Article Text

Abstract
Objectives Patients with health literacy (HL) disparities are less likely to comprehend hospital discharge instructions and less satisfied with physician communication. In this prospective cohort study, we sought to examine the interaction of HL, physician communication, and quality of life after hospital discharge among postoperative emergency surgery and trauma patients.
Methods Emergency surgery and trauma surgery patients were prospectively enrolled between December 2020 and December 2021 at an urban level 1 trauma center. Newest Vital Sign (NVS) instrument was used to measure HL during hospitalization. After discharge, patients were administered Revised Trauma Quality of Life (RT-QOL) and Interpersonal Processes of Care (IPC) instruments. An adjusted regression model was used to determine associations among NVS the emotional well-being subscale on the RT-QOL, and patient perception of physician compassion and respect on the IPC.
Results 94 patients completed all instruments. HL was proficient (high HL) in 59.6% and less than proficient (low HL) in 40.4%. HL was positively associated with RT-QOL emotional well-being, r(94)=0.212, p=0.040. However, higher rating of surgeon compassion and respect on IPC moderated the relationship between HL and emotional well-being such that patients with low HL and high perception of physician compassion and respect had similar emotional well-being as the high HL group (p=0.042).
Conclusion Favorable patient perception of surgeon compassion and respect was correlated with higher emotional well-being, independent of HL proficiency. Although the allocation of resources toward improving HL disparities remains warranted, improving patient perception of caregiver compassion during hospitalization may be a target of opportunity with respect to improving quality of life after hospital discharge.
Level of evidence Level III.
- Health literacy
- patient reported outcome measures
- Healthcare disparities
Data availability statement
Data are available upon reasonable request. Data will be made available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Health literacy (HL) disparities have shown to be associated with decreased quality of life; however, this research has not considered the potential impact of the patient–physician relationship.
WHAT THIS STUDY ADDS
In this study, patient HL and surgeon compassion were measured during hospitalization and emotional well-being after discharge. Surgeon compassion was associated with higher emotional well-being, independent of HL proficiency.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study highlights an opportunity to focus on physician compassion during hospitalization as a precursor to improved patient emotional quality of life after hospitalization.
Objectives
Prior studies have investigated the relationship between health literacy (HL) and quality of life (QOL), and although some studies demonstrated a positive association between HL and QOL, this finding has not been consistently validated across all studies.1–5 In prior work from our own institution, we found that patients with less than adequate HL were relatively less satisfied with the physician communication they experienced during hospitalization.6 We also identified, in a follow-up study, that HL proficiency among trauma inpatients predicted ability to comprehend instructions after hospital discharge.7 We did not, however, evaluate the influence of either HL proficiency or perception of physician communication on postdischarge QOL.
Recently, Herrera-Escobar et al developed and subsequently validated a trauma-specific QOL instrument (Revised Trauma Quality of Life, RT-QOL).8 This instrument is an 18-question survey that generates composite scores for three domains: emotional well-being, functional engagement, and physical well-being and recovery. To our knowledge, the association between HL and this specific patient population had not been studied. We sought to evaluate the relationship between HL assessed during hospitalization and postdischarge RT-QOL results. In addition, we evaluated the interaction between HL and perception of physician communication on QOL after hospital discharge. We hypothesized that RT-QOL scores would be positively associated with both HL proficiency and positive perception of physician communication during hospitalization.
Methods
The methodology for this project builds on previous work conducted at St Joseph’s Hospital and Medical Center in Phoenix, Arizona.6 7 Patients admitted from the emergency department to either the trauma service or emergency general surgery service were approached for enrollment.
Inclusion criteria were as follows: patients who underwent an operation with general anesthesia, were 18 years or older, English speaking, agreeing to postdischarge follow-up, and discharged home. Exclusion criteria were as follows: patients not alert and oriented to place, person, and time, or otherwise unable to communicate as a result of either injuries or baseline cognitive status. In addition, patients with unplanned readmission or death prior to follow-up were excluded.
After consent, patients were administered three survey instruments. Newest Vital Sign (NVS),9 an assessment of HL proficiency, was administered once the patient was ready for hospital discharge. Short-Form Interpersonal Processes of Care (SF-IPC) was also administered at this time.10 RT-QOL survey was administered by telephone approximately 1 month after hospital discharge.
