Article Text

Abstract
Background Patient selection for resuscitative endovascular balloon occlusion of the aorta (REBOA) has evolved during the last decade. A recent multicenter collaboration to implement the newest generation REBOA balloon catheter identified variability in patient selection criteria. The aims of this systematic review were to compare recent REBOA patient selection guidelines and to identify current areas of consensus and variability.
Methods In accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, we conducted a systematic review of clinical practice guidelines for REBOA patient selection in trauma. Published algorithms from 2015 to 2022 and institutional guidelines from a seven-center REBOA collaboration were compiled and synthesized.
Results Ten published algorithms and seven institutional guidelines on REBOA patient selection were included. Broad consensus exists on REBOA deployment for blunt and penetrating trauma patients with non-compressible torso hemorrhage refractory to blood product resuscitation. Algorithms diverge on precise systolic blood pressure triggers for early common femoral artery access and REBOA deployment, as well as the use of REBOA for traumatic arrest and chest or extremity hemorrhage control.
Conclusion Although our convenience sample of institutional guidelines likely underestimates patient selection variability, broad consensus exists in the published literature regarding REBOA deployment for blunt and penetrating trauma patients with hypotension not responsive to resuscitation. Several areas of patient selection variability reflect individual practice environments.
Level of evidence Level 5, systematic review.
- hemorrhage
- resuscitation
- practice guideline
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Resuscitative endovascular balloon occlusion of the aorta (REBOA) practices have evolved during the past decade and patient selection has emerged as a key factor in optimizing REBOA outcomes.
Although several groups have published patient selection algorithms, consensus has not been reached.
WHAT THIS STUDY ADDS
By evaluating REBOA patient selection criteria guidelines from the published literature and multiple trauma hospitals, we identified several elements of broad consensus and ongoing areas of patient selection variability that merit further study.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Articulating consensus around REBOA patient selection provides the trauma community with physiological triggers to optimize clinical outcomes and better care for patients in hemorrhagic shock.
Ongoing areas of patient selection variability and controversy merit further research.
Introduction
In response to the persistent challenge of non-compressible torso hemorrhage, resuscitative endovascular balloon occlusion of the aorta (REBOA) has undergone a revival as a bridge to definitive hemorrhage control. As this tool began to show promise in high-volume trauma centers, innovators in the field proposed patient selection guidelines focused on hypotensive trauma patients with suspected hemorrhage who were partial or non-responders to initial resuscitation.1–3 Military investment in this technology led to more widespread adoption of both training techniques and devices adopted for use in civilian trauma.4 5 In parallel, the American Association for the Surgery of Trauma initiated a registry on the use of REBOA that has proven immensely valuable in testing and refining initial approaches, innovating, training, and evaluating experience.6
As part of the ongoing refinement of REBOA, a multicenter collaboration comprising seven North American trauma centers was launched in 2020 to implement the newest generation REBOA balloon catheter designed for use in trauma. This new device, the pREBOA-PRO Catheter (Prytime Medical Devices, Boerne, TX), was significantly advanced by the Department of Defense funding to address the major limitations of REBOA: the limited complete occlusion time and the ischemic burden of this procedure. This multicenter collaboration effort included robust training and preparation prior to clinical implementation as well as monthly multicenter process improvement meetings to facilitate rapid dissemination of best practices. As part of this effort, all participating centers shared their patient selection algorithms, inspiring an effort to assess the status of consensus on patient selection.
Although national guidelines exist, including the Joint Trauma System (JTS) Clinical Practice Guideline, it remains unclear to what extent a relative consensus exists regarding patient selection for REBOA deployment, including at the institutional level.7 8 Emerging data suggest that earlier action with REBOA in the correct patient population is associated with better outcomes.9 10 Differences in patient selection algorithms may lead to differences in outcomes with REBOA deployment, and the current literature is heterogenous and difficult to interpret due to protocol differences. Patient selection for common femoral artery (CFA) access, the so-called “step up approach,” is also an area of active interest and discussion.11 To identify both areas of gaps in knowledge as well as to highlight areas of consensus, we conducted a systematic review of modern clinical practice guidelines for REBOA patient selection in trauma.
