Article Text

Abstract
Background Resuscitative endovascular balloon occlusion of the aorta (REBOA) is a torso hemorrhage control technique. To expedite deployment, inflation is frequently performed as a blind technique with minimal imaging, which carries a theoretical risk of aortic injury. The objective of this study was to examine the relationship between balloon inflation, deformation and the risk of aortic rupture.
Methods Compliant balloon catheters were incrementally inflated in segments of cadaveric swine aorta. Serial longitudinal and circumferential measurements were recorded, along with the incidence of aortic rupture.
Results Fourteen cadaveric swine aorta segments were tested with mean (±SD) baseline aortic diameter (mm) of 14.2±3.4. Rupture occurred in three aortas. The mean baseline diameters (mm) of the aortic segments that were ruptured were significantly smaller than those that did not rupture (8.9±1.2 vs 15.6±1.9; P<0.001). The maximal circumferential stretch ratios were significantly higher in the aorta segments that ruptured compared with those that did not (1.9±0.1 vs 1.5±0.1; P<0.001). The maximal amount of balloon longitudinal deformation was 80 mm (116% longer than the intended working length).
Conclusions Inflation of aortic balloon catheters carries an inherent risk of aortic injury, which may be minimized through an understanding of the intrinsic characteristics of the aorta and compliant balloons. Smaller diameter aortic segments undergoing overinflation, particularly beyond a circumferential stretch ratio of 1.8, are at risk of aortic rupture.
Level of evidence Level II.
- resuscitative endovascular balloon occlusion of the aorta
- reboa
- aortic rupture
- arterial injury
- blind inflation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- resuscitative endovascular balloon occlusion of the aorta
- reboa
- aortic rupture
- arterial injury
- blind inflation
Background
Resuscitative endovascular balloon occlusion of the aorta (REBOA) is a technique for the control of torso hemorrhage in trauma. A compliant balloon is inserted via the femoral artery and inflated in the thoracic (zone 1) or infrarenal (zone 3) aorta, providing inflow control of the abdomen or pelvis, respectively. Originally, this technique was described using conventional endovascular equipment, consisting of large sheaths, wires and balloon catheters, guided by fluoroscopy.1 2 However, in an effort to expedite the procedure, smaller caliber balloon catheters have been developed, which do not require a wire or fluoroscopic imaging.
The concern with blind placement is the risk of overinflation and potential for aortic rupture. Several cases have been described in the literature which have related to both non-diseased and diseased, with and without imaging.3-11 Of particular concern are patients with small caliber aortas who have balloon inflation without radiographic guidance. Due to the nature of morbidity reporting, the literature likely underestimates this issue. The structural integrity of the aorta has been well described in the context of aortic clamping and compressive strength,12-14 but the expansile failure threshold has yet to be fully characterized.
This study has three aims. First, we aim to introduce the metrics of aortic mechanics in an endovascular context. Second, using explanted porcine aortas, characterize the relationship between balloon inflation and balloon and aortic deformation, including aortic rupture risk. Lastly, define a threshold which is associated with aortic rupture.
Methods
Study overview
This in vitro study characterizes the rupture threshold of fresh, untreated, explanted porcine aortas, using a commercially available balloon catheter (ER-REBOA catheter, Prytime Medical Inc., Boerne TX, USA). Aortas were harvested from Yorkshire swine (Sus scrofa) weighing between 70 kg and 90 kg. Institutional Animal Care and Use Committee (IACUC) approval was not required as this was a postmortem study.
Definitions and terminology
The field of soft-tissue mechanics and failure is complex and has its own field of study within the physical sciences. For the purposes of the current study, it is important to have a basic understanding of terminology, which is relevant to endovascular practice and are discussed below.