NVS comprises an exercise in which patients are asked to interpret a nutrition label and is used as a proxy for HL.9 The NVS was scored as defined in the publication; scores ranging from 0 to 6 and were dichotomized at 0–2 reflecting inadequate HL and 3–6 to reflect adequate HL. The 18-item SF-IPC survey is a validated measure of patient satisfaction with quality of interpersonal communication and contains seven composite-scored domains: general clarity, elicitation and responsiveness to concerns, explanation of the condition and results, decision-making, compassion and respect, lack of discrimination by race/ethnicity, and staff respect.10 Each domain comprises two to three questions, with responses scored on a 5-point Likert scale. This scale was dichotomized to a score of 5 reflecting the patient always thought positively about the specific question versus scores of 1–4 indicating less than always. RT-QOL is an 18-item survey. Items are scored on a 1–5 Likert scale. Composite scores for each of the instrument’s three domains were calculated (emotional well-being, functional engagement, and physical well-being and recovery).8
Other variables that were collected as part of this study included patient demographics, hospital length of stay, and diagnostic-related group (DRG) weight. DRG weight is an estimation of hospital resources required to treat a case within a specific DRG relative to other DRGs.
Statistical analysis
The cohort was described using counts with percentages, means±SDs, or medians with 25th–75th percentiles, as appropriate. Spearman correlations were used to assess the association between survey constructs. Group means were compared using independent samples t-tests, or independent samples median tests as a non-parametric option. Categorical variables were compared between the adequate and inadequate health literate groups using the χ2 or Fisher’s exact statistic. A logistic regression analysis adjusted for patient age, race, DRG weight, and payer was used to evaluate the association between HL, patient perception of physician compassion and respect with emotional well-being.
An interaction term was created to test the association between adequate HL and high physician compassion/respect. Covariates were chosen based on their association with HL and clinical judgement. No attempt was made to address missing data through imputation. Statistical analyses were performed using SPSS V.27.
Results
Two hundred surgery patients consented to participate in the study and follow-up was obtained on 94. There was not a significant difference between the group with versus without follow-up based on age (p=0.214), sex (p=0.053), or education level (p=0.214). The distribution of race/ethnicity was different from expected with fewer American Indians/Alaska Natives based on the χ2 distribution (p=0.012, standardized residual −2.1). In our study cohort of 94 patients, 43 (45.7%) were male with an average age of 45.5±16.5 years (table 1). Ninety-four (50%) of patients attended some college or beyond. The majority of patients were government insured (62.8%). Twenty-three (24.5%) patients had a minimum of one comorbidity. The most frequent comorbidities were substance abuse disorder (13, 13.9%), hypertension (8, 8.5%), smoking (5, 5.3%), and diabetes mellitus (4, 4.3%). 37.2% (n=35) were admitted to the trauma service and 62.8% (n=59) were admitted to the emergency general surgery service. Trauma and emergency patients were considered together as there were not statistically significant differences between groups in patient age (p=0.761), education (p=0.748), HL score (p=0.259), or hospital length of stay (p=0.279).
Patient demographics and injury characteristics
Fifty-six (59.6%) of patients scored adequate or better in HL as measured by a score of 4–6 on the NVS (table 1). Two (2.1%) patients scored 0 points and 20 (21.3%) scored a perfect 6. The patient perception of physician compassion and respect scale was dichotomized to a score of 5 reflecting the patient always thought the physician treated them with compassion and respect versus scores of 1–4 indicating less than always. The mean emotional well-being score at 1 month after discharge was 3.7±0.9, just higher than the midpoint on the 5-point scale. The minimum score was 1.5, scored by 1 (1.5%) patient, and the maximum 5 was scored by 10 (10.6%) patients.
A comparison between the adequate versus inadequate literacy groups is shown in table 2. The inadequate group was significantly older (p=0.005) with a higher proportion of government payers (p=0.008). There was not a statistically significant difference in length of stay, sex, race, or DRG weight. Education was considered ordinally and was not associated with HL proficiency (p=0.192). The percentage of maximum (5/5) scores across the seven IPC domains was similar between the deficient and proficient HL groups. There were also no differences between the average RT-QOL scores between the deficient and proficient HL groups. However, HL was positively correlated with RT-QOL emotional well-being, r(94)=0.212, p=0.040. HL was not correlated with either functional engagement (p=0.712) or physical well-being/recovery (p=0.085).