Methods
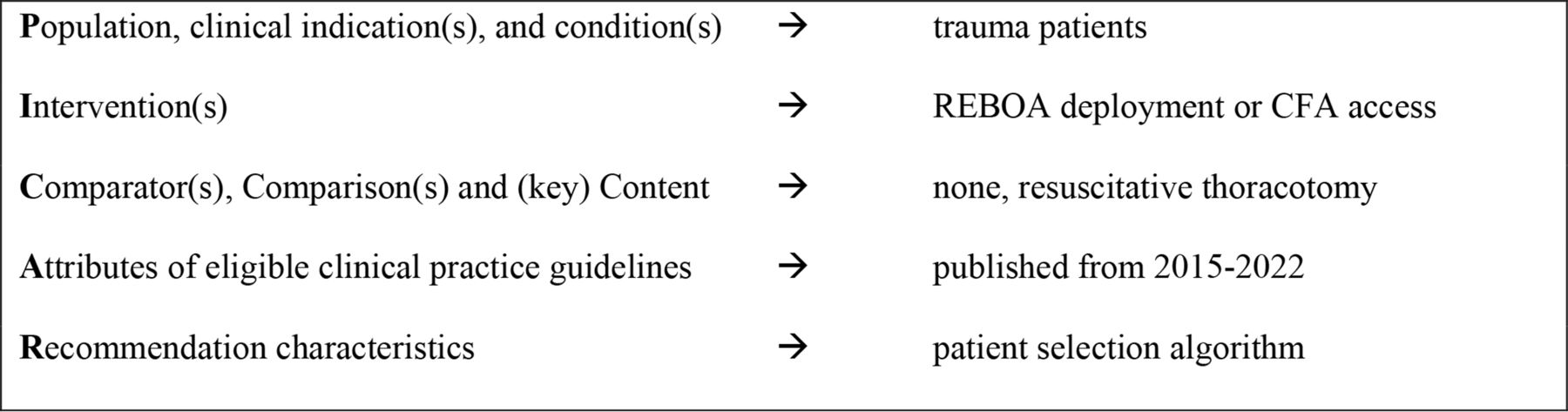
We conducted a systematic review of clinical practice guidelines and algorithms for REBOA patient selection. We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines as well as the PICAR framework (population, intervention, comparison, attributes, and recommendation characteristics) in accordance with best methodological guidance on compiling and synthesizing clinical practice guidelines (figure 1).12 Specifically, we identified all publications describing a patient selection algorithm for REBOA deployment in trauma patients.

PICAR framework for systematic review of REBOA patient selection clinical practice guidelines. CFA, common femoral artery; PICAR, population, intervention, comparison, attributes, and recommendation characteristics; REBOA, resuscitative endovascular balloon occlusion of the aorta.
Identifying eligible guidelines
We used the following PubMed search query in September 2022: ((((resuscitative endovascular balloon) OR (reboa) OR (aortic occlusion)) AND ((trauma) OR (traumatic)) AND ((clinical practice guideline) OR (algorithm) OR (guideline) OR (patient selection))) AND (2015:2022(pdat))). Only English-language publications were included. We chose to limit our inclusion criteria to publications within the last 7 years due to high variability in patient selection in the initial years of REBOA utilization. Articles were reviewed, either the abstracts alone or the full article text as needed, to determine relevance to the PICAR query. We also used an iterative approach to identify any additional publications describing a patient selection algorithm for REBOA deployment in trauma patients. Furthermore, the table of contents of the Journal of Endovascular Resuscitation and Trauma Management (JEVTM) was manually reviewed for any relevant publications.
In addition to the published algorithms identified through the described search, we also included a convenience sample of institutional guidelines for REBOA patient selection from each of the seven level 1 trauma centers in North America involved in the ongoing rollout of the Prytime partial REBOA catheter: Ernest E Moore Shock Trauma Center at Denver Health (Denver, Colorado), Grady Memorial Hospital (Atlanta, Georgia), Grant Medical Center (Columbus, Ohio), Shock Trauma Center (Baltimore, Maryland), St Michael’s Hospital (Toronto, Ontario), University Medical Center New Orleans (New Orleans, Louisiana), and Vanderbilt University Medical Center (Nashville, Tennessee). These algorithms were reviewed and synthesized in a similar fashion.
