patients with these injuries. In addition, it is not only minor injuries that would be missed. We found that 52% of patients who did not meet any of the expanded Denver criteria had Biffl grade 2 or higher injuries. As reported from previous studies,17–19 23 without treatment these patients would be at a significant risk of stroke and mortality. We also identified no difference in the mechanism of injury between patients with BCVI who met criteria and those who did not, thereby limiting the utility of using low mechanism of injury to avoid using CTA screening. Not unexpectedly, those who do not have risk factors outlined in the expanded Denver criteria had a significantly lower ISS (22.1 vs 14.7, p<0.004). This further reinforces the notion that patients with low mechanism of injury and lower injury severity are still at risk for BCVI and that CTA screening is warranted in these patients. In addition, 13.7% of BCVIs in our study resulted from falls—12 (7.5%) of which were from standing. Of the 22 falls, 18% did not have any of the clinical risk factors outlined from the expanded Denver criteria. This supports findings from Anto et al, who reported that elderly patients with ground-level falls have a clinically significant risk of BCVI despite a low-impact mechanism of injury.8
Our data corroborate several recent publications that advocate for more expansive screening for BCVIs in the blunt trauma patient population.7 13–15 Leichtle et al made the recommendation for universal BCVI screening in all trauma activations.7 According to their findings, 17% of BCVIs would have been missed by the most sensitive current screening guidelines.7 Comparatively, our data identified an almost identical incidence of injuries that would have been missed (16%) with the application of a well-defined liberal screening guideline. Most recently, Black et al reviewed their experience with universal screening. In their study, 6287 of 6800 (92.5%) blunt trauma patients underwent CTA of the neck, identifying 480 BCVIs (7.6%).14 They similarly demonstrated that 25.3% of patients with BCVI identified with universal screening had none of the clinical risk factors included in the expanded Denver criteria.
Universal screening does raise concern for increased exposure to radiation and nephrotoxic contrast. Our guideline mitigates these concerns by screening those patients who are already undergoing CT of the cervical spine and/or receiving contrast for a CTA of the chest. In patients already undergoing a CT of the cervical spine, the CTA neck and CT cervical spine are performed in a single run and patients do not receive any additional radiation exposure. In patients undergoing a CTA of the chest, the increase in contrast administered is minimal. In addition, simultaneous CTA of the neck avoids a return to CT for a separate study in patients in whom one of the expanded Denver criteria risk factors are identified on the initial imaging.
Early recognition of these injuries and initiation of treatment during the initial latent asymptomatic period is crucial in the prevention of progression to stroke.12 17 19 23 A recent review of the National Trauma Data Bank demonstrated an incidence of stroke of 9% in the post-expanded Denver criteria era.3 In our study, the incidence of stroke occurring as a direct result of BCVI was 6.9% or 5.8% (11 of 191) per vessel injured. Our treatment guideline (online supplemental file 1), developed in collaboration with neurosurgery, uses aspirin 325 mg daily for carotid artery injuries until a scheduled follow-up in 3 months for repeat imaging. Patients with Biffl grade 1 or 2 vertebral artery injuries are started on aspirin 81 mg daily for 6 months with no follow-up imaging and those with Biffl 3 or 4 injuries are started on 325 mg aspirin daily with follow-up imaging at 3 months.
Supplemental material
This study has several limitations. Overall, only 29% of blunt trauma patients underwent CTA of the neck. It is likely that a number of patients with low mechanism of injury were not felt to require CT of the cervical spine and/or CTA of the chest and, therefore, did not undergo CTA of the neck. Although there may be variation between centers and clinicians for obtaining CT of the cervical spine and or CTA of the chest, our recommendation to obtain CTA of the neck at the same time as these studies can be used irrespective of local protocol and mitigates the need for the CTA of the neck to be obtained separately. In those patients undergoing a CT of the cervical spine and/or CTA of the chest, 58.4% underwent CTA of the neck. Although the intent of our screening guideline was to obtain a CTA of the neck in all patients undergoing CT of the cervical spine and/or CTA of the chest, several factors contributed to incomplete adherence to the guideline. Radiologic workup of lower level trauma activations and non-activations was initiated by our emergency medicine physicians and at the time of implementation, CTA of the neck in the absence of any of the expanded Denver criteria was not yet considered the standard of care. In addition, approximately 38% of patients were transferred from other hospitals and many had already undergone CT of the cervical spine and/or CTA of the chest. These patients only underwent CTA of the neck post-transfer if one of the expanded Denver criteria was present. Finally, patients with chronic kidney disease and allergy to contrast did not routinely undergo CTA of the neck. Another limitation of the study is that it is a retrospective cohort study at a single center, which is subject to selection bias and may not be generalizable to all centers. To mitigate some of these concerns, we plan to expand our clinical screening guideline for BCVI within our emergency medicine physician group for patients seen prior to consultation of the trauma service and to recommend implementation at referring hospitals within our catchment area.
Our findings indicate that reliance on the expanded Denver criteria alone for BCVI screening will result in missed injuries. Because of this, use of these guidelines should be reconsidered in favor of more liberal screening. Obtaining a simultaneous CTA of the neck in patients with a mechanism of injury sufficient enough to warrant a CT of their cervical spine and/or CTA of the chest minimizes additional radiation exposure and contrast toxicity and will identify injuries that would otherwise have been missed. We therefore recommend implementation of this routine screening guideline to capture those patients with BCVI who have none of the clinical or radiological risk factors outlined in current clinical screening criteria.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Literature search/study design: PRH, LEJ, JMW. Data collection: PRH, LEJ, JMW. Data analysis/data interpretation: ZS, PRH, LEJ, JMW. Writing: PRH. Critical revisions: PRH, LEJ, JMW, ZS, RBR. Guarantors: PRH, LEJ
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.