Article Text

Abstract
As general surgery trainees continue to enter specialty practice at a high rate, fewer and fewer are caring for emergency general surgery (EGS) patients. Thus EGS has become one of the cornerstones of the practice of acute care surgery. With the centralization of this area of surgical care in many areas of the country, a clear understanding of the issues associated with this becomes vital. Understanding the public health implications with respect to burden of care and cost will allow for appropriate planning and resource allocation in the future. In addition, the development of validated severity modeling will help with risk stratification in future study of these diseases.
- emergency general surgery
- burden of disease
- risk-adjustment
- public health
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Emergency general surgery (EGS) has long been considered to be a large portion of ‘bread and butter’ general surgical practice, but this is not borne out in analysis of graduates finishing general surgical residency in the 21st century. Roughly 80% of finishing residents pursue specialized fellowship training, which leads to specialty-specific practice patterns.1 This produces surgeons who are uncomfortable caring for emergencies outside their area of specialization in many cases. Although there are certainly a multitude of reasons for this shift in training, it leaves patients with emergency general surgical problems with fewer and fewer surgeons who are skilled in providing the type of care needed.
In addition, there is a worsening shortage of physicians, and one source estimates that there will be a gap of 41 000 by 2025 between the number of practicing general surgeons and the number needed to cover the needs of the general surgical patient population.2 These and other issues have combined to cause the Institute of Medicine in their often quoted publication from 2006 to declare that we are facing a crisis in emergency care in the USA.3
These are some of the underlying forces that led the American Association for the Surgery of Trauma (AAST) to create the specialty of acute care surgery. Acute care surgery includes trauma, surgical critical care, and EGS at its core. The AAST Acute Care Surgery Committee has gone on to establish acute care surgery as a specialty with its own curriculum, site visits to ensure program requirements are met, and a certificate of completion. There are 20 accredited fellowship programs currently and more are planned.
Although EGS has been contained within general surgical practice for many years, the development of acute care surgery highlights this area of surgery as its own area of practice. Its separation from daily surgical practice in many centers has created the need to carefully study the burden of the diseases that constitute EGS and determine the resources needed to best care for these patients under this paradigm. Additionally, the desire to optimize outcomes has created the need to understand and quantify severity of disease as it relates to resource utilization, care algorithms, and outcome.
EGS definition
To examine overall burden of disease or begin to develop severity scoring systems, one must first have a definition of EGS. In 2012, the AAST Committee on Severity Assessment and Outcomes set out to develop such a definition.4 They began by defining an EGS patient as any patient (inpatient or emergency department) requiring an emergency surgical evaluation (operative or non-operative) for diseases within the realm of general surgery as defined by the American Board of Surgery. Both operative and non-operative patients are included as there are many emergencies that may require surgical evaluation without operative interventions, such as diverticulitis, pancreatitis, or even appendicitis in certain cases. To further refine the disease processes that make up EGS, the committee pooled International Classification of Diseases-9th Rev. (ICD-9) codes of surgeons from seven institutions for the previous 5 years. Primary diagnoses only were included. Codes 800–999 (trauma) were excluded, as were critical care codes. A modified Delphi methodology was used to review 621 codes, and 309 were finally selected as EGS diagnoses. This subset of diagnoses has been used extensively in subsequent publications and data sets evaluating overall burden of disease on a national level.