Quality assessment
Because many of the publications and institutional guidelines were not developed explicitly as evidence-based clinical practice guidelines, we were unable to perform a more structured quality assessment, such as the Appraisal of Guidelines for Research and Evaluation Instrument Version 2.13 Rather, guidelines were broadly characterized as institutional or, where relevant, developed with a more rigorous methodology. We reviewed the guidelines for the presence or absence of cited data sources but did not pursue an indepth analysis of the data sources for each algorithm as that was outside the scope of this review.
Data extraction and analysis
The general characteristics of each guideline were extracted systematically, including publication year, institution, method of development (when stated), scope limitations for intended patient population and intended use environment, inclusion of patient selection criteria for CFA access, contraindications to REBOA use, and criteria used to determine patient selection for REBOA deployment. Finally, we synthesized the patient selection guidelines using a narrative review.
Results
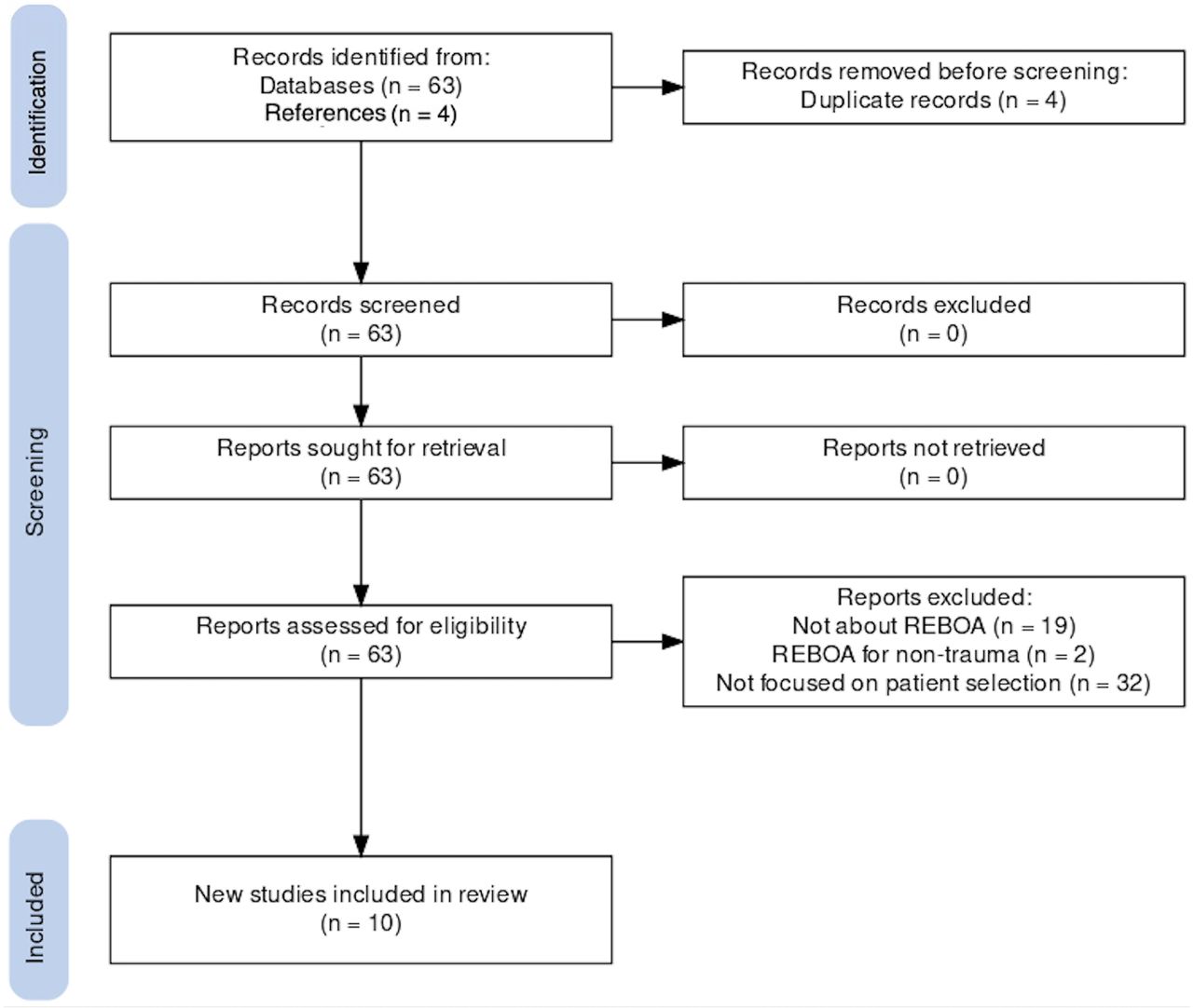
Figure 2 shows the PRISMA flow sheet for the literature review. Sixty-three articles were identified from PubMed query and four additional publications were identified using an iterative approach. One additional publication was identified from the JEVTM website. Four articles presenting duplicate, near-duplicate, or recently updated algorithms were excluded. The 2020 JTS Clinical Practice Guideline on REBOA was a duplicate algorithm of a 2018 article published by Butler et al, and a 2021 Hadley et al article was an updated version of a 2015 Biffl et al14 article presenting the Denver Health