The aorta is anisotropic, compliant and distensible, with the ability to stretch more in the circumferential direction than the longitudinal direction.15 These intrinsic properties of the aorta result in a physiologically important function, allowing for the prevention of pathologic increases in systolic blood pressure, afterload and pulse pressure. This is accomplished through a buffer-reservoir type effect during systole and also by attenuating pressure decay during diastole.16 17
Given the compliant nature of the aorta, the aorta stretches under pressure until it reaches its maximal stretching threshold. The amount of force required to break the aorta when being stretched is termed the ultimate tensile strength; however, this value changes depending on the degree of stretch experienced in the orthogonal dimension and is reached after a critical stretch ratio has been reached. In an endovascular context, the amount the aorta stretches in the circumferential direction is of particular interest, and this ratio is defined as:

When a compliant balloon catheter is inflated, the balloon will ‘unpack’ and start to fill, eventually opposing the vessel wall, occluding the lumen. Compliant balloons are generally constructed with proximal and distal radio-opaque markers, which denote the ‘intended working length’ of the balloon, or the portion in contact with the vessel wall. However, in reality, the proportion of material in contact with the wall can be greater or lesser depending on the balloon volume and this is termed the balloon ‘footprint’ (figure 1 A).
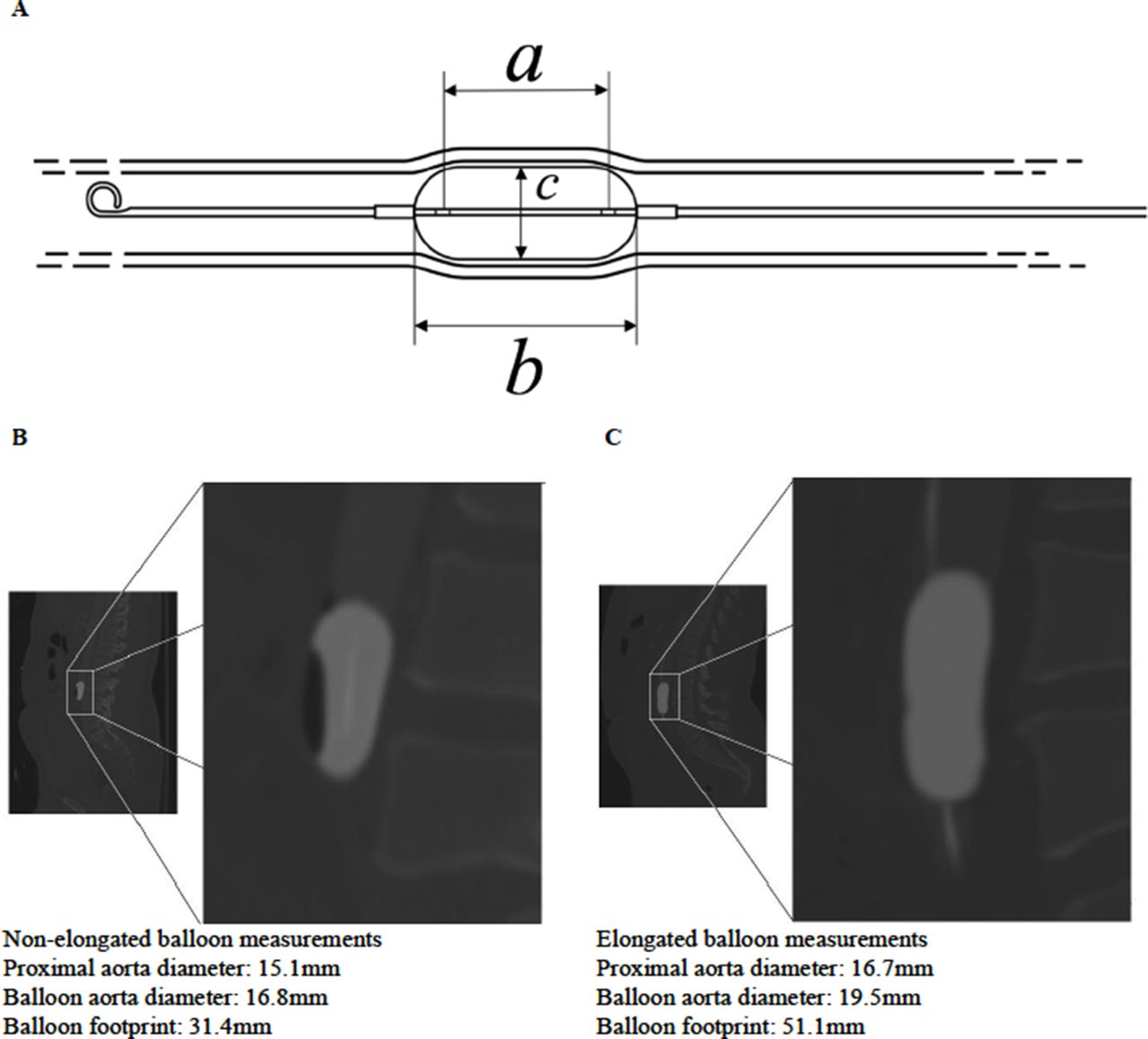
(A) Line drawing of an ER-REBOA catheter. Length ‘a’ is the intended working length, between radio-opaque markers, which is normally up to 37 mm. Length ‘b’ is the entire length of the balloon, including the ‘shoulders’, which are not intended to be in apposition with the vessel wall. Length ‘c’ is the diameter of the balloon. (B) Zone 3 resuscitative endovascular balloon occlusion of the aorta (REBOA) demonstrating appropriate balloon inflation. Note: rounded shoulders and a footprint of 31.4 mm, well within the intended working length of 37 mm. (C) Zone 3 REBOA demonstrating overinflation and elongation, with a balloon footprint of 51.1 mm. Same scale as (B).