Burden of disease
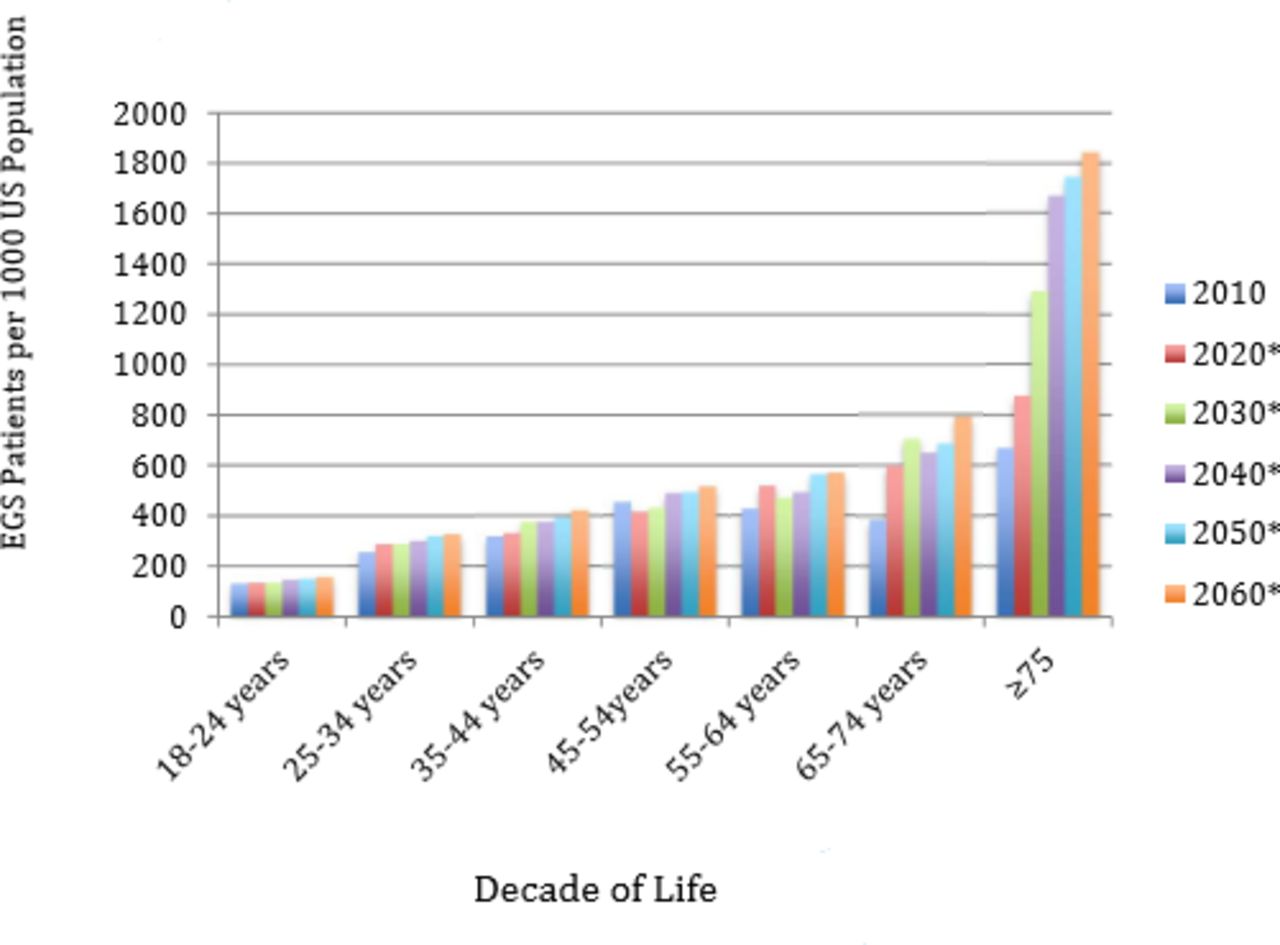
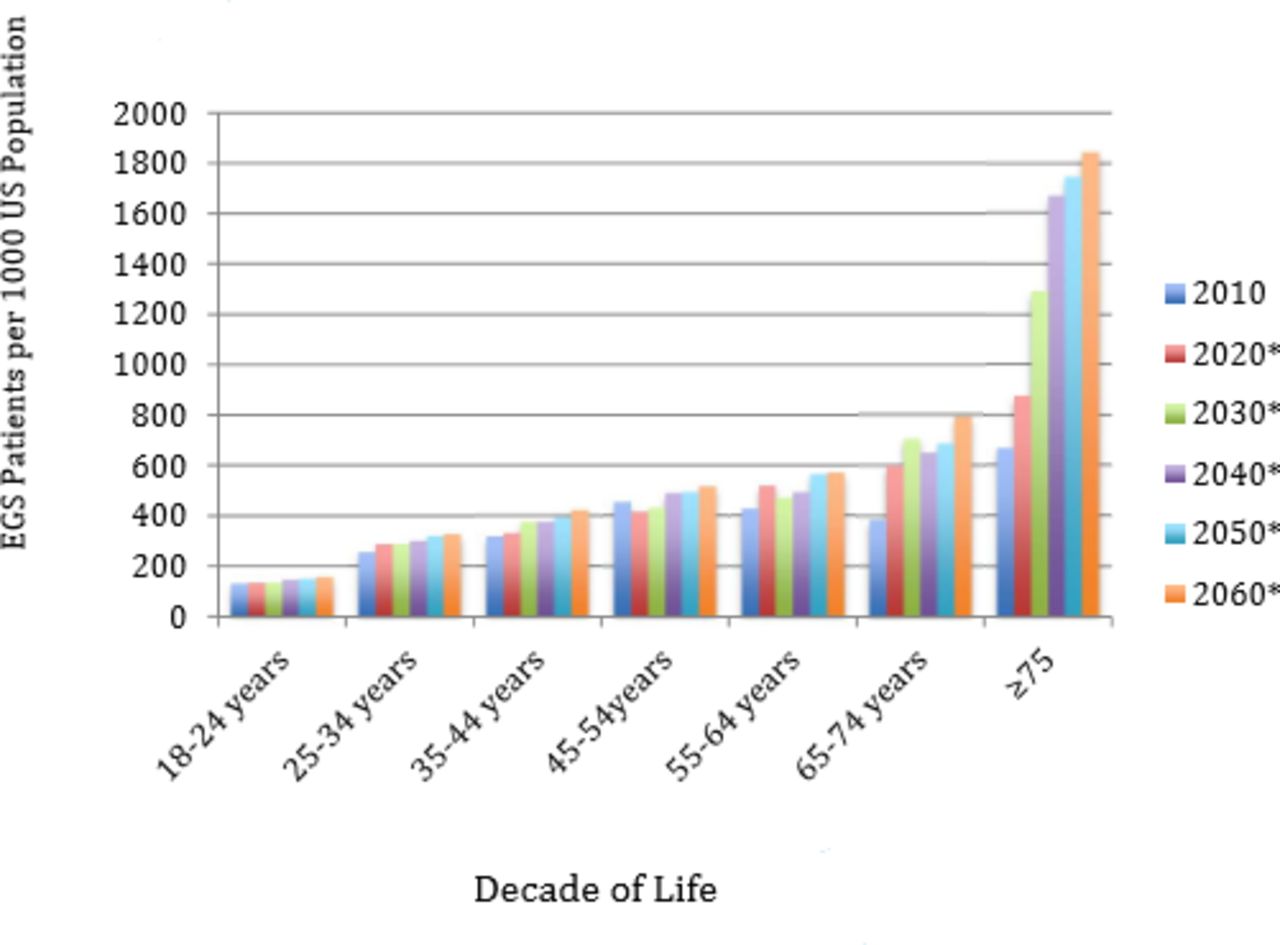
As EGS further differentiates into its own area of practice, the overall burden of disease becomes an important issue to attempt to understand. The first focused examination of this was published again in 2012 in which the 2009 National Inpatient Sample (NIS) was queried for patients whose primary diagnosis matched one of the ICD-9 codes defined as EGS diagnoses. This yielded an estimated 4 005 935 patients nationwide with such a diagnosis. Of these 2 344 576 were admitted as emergencies. As a point of comparison, during the same time period, approximately 1.75 million new cases of diabetes mellitus were diagnosed.4 This work was expanded by Gale et al 5 in 2014 using a larger cross-section of the NIS (2001–2010). During this time period over 27 million patients were admitted to US hospitals with primary EGS diagnoses, comprising 7.12% of all hospital admissions. Over 25% of this cohort required operative intervention. When examined by year, the number of EGS admission increased steadily from 2.38 million in 2001 to 3.03 million in 2010. This volume outstrips the 2.3 million trauma admissions/year nationwide based on 2014 CDC data. This amounts to 1290/100 000 of total population (as compared with 899/100 000 cases of new diabetes mellitus or 650/100 000 new cancer diagnoses). In 2015 Ogola et al 6 used the 2010 NIS and expected population growth to project EGS population out to 2060. This is represented in figure 1. Based on these estimates, EGS resource utilization is expected to expand significantly as the population ages and grows.
{kind=link}
Projected growth in the EGS population through 2060.6 *Represents projected patients based on current estimates. EGS, emergency general surgery.