algorithm.2 8 15 Two publications from the Cali, Colombia group, both published in 2020, were considered together because they largely presented the same institutional algorithm.16 17 Articles were excluded primarily because they were not relevant to REBOA, did not focus on the trauma population, and/or did not specify an algorithm for patient selection. After assessing for eligibility and removing duplicates, we included a total of 10 articles for synthesis. Some guidelines did not explicitly state the evidence on which they were based.
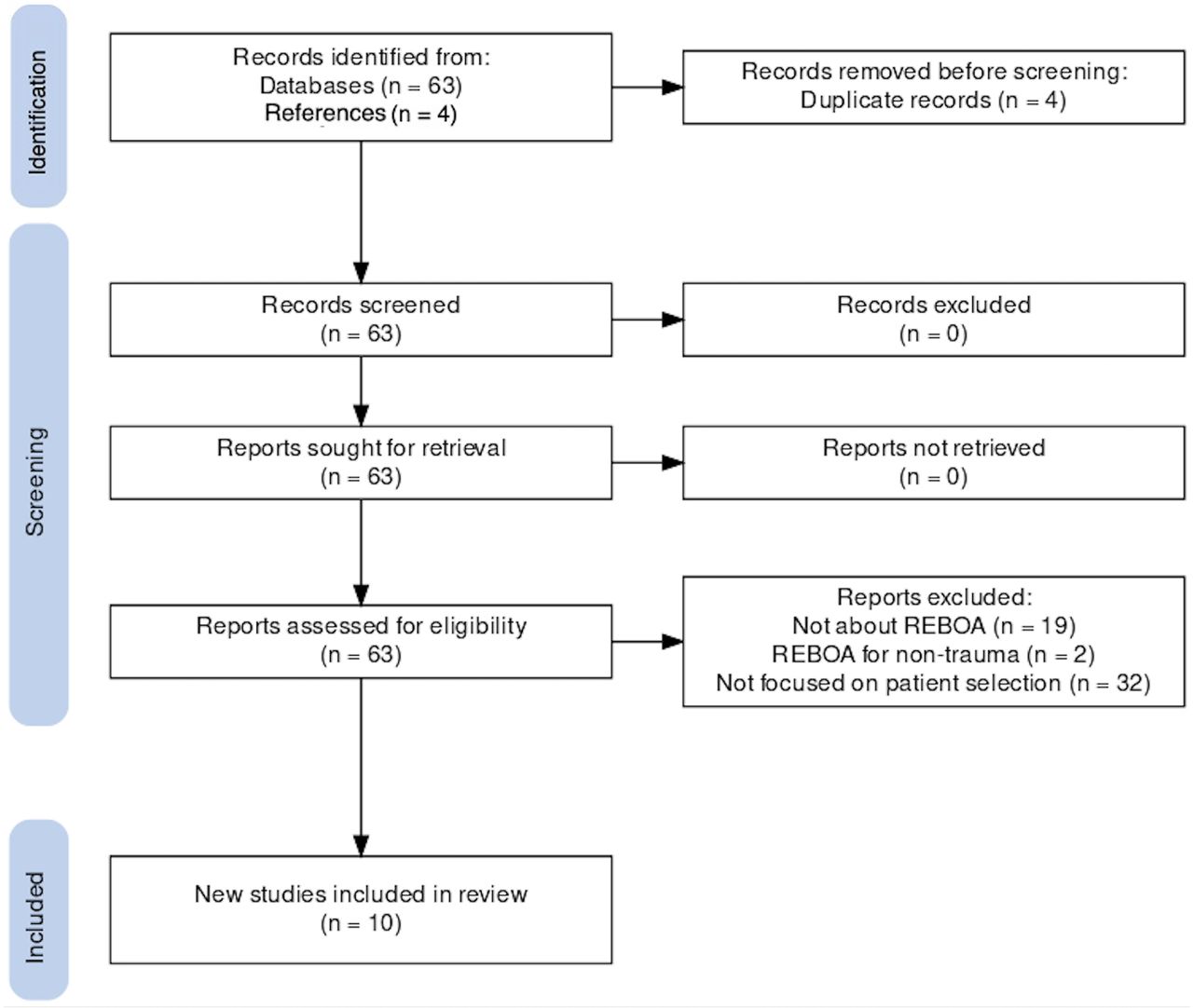
PRISMA flow sheet. REBOA, resuscitative endovascular balloon occlusion of the aorta.
REBOA patient selection
The ten published algorithms are similar in identifying REBOA patient selection criteria as hypotension in both blunt and penetrating trauma with a transient or inadequate response to resuscitation (table 1). Of the 10 algorithms, 4 (40%) cite systolic blood pressure (SBP) <90 mm Hg and 1 uses SBP <80 mm Hg. The remaining algorithms use “hemorrhagic shock”(1), “hypotension” or “hypotensive”(3), and “hemorrhage”(1) as inclusion criteria for REBOA patient selection. Resuscitation is not specifically defined as blood product resuscitation in any of the published algorithms. Similarly, response to resuscitation is not specifically defined in any of the published algorithms but phrased variably as “partial,” “transient,” or “non-response.”
Publications presenting algorithms for REBOA patient selection (2015–2022)
Algorithms differed in defining REBOA patient selection criteria based on hemorrhage location, limiting to “below the diaphragm”(1), “abdominopelvic” (1), “abdominal, pelvic or junctional” (1), “torso” (2), or without anatomic qualifications (3). The Hadley et al15 algorithm (Denver Health) includes a graded approach to REBOA patient selection depending on hemorrhage location.