The distance from the radio-opaque marker to balloon catheter attachment is called the ‘balloon shoulder’. Once the balloon is sufficiently inflated to encounter radial resistance, the balloon will expand on its long axis, termed elongation. An example of this phenomenon is illustrated in figure 1B,C, where CT images of an appropriately inflated balloon is compared with an overinflated balloon. These CT images were obtained in patients during full aortic occlusion by REBOA which has been previously described.18 The key point is that figure 1C demonstrates loss of shouldering which potentially places the aorta at risk of injury. Importantly, deliberate overinflation is unnecessary to achieve large vessel occlusion.
The magnitude in which the balloon is deformed in the circumferential and longitudinal planes is dependent on the compliant characteristics of the balloon and the resistance to stretching provided by the vessel. The deformational properties of the balloon can be defined by measuring the circumferential and longitudinal compliance quotients, which can be defined as:

Experimental design
After aortic harvest, sections of the thoracic and infrarenal aorta were excised, which were at least 7 cm in length. The aortic segments were harvested after humane euthanasia of swine used in an IACUC-approved research protocol and in conformation with the aims of the three Rs (replace, reduce, refine) in animal research. The aortic tissue was stored in normal saline to prevent desiccation. All aortic sections were tested within 2 hours of euthanasia. Prior to any instrumentation, baseline measurements of aortic diameter were obtained. An ER-REBOA catheter was inserted into the lumen and the balloon inflated with 0.9% saline until full occlusion of the vessel was achieved based on direct visualization.
Having achieved occlusion, serial aortic diameters (mm) were recorded, with measurements taken every 2 mL to 4 mL of saline instilled into the balloon, to the maximum volume of 24 mL (per manufactures instructions).19 Balloon elongation was calculated by measuring the balloon footprint on the aorta (the longitudinal length of the aorta where there was diameter expansion secondary to balloon inflation) for each inflation point. Measurements were obtained with a digital caliper (Apex Tool Group, Sparks MD, USA; measuring range: 150 mm; accuracy: ±0.02 mm).
Endpoints and statistical analysis
The primary endpoint of this study was aortic failure, which was defined as visualization of the balloon material through a defect in the vessel wall. Data on the two groups (ruptured vs unruptured) were compared using an unpaired two-sample t-test. Secondary endpoints included a quantification of the relationship between aortic diameter and the circumferential stretch ratio, circumferential and longitudinal compliance ratio. This was assessed using linear regression with an R2 value used to report the strength of the relationship. Statistical significance was defined as a P value of 0.05 or less and the analysis was performed using GraphPad Prism.
Results
Baseline characteristics
Fresh aortas were obtained from six female swine. The mean±SD weight (kg) of the swine was 81.6±5.2. In total, 14 unique sections of aorta were harvested for inclusion in the study. The mean±SD baseline aortic diameter (mm) was 14.2±3.4, with a range of 7.6–18.1.