Within the 309 diagnoses that constitute EGS practice, 7 groups of diagnoses have been shown to be responsible for the large majority of procedures, cost, complications, and mortality. In 2016, Scott et al 7 used the 2009–2011 NIS data to demonstrate that the diagnoses groups of partial colectomy, small bowel resection, cholecystectomy, operative management of peptic ulcer disease, lysis of peritoneal adhesions, appendectomy, and laparotomy account for 80.0% of procedures, 80.3% of deaths, 78.9% of complications, and 80.2% of inpatient costs in the USA.
The prevalence and severity of EGS-driven hospitalizations present a significant public health cost burden. The total estimated cost of EGS hospitalizations in 2010 was $28.4 billion, and this is expected to nearly double by 2060.6 This NIS-based estimate does not include provider costs or costs of care outside the hospital. Thus EGS is the most expensive cause of emergency hospitalization in the USA as compared with other common conditions including trauma, myocardial infarction, congestive heart failure ,chronic obstructive pulmonary disease, and diabetes mellitus. In an analysis of the Maryland Health Services Cost Review Commission database from 2009 to 2013, which contains discharge information on all hospital admissions, Narayan et al 8 found that almost 14% of admission were EGS admissions, with overall charges of over $3.8 billion. Available data also demonstrate that 56% of EGS admissions between 2001 and 2010 carried Medicare/Medicaid, whereas roughly 10% were uninsured.5
Severity stratification
Given that EGS represents a substantial portion of patients requiring treatment at US hospitals, development of reliable measures of severity is vital. Such tools would allow for accurate and consistent study of EGS diseases, assessment of impact of disease severity on outcomes, and a clear understanding of the relationship between resource need and disease severity. Some EGS diseases have one or more severity scales already associated with them (pancreatitis, diverticulitis), but many do not.
The AAST Committee on Severity Assessment and Outcomes has developed a scaling system for anatomic severity of disease that can be applied uniformly across all EGS disease states.9 Such a system serves an essential role in comparing patient populations for risk adjustment purposes, clinical trials, and estimation of patient prognosis. This schema follows disease progression with grade I-minimal to grade V-severe. Grade I is classified as local disease confined to the organ with minimal abnormality; grade II is local disease confined to the organ with severe abnormality; grade III is local extension beyond the organ; grade IV is regional extension beyond the organ; and grade V is widespread extension beyond the organ. These principles were used to define grades for 16 common EGS conditions (acute appendicitis, breast infections, acute cholecystitis, acute diverticulitis of the colon, esophageal perforation, hernias (internal or abdominal wall), infectious colitis, intestinal obstruction, intestinal arterial ischemia, acute pancreatitis, pelvic inflammatory disease, perirectal abscess, perforated peptic ulcer, pleural space infection, soft tissue infections, and surgical site infections).10
This concept has since been validated in several EGS disease states and performs well based on available data. The diverticulitis scale was recently examined in a multicenter trial.11 The system showed good inter-rater reliability as well as a clear association of increasing score with worse outcome and higher resource consumption. Similar work looking at the AAST grading scale for appendicitis has shown strong correlation between AAST severity grade assigned by preoperative cross-sectional imaging and intraoperative findings.12 AAST severity grade also correlated well with outcomes in this study.
Although this method of grading appears to carry utility, additional information needed to develop a comprehensive prediction of outcome likely includes age, comorbidities, and physiologic state. Uniform tools including these types of variables for outcome prediction applicable to all EGS diseases have not been developed, but available data make it clear that the outcomes in EGS patients are generally worse than patients undergoing similar operations under elective conditions. Early data show that the ACS National Surgical Quality Improvememnt Program Surgical Risk Calculator may fill this niche as it appears to predict outcome well in the EGS population.
EGS continues to grow and consolidate as an area of practice within the specialty of acute care surgery. This has led to investigators becoming interested in understanding the impact of EGS within the overall care of patients in the USA. Subsequent studies make it clear that EGS diseases constitute a significant portion of urgent and emergent care in our healthcare system, outstripping problems such as trauma care, newly diagnosed diabetes, and newly diagnosed cancer in volume on an annual basis. Such large volume is naturally accompanied by significant cost, making EGS an important public health issue. Continued work as to the impact of EGS on different sectors of healthcare as well as development of accurate, validated severity measures will allow for planning for the optimum care of these patients as we move forward. Although the answers to some of these questions are not yet apparent, the successes of the trauma care community in building systems and implementing care protocols in the past decades may serve as a model that deserves examination.
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.