Partial REBOA patient selection
Table 2 summarizes the seven algorithms used by the level 1 trauma centers involved in the ongoing rollout of the partial REBOA catheter, with the Denver Health algorithm also previously referenced in table 1.15 Patient selection for partial REBOA deployment is similar across institutions, although Denver Health and Vanderbilt University Medical Center use a lower trigger of SBP <80 mm Hg, and St Michael’s Hospital reserves REBOA for patients with a positive abdominal focused assessment with sonography in trauma or pelvic fracture. Resuscitation is not specifically defined as blood product resuscitation, and “non-response” is not specifically defined except in the Grady algorithm. Many institutional guidelines did not explicitly state the evidence on which they were based.
Partial REBOA rollout collaborative institutional algorithms for REBOA patient selection
Contraindications to REBOA and partial REBOA
Contraindications described in the 10 published patient selection algorithms also varied, with 2 out of 10 published algorithms (20%) without any explicit contraindications. The remaining eight algorithms broadly referenced chest trauma as a REBOA contraindication, defined variably as major bleeding “proximal to the left subclavian artery” (1), “severe blunt chest injury”(1), “major thoracic vascular injury” (1), “thoracic hemorrhage” (2), “suspicion of thoracic aortic injury” (2), and limiting to “hemorrhage below the diaphragm” (1), Among the partial REBOA institutional guidelines, four out of seven (57%) listed chest trauma as a contraindication. No algorithm explicitly listed traumatic brain injury (TBI) as a contraindication to REBOA.