Comparison of demographics and outcomes by health literacy proficiency
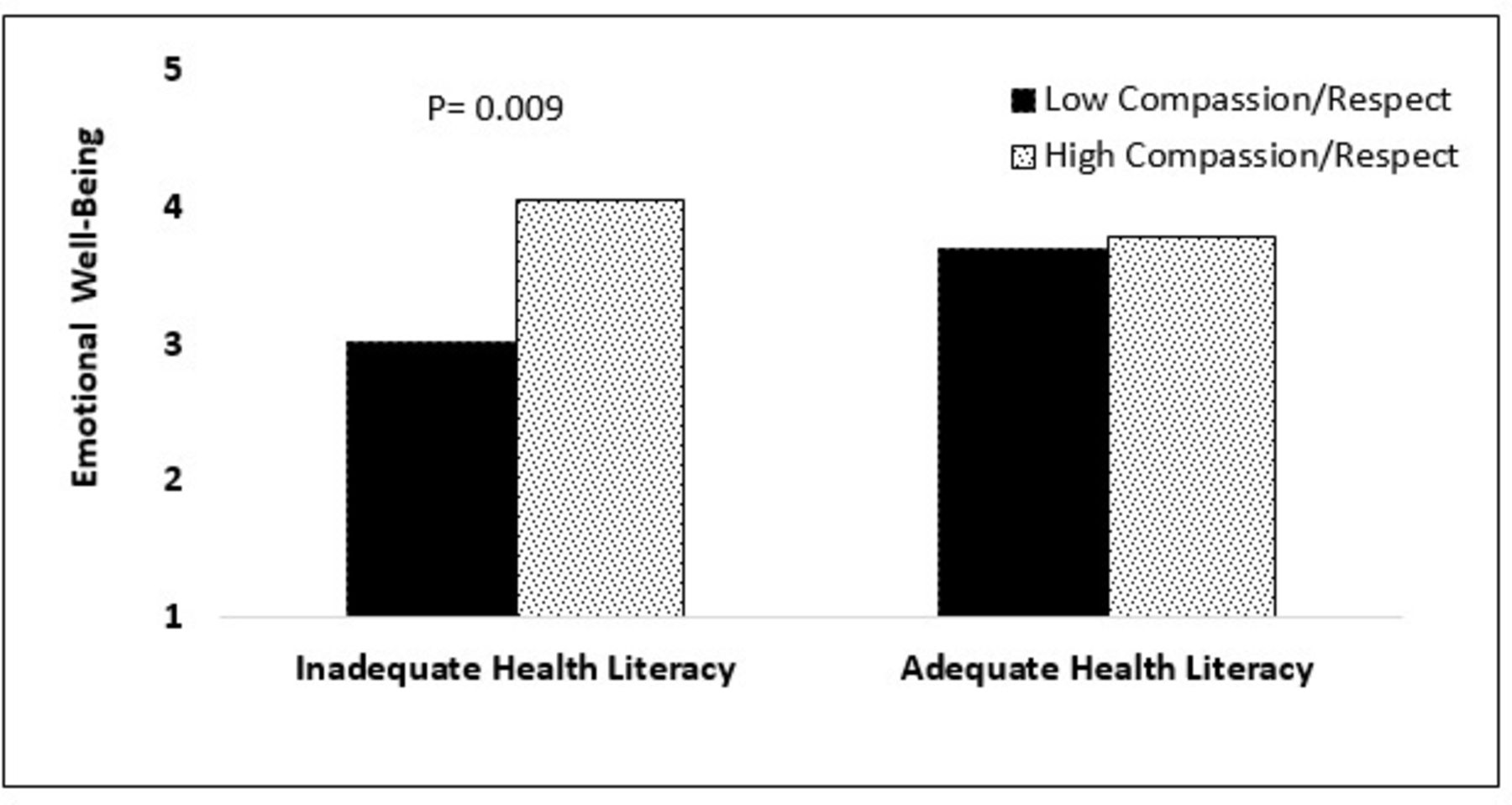
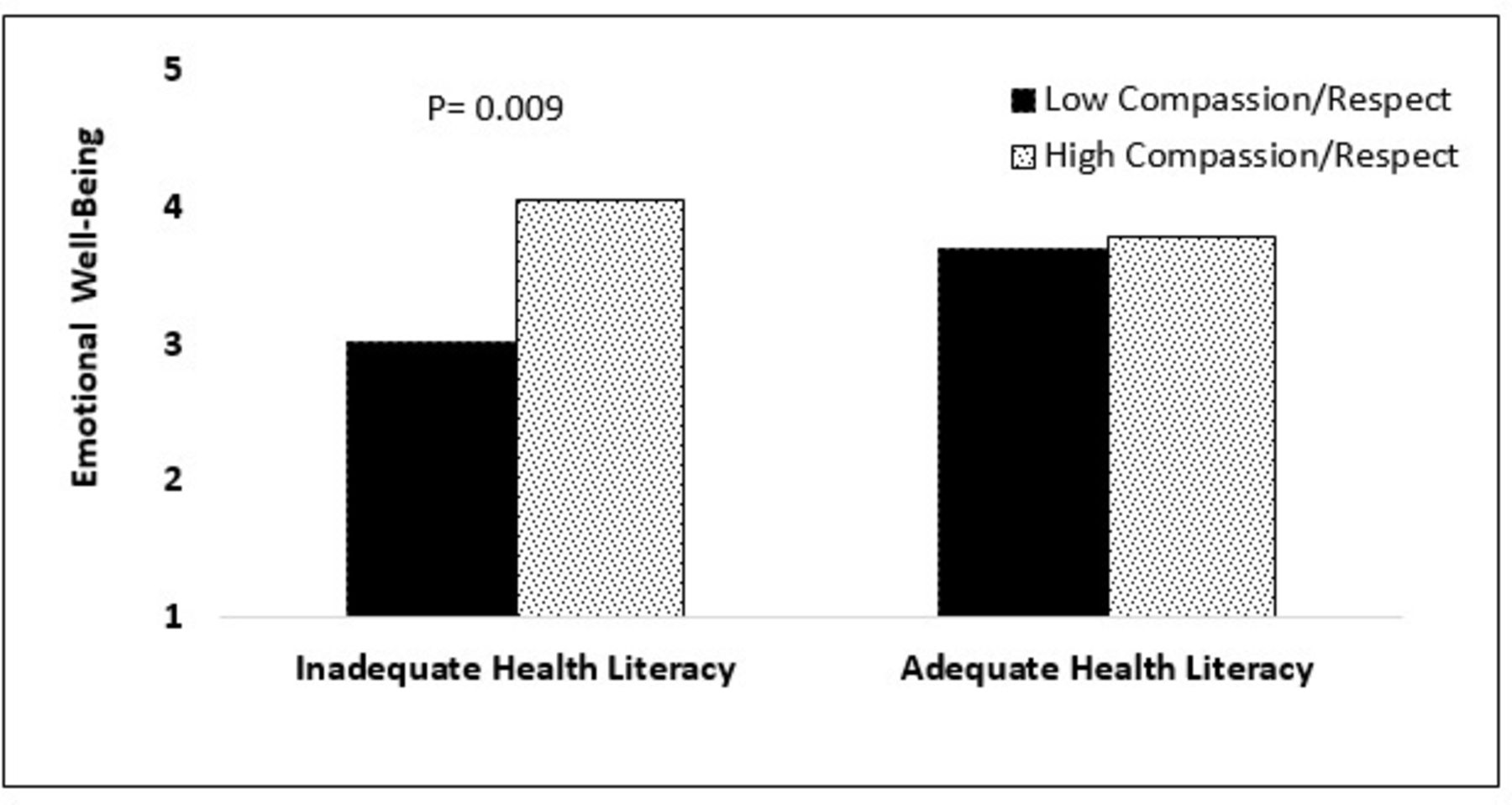
A multivariate model was used to further evaluate the association among RT-QOL emotional well-being domain, HL proficiency, and the IPC domain physician compassion and respect. Model selection was based on p values <0.15 in table 2. DRG weight was not statistically different between HL groups; however, it was found to be significantly correlated with emotional well-being (r(94)=−0.257, p=0.013) and was added to the multivariate model. Covariates included age, education level in years, race/ethnicity, DRG weight, and payer. There were no significant covariates (table 3). A main effect emerged for patient report of physician compassion and respect (p<0.001) but not for HL (p=0.992). However, an interaction between HL and physician compassion was present (p=0.009). Post hoc comparisons with Bonferroni adjustment revealed no mean difference for low versus high compassion and respect within the proficient HL group (p=1.00); however, higher emotional well-being for patients with deficient HL who perceived their physician to have high compassion and respect was observed (p=0.001; figure 1). Further modeling was performed to evaluate the remaining IPC domains and no significant associations were observed.
