Article Text

Abstract
Objective Severe acute kidney injury (sAKI) has been associated with a higher mortality in trauma patients, and severity of trauma often correlates with risk of sAKI. Whether minor to moderate trauma is associated with sAKI is less clear. The purpose of the study was to examine the outcomes of minor to moderate trauma patients who developed sAKI.
Methods The National Trauma Database participant use files of 2017 and 2018 were accessed for the study. All patients aged 18 years old and above who sustained an Injury Severity Score (ISS) of <16 and who were brought to a level I or level II trauma center were included in the study. sAKI was defined as an abrupt decrease in kidney function either three times increase in serum creatinine (SCr) level from the baseline or increase in SCr to ≥4.0 mg/dL (≥353.6 µmol/L), initiation of renal replacement therapy, or anuria for ≥12 hours. Propensity matching analysis was performed between the groups who developed sAKI and without sAKI. Outcome of interest was in-hospital mortality.
Results A total of 655 872 patients fulfilled the inclusion criteria with complete information, of which 1896 patients were found to have sAKI. There were significant differences between the two groups on baseline characteristics. The propensity score matching eliminated all the differences and created 1896 pairs of patients. The median hospital length of stay was longer in patients with sAKI when compared with patients who did not develop sAKI (14 (13 to 15) vs. 5 (5 to 5), days p<0.001) . The overall in-hospital mortality was 20.6% in patients with sAKI compared with 2.1% without sAKI (p<0.001).
Conclusion The occurrence of sAKI in minor to moderate trauma patients was less than 0.5%. There was a three times longer hospital stay in patients with sAKI and 10-fold increase in mortality when compared with patients who did not develop sAKI.
Level of evidence IV.
Study type Observational cohort study.
- multiple trauma
- acute kidney injury
- mortality
Data availability statement
Data may be obtained from a third party and are not publicly available. The data are available from the American College of Surgeon committee on Trauma.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Acute kidney injury was associated with higher severity of the injury.
Higher mortality was reported in severe acute kidney injury (sAKI).
WHAT THIS STUDY ADDS
Current study was designed to see the mortality outcome with minor to moderate injury.
Our study showed a significantly higher mortality associated with minor to moderate injury.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Prevention of AKI with aggressive resuscitation and monitoring may reduce the incidence of sAKI and overall mortality in trauma patients.
Introduction
Trauma can be a leading cause of death and disability in patients aged 45 years or less.1 The impact of trauma on society can be substantial.2 Even for minor injury, the disability-adjusted life-year was found to be 5.2 per 1000 inhabitants.2 The causes of immediate and early deaths of trauma have been associated with brain injury and cardiovascular collapse. However, late death (after 24 hours of injury) is often related to organ failure or infection.3 Acute kidney injury (AKI) is one of the in-hospital organ failure complications that can result in higher mortality and morbidity.4 5
The true prevalence of AKI following a trauma is not known due to different definitions of AKI. Using the risk–injury–loss–failure–end stage (RIFLE) criteria, AKI occurrence was found to be approximately 3% to 9% following major injury.6 7 Severe injury, higher Injury Severity Sore (ISS), hemorrhagic shock, and male gender were found to be some of the risk factors of AKI.8–12 The mortality associated with AKI can range from 20% to 70%.4 5 Likewise, the severity of AKI in the context of trauma often correlates with the outcomes, with more severe acute kidney injury (sAKI) (usually higher stages, eg, failure criteria in RIFLE) associated with worse outcomes.
Most prior studies found an association between sAKI and severe injury. Some of those factors that were associated with the complications of sAKI were also associated with mortality. Therefore, excluding severe injury may be a key component of determining the association of sAKI with mortality. There is a paucity of information regarding the incidence of sAKI in minor to moderate injury and associated outcomes. Therefore, we designed the study