REBOA and partial REBOA for traumatic cardiac arrest
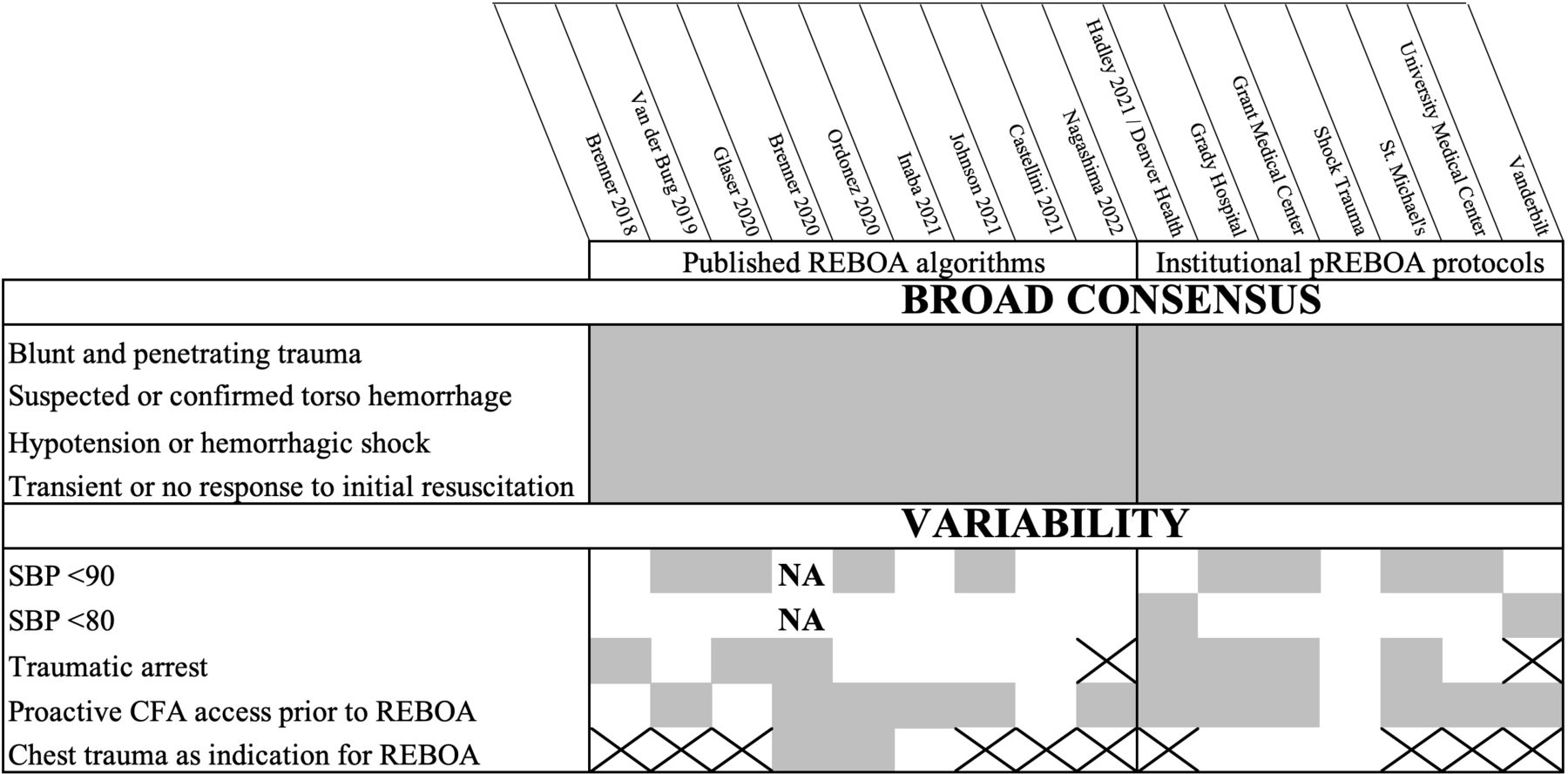
Figure 3 summarizes the specific areas of consensus and variation in practice guidelines for REBOA patient selection as identified from this systematic review. Both published and institutional algorithms differed in the inclusion or exclusion of traumatic arrest patients, with 8 out of 16 (50%) including traumatic arrest as an indication for REBOA. One institutional algorithm (Vanderbilt) used cardiac arrest as an explicit contraindication to partial REBOA.