Comparison of aortic diameters and rupture
Out of the 14 sections of aorta tested, aortic rupture occurred in three. The volume (mL) instilled in the balloons at the points of aortic rupture were 11, 12 and 14. As seen in figure 2, aortic rupture was uniformly in a longitudinal direction. The mean baseline diameters of the aortic segments that were ruptured were significantly smaller than those that did not rupture (8.9±1.2 vs 15.6±1.9; P<0.001). Intimal disruption was not observed macroscopically in aortic segments that did not rupture after balloon inflation. In addition, as seen in figure 3, the maximal circumferential stretch ratios accomplished were significantly higher in the aortic segments that ruptured compared with those that did not (1.86±0.12 vs 1.53±0.09; P<0.001). Furthermore, the relationship between aortic diameter and stretch ratio was linear (R2=0.72; P<0.001). Of note, there were no instances in which the balloon ruptured.
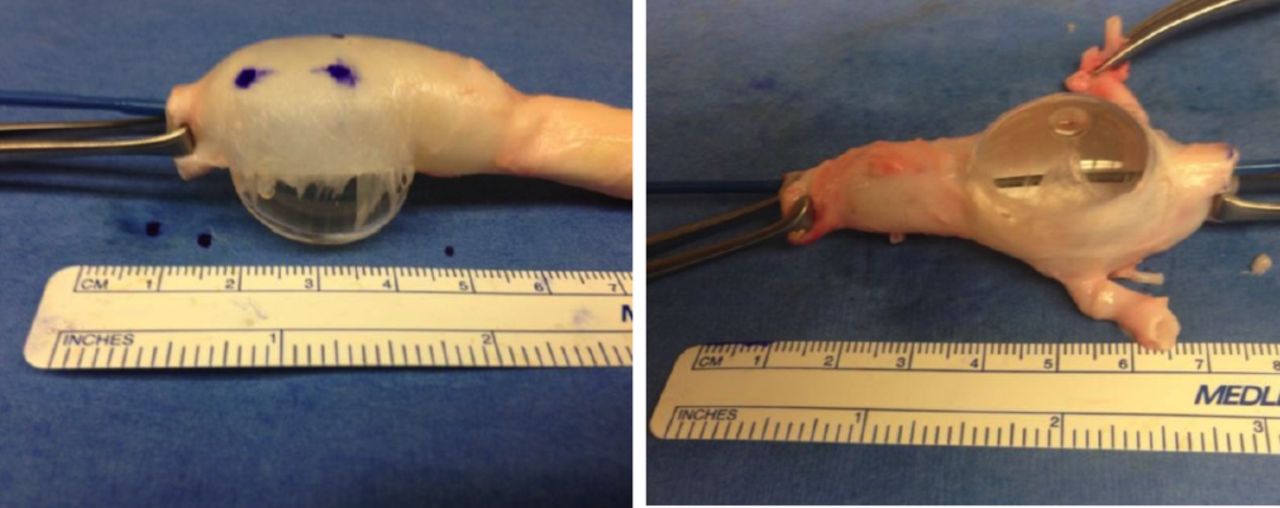
Two images demonstrating the propensity for the aorta to rupture in the longitudinal direction.

Maximal circumferential stretch ratios compared with baseline aortic diameter. Linear regression, R2=0.72; P<0.001.