Summary of multivariate regression model predicting emotional well-being
{kind=link}
Interaction between physician compassion and respect and health literacy.
Discussion
Deficient HL is prevalent in the USA, affecting nearly 40% of the adult population.11 In the current study, it is notable that we identified deficient HL in 40% of our study patients. Patients with deficient HL often have a limited knowledge of self-management skills and greater difficulty understanding prescription drug labels, contributing to high rates of non-adherence to treatment, emergency department visits, and hospital readmissions.11–16
The relationship between HL proficiency and postdischarge QOL among patients hospitalized for injury or emergency surgery has not been extensively evaluated. Prior studies of the relationship between QOL and HL have demonstrated inconsistent results.17 This may be attributable to relatively small sample sizes (usually a few hundred patients) and use of different instruments to assess both HL and QOL. In the current study, we have observed a weak association between HL proficiency and emotional well-being after hospital discharge. This is a somewhat intuitive finding; one might expect the HL-deficient patient to suffer some level of frustration after a healthcare-related emergency, be it an injury or an acute surgical disease. Nonetheless, there are obviously multiple contributors to emotional well-being beyond literacy that are beyond the scope of this study but are worthy of investigation.
In prior work, we identified that HL-deficient patients may perceive physician–patient communication during hospitalization less satisfactory than HL-proficient patients.6 In the current study, we did not replicate those findings. This may be attributable to the smaller sample size of the current study and the use of a different instrument to assess HL. We did, however, observe that a positive perception of physician compassion among patients with deficient HL contributed positively to postdischarge emotional well-being. Although the correlation between perception of physician compassion and emotional well-being is relatively weak, it nonetheless presents a target of opportunity to improve the postdischarge outcomes of our HL-deficient patients.
It is important to emphasize that what was evaluated was the perception of physician compassion rather than whether a physician was, in fact, compassionate. We think it is a reasonable assumption that most if not all our physicians provide compassionate care. However, it is prudent for those of us who provide patient care to reflect on whether our patients perceive our care as compassionate and identify personal areas for improvement, such as taking the time to sit, rather than stand at the bedside, which is a simple maneuver that is associated with improved patient perception of physician communication.18
There are a number of limitations of this study that are worth of highlighting. For one, we applied a trauma-specific QOL instrument to a mixed cohort of trauma and emergency surgery patients. Although the RT-QOL was not validated in an emergency general surgery patient population, these patients share certain attributes with injured patients and it is presumable that the RT-QOL would be applicable to this group. Specifically, these patients are similar to injured patients in that their illness is acute and unexpected and they undergo procedures that are urgent and usually without opportunity for deliberation. Second, it is impossible to determine which physicians were considered in a patient’s decision to score their perception of physician–patient communication given that they interact with both residents and attendings, and multiple specialties may be involved in the patient’s care. It is quite possible that a particularly negative interaction with one particular physician may have had an outsized influence on the patient’s perception of their experience. Third, the results of this study may not be generalizable. This study was performed in a single institution in the Southwestern United States, and it remains unclear if similar patient cohorts in other areas of the country would have similar outcomes, particularly with respect to RT-QOL, which was validated in a Northeastern patient population.8 Lastly, this study suffered a considerable loss of follow-up leaving open the possibility that the results may have differed significantly with a higher capture rate of those who initially agreed to participate but then did not respond when called to complete the RT-QOL.
In conclusion, we observed a weak correlation between HL proficiency and emotional well-being as measured by the RT-QOL instrument. In addition, we observed that a positive perception of physician compassion may contribute to emotional well-being soon after hospital discharge among HL-deficient patients. Improving patient perception of caregiver compassion during hospitalization may be a target of opportunity with respect to improving QOL after hospital discharge.
Data availability statement
Data are available upon reasonable request. Data will be made available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study obtained approval from St Joseph’s Hospital and Medical Center’s Institutional Review Board (approval number: PHX-19-500-156-50-35).
References
Footnotes
Contributors MJH participated in data collection, writing, and critical revision. HS-L participated in study design, data collection, and critical revision. TML participated in data collection and critical revision. KMC participated in data collection, data analysis, interpretation and writing. JNB and JAW participated in study design, interpretation, writing and critical revision. JAW is the study guarantor.
Funding This research was supported by a grant from our hospital foundation.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.