{kind=link}
{kind=link}
{kind=link}
Consensus and Variability in REBOA Patient Selection Criteria. Gray indicates the inclusion of this detail in the algorithm, white indicates the absence of explicit inclusion, and “X” indicates this detail included as a contraindication. CFA, common femoral artery; NA, not applicable; pREBOA, partial REBOA; REBOA, resuscitative endovascular balloon occlusion of the aorta; SBP, systolic blood pressure.
Criteria for CFA access
Of the 10 published REBOA patient selection algorithms in table 1, 6 (60%) commented on early CFA access. For example, the Borger van der Burg et al7 Delphi method reached consensus on early CFA access being indicated for any trauma victim with advanced trauma life support class III to IV hypovolemic shock and trauma patients with an initial SBP <90 mm Hg and transient or no response to initial fluid or blood products. Among the institutional partial REBOA patient selection algorithms in table 2, triggers for early CFA access vary from essentially identical criteria for CFA access and REBOA deployment at Grady Memorial Hospital, Grant Medical Center, and University Medical Center New Orleans to a stepwise approach at Denver Health depending on the initial SBP and cavitary triage. All but one institution (6 out of 7, 86%) outlined the criteria for CFA access.
Discussion
As evidenced by recent publications linking patient-specific factors to improved survival, REBOA patient selection is crucial.9 10 Despite a decade of controversy and much discussion around optimal patient selection for REBOA deployment in trauma, this systematic review of recent patient selection algorithms in the published literature and in our seven-institution partial REBOA collaborative reveals a relative consensus on which patients are most likely to benefit from REBOA deployment: blunt and penetrating trauma patients with hypotension not responsive to resuscitation. Algorithms diverge on precise SBP triggers for early CFA access and REBOA deployment, as well as the use of REBOA for traumatic arrest and chest or extremity hemorrhage control.
Eight of the 16 published and institutional algorithms summarized in this systematic review stipulate a specific SBP threshold of <90 mm Hg for REBOA use, whereas two algorithms use SBP <80 mm Hg and six algorithms do not specify an SBP threshold. Taken together, these identify a relative consensus with an SBP of less than 80 to 90 mm Hg as a guideline in this patient population. This threshold has remained remarkably constant, as it was first proposed in 2015, prior to the development of trauma-specific REBOA devices and when REBOA for trauma was largely practiced at only a handful of institutions.3 As devices have evolved and the use of REBOA has become more widespread, this threshold has stood the test of time and experience. The clinical significance of SBP <90 mm Hg has been repeatedly confirmed as blood pressures below this threshold are associated with nearly 50% mortality in trauma patients who undergo laparotomy and 32% mortality in patients with pelvic fractures.18 19 There is also broad consensus across the algorithms that patients without an appropriate hemodynamic response to initial resuscitation should be considered for REBOA. Although not explicitly spelled out in the included algorithms, this authorship group thinks that persistent or recurrent hypotension after 1 to 2 units of blood product resuscitation is an appropriate patient selection metric to trigger REBOA deployment in many practice settings.
The algorithms identified in this analysis are remarkably consistent despite divergent situations with variation in available resources. Some differences were noted, which is to be expected when comparing guidelines intended for use in military and civilian settings and across multiple institutions. Among the guidelines we examined, we found those developed for broader use were less specific in their selection criteria. For example, the recently published Western Trauma Association (WTA) guidelines lack a recommendation regarding SBP thresholds for patient selection.20 As the authors note, this more general guideline should be tailored to the specific capabilities and needs of each trauma program.