Comparison of axial and circumferential compliance and aortic diameters
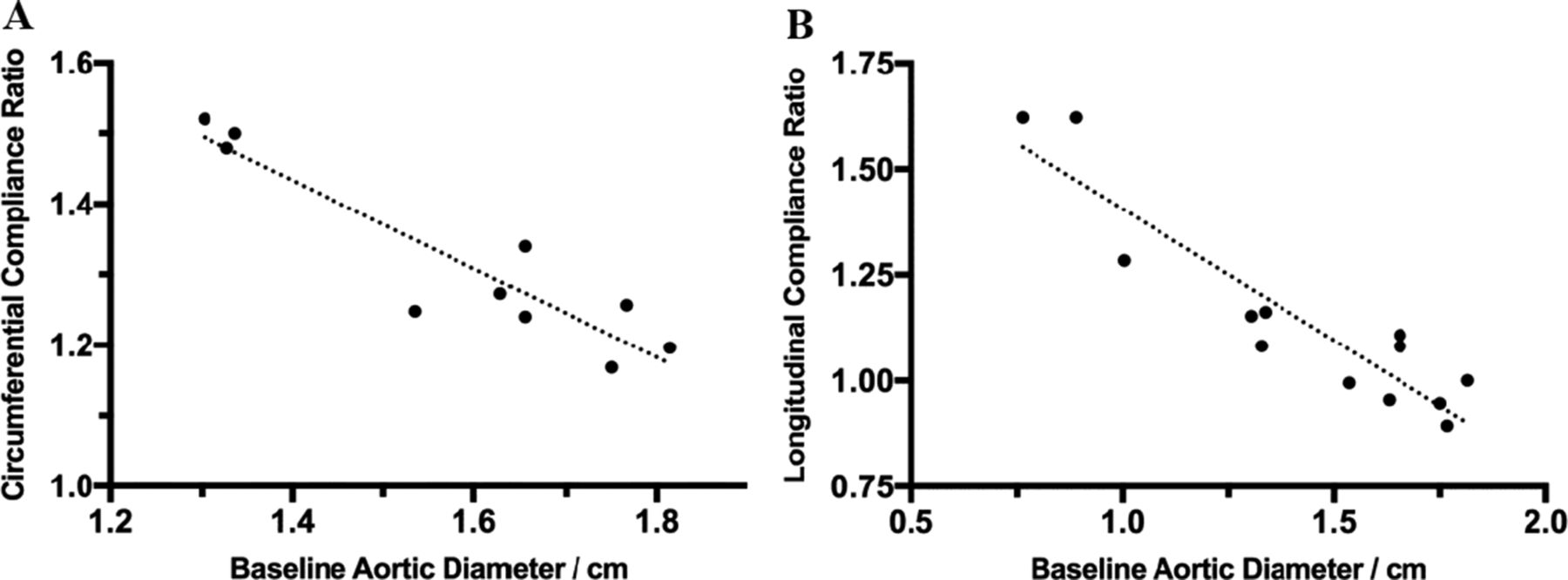
The balloon was able to be fully inflated (24 mL) in 10 aortic segments. For those segments, the circumferential compliance quotient was inversely proportional to the aortic diameter, as seen in figure 4A (R2=0.85; P<0.001). A higher circumferential compliance quotient resulted in greater longitudinal expansion (elongation). Similarly, the longitudinal compliance quotient was inversely proportional to the aortic diameter, as seen in figure 4B (R2=0.85; P<0.001). The maximum amount of balloon elongation measured was 80 mm.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Circumferential compliance ratio compared to aortic diameter at maximum balloon inflation (24 mL, expected balloon diameter is 32 mm). R2=0.85. (B) Longitudinal compliance ratio compared with aortic diameter when balloon is inflated with 8 mL (expected balloon diameter is 20 mm). R2=0.85.
Discussion
The current study is the first characterization of aortic failure in the context of endovascular balloon occlusion. When using large diameter, compliant balloons, the aorta is at greatest risk of failure at smaller diameters. Furthermore, balloon elongation is a feature of an overinflated balloon, which can substantially increase the balloon footprint, potentially exceeding the landing zone or risking aortic failure. These findings have important implications for the use of REBOA in hemorrhage control, especially when using a blind inflation technique.
Previous investigators have sought to examine the failure threshold of arteries using single and dual-directional loading. These studies have largely focused on understanding tissue mechanics in relation to atherosclerotic plaque or aneurysmal disease.14 20-23 Interestingly, despite a different focus and methodology, several investigators agree with the findings of the current study.
The oldest examination of aortic failure was performed by Mohan and Melvin in 1982.23 Those investigators examined 31 autopsy obtained aortas in ages ranging between 4 and 89 years of age. They performed uniaxial tension tests and demonstrated that, for patients less than 60 years old, the mean (±SD) circumferential stretch ratio before aortic failure was 1.73±0.22.23
More recently, Chen et al 20 examined the microscopic behavior of collagen and elastin fibers in porcine coronary arteries. That group demonstrated that collagen and elastin fibers become maximally aligned at a circumferential stretch ratio of 1.8,20 suggesting that this stretch ratio is the upper limit of vessel distention. Teng et al 21 examined human atherosclerotic arteries and demonstrated a stretch ratio failure point of around 1.7. In the current study, all three aortic failures occurred around a stretch ratio of 1.8, suggesting that aortic tissue has a failure threshold around this point.
Although many of these findings may be obvious, the objective description of a failure threshold applies a useful quantitative measure that can be used to enhance procedural safety, either by training or improved catheter design. The proponents of blind REBOA inflation need to be aware of the current study findings as there are clear clinical implications.
First, the current study has shown that overinflation results in significant balloon elongation beyond its normal working length. This is accentuated in smaller caliber vessels, for example, when the balloon was inflated with 20 mL in a 14.3 mm aorta, it resulted in an elongation length of 80 mm (normal of 37 mm). In human patients, the infrarenal (zone 3) balloon landing zone can range from 6.3 cm to 12.3 cm in adults.24 Clinically, an expanded balloon footprint could encroach on the renal ostia, inducing an ischemic injury.
Second, the relationship between aortic diameter and rupture risk allows for the identification of ‘high-risk’ groups where special care must be taken during inflation. Women, children, young adults and smaller vessels such as the iliac artery are all at risk.3 11 25-27
To illustrate, if an ER-REBOA catheter were to be inflated in an 18 mm artery with its maximal volume of 24 mL, it would be at risk of attaining or exceeding a circumferential stretch ratio of 1.8. In a population-based study determining the average size of vessels in differing age groups,25 this threshold of patients at high risk includes patients age <30 years old undergoing distal zone 1 REBOA, patients age <80 years old undergoing zone 3 REBOA and all patients undergoing iliac artery occlusion.
The inherent risks associated with blind balloon inflation may be minimized through education, increased utilization of imaging where feasible and improvements in catheter design. Performing adequate balloon occlusion has been taught through the use of haptic feedback28 29; however, this is poorly defined. Given the smaller profile of newer catheters, haptic feedback may largely represent the intrinsic resistance within the balloon inflation lumen, rather than from actual balloon compliance. Improvements in catheter design and technology, such as the use of pressure monitors, pressure pop-off valves and alternative inflation mediums, may increase blind inflation safety.
In addition, depending on aortic location and patient demographic, guidelines for approximate volume/diameter to be inflated are helpful. In fact, the Joint Trauma System Clinical Practice Guidelines30 recommends that approximately 8 mL and 3 mL be used for balloon inflation for zones 1 and 3, respectively, followed by incremental adjustments. This could be used in conjunction with arterial line monitoring demonstrating an improvement in hemodynamics, as well as utilization of imaging to confirm adequate occlusion. We have incorporated these considerations into our practice patterns and have also assimilated these findings within our REBOA teaching course, the BEST course.28
This study has several limitations. The current study examined a relatively small number of aortas with a limited range of vessel diameters, which largely relates to the phylogenetic differences between swine and humans. Despite a similar body weight, swine do have a smaller aorta than human subjects. Importantly though, the current study and literature suggest that the greatest issues are encountered in smaller vessels. Additional study with a higher power and a wider range of aortic diameters would be helpful in defining a more precise circumferential stretch failure threshold.
The current study deliberately does not report histological examination, because the ex vivo nature of the current model may affect how the tissue responds to balloon occlusion on a microscopic level. Furthermore, the interaction of the balloon–arterial wall interface may also be different in vitro compared with an in vivo model.
These limitations should be taken into consideration when applying the study’s findings to future catheter design, especially regarding the generalizability of the findings of the directionality of aortic rupture. Lastly, only one catheter type was tested in this study, and it is unclear whether or not other balloon catheters of differing specifications would result in similar results given the anisotropic nature of the aorta.
Conclusions
Inflation of aortic balloon catheters carries an inherent risk of aortic injury, which may be minimized through an understanding of the intrinsic characteristics of the aorta and compliant balloons. Smaller diameter aortic segments undergoing overinflation, particularly beyond a circumferential stretch ratio of 1.8, are at risk of aortic rupture. Further study using human aortic tissue is warranted to assess the clinical translation of these findings.
References
Footnotes
Contributors PJW was involved in the acquisition of data. PJW and JJM did the analysis and interpretation of data and also drafted the manuscript. All the authors equally contributed to the study conception and design and critical revision of the manuscript.
Funding This study was funded in part by a grant from the Department of Defense; grant number W81XWH-16-1-0116.
Competing interests JJM and MLB are clinical advisory board members for Prytime Medical Inc.
Provenance and peer review Not commissioned; externally peer reviewed.