The algorithms diverge in the exact phrasing regarding chest trauma as a contraindication to REBOA, but 10 (63%) cited major chest trauma as a contraindication, whereas 2 (13%) cited chest trauma as a criterion for REBOA patient selection. Many algorithms do not specifically comment on the specific method of identifying major chest trauma, thoracic vascular trauma, or major bleeding proximal to the left subclavian artery prior to a patient selection for REBOA, but presumably a combination of physical examination, extended Focused Assessment with Sonography for Trauma (eFAST), and portable chest radiograph is the most common and expedient diagnostic approach. The risk of REBOA deployment in the context of major chest trauma is not well quantified due to a paucity of high-quality data, a common theme and challenge in developing criteria for REBOA patient selection.17 Broad-based guidelines such as those developed by the US military and WTA appear to be customizable for individual facilities to enable early CFA access and proactive, successful REBOA deployment in each unique practice setting, balancing the need for emergency hemorrhage control and resuscitation with definitive surgical care. Further research may identify how best to customize patient selection for each practice setting, including those in a variety of military and civilian settings.
Optimizing patient selection for initial CFA access is also critical. The rate-limiting step to REBOA deployment has been shown to be initial CFA access rather than upsizing to the REBOA sheath or deploying the REBOA itself.21 In unpublished data collected by the seven-center pREBOA-PRO collaborative, a minority (20%) of patients who undergo early CFA access progress to REBOA. Further identifying which patients benefit most from early CFA access is ripe for future study, as are safety outcomes for the larger pool of patients undergoing CFA access without REBOA placement.
The use of REBOA and/or resuscitative thoracotomy after traumatic cardiac arrest as a means to achieve aortic occlusion is an area of active debate.22 Half of the algorithms reviewed specifically cited traumatic arrest as a possible criterion for REBOA patient selection, whereas one algorithm (Vanderbilt) mandates a pulse to proceed down the REBOA pathway. Other areas of divergence among REBOA patient selection guidelines may represent knowledge gaps or areas for future study, including how best to rule out major chest trauma, intraoperative REBOA deployment, the possible utility of higher SBP triggers in resource-limited environments, and REBOA patient selection in the context of TBI.
Interestingly, no algorithm specifically listed TBI as a contraindication to REBOA. Future directions may also include investigating the utility of incorporating Glasgow Coma Scale (GCS) score into REBOA patient selection decision-making, as a recent Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) registry study reported that GCS score ≥9 and SBP <90 were useful predictors of success of aortic occlusion.23 Alternatively, in the context of a poor GCS score due to penetrating TBI, REBOA may be used as a less invasive means of aortic occlusion for the purpose of defining survivability for organ donation.
The primary limitation of our study is our use of a convenience sample of the seven level 1 trauma centers in North America involved in partial REBOA rollout rather than a broad survey of all institutions currently using REBOA for traumatic hemorrhage. We recognize that this selection likely led to the exclusion of more varied approaches to patient selection for early CFA access and REBOA deployment and an underestimate of the variability of patient selection algorithms currently in practice, possibly overemphasizing the practice patterns at a select number of high-volume academic North American trauma centers. These patient selection algorithms may not be transferable to prehospital, military, or lower-resourced settings, where different triggers exist for REBOA or CFA access. An additional limitation of our study is our inability to perform a rigorous quality assessment of the included studies. Finally, we included both REBOA and partial REBOA patient selection algorithms for consideration together. As we gather more data on how partial REBOA is best used, these patient selection algorithms may eventually diverge.
Conclusion
In this systematic review of available contemporaneous REBOA patient selection algorithms, we identified broad consensus on REBOA patient selection that includes hypotension with torso hemorrhage unresponsive to initial resuscitation, either caused by blunt or penetrating injury. Variability existed in the specific SBP trigger used, REBOA in traumatic arrest, proactive CFA access, and REBOA in chest trauma.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors All authors participated in study design and critical revision of the article. AWM and BMD drafted the article. AWM performed the literature search and interpretation. AWM is the author acting as guarantor.
Funding Funds for publication costs were provided by Prytime Medical Devices.
Competing interests JJM receives honoraria for lectures from Prytime Medical and is a member of the Prytime Medical Clinical Advisory Board. All authors voluntarily participate in a collaborative group of centers organized by Prytime Medical that share clinical experiences with the pREBOA-PRO device, but none receives compensation for participation.
Provenance and peer review Not commissioned; internally peer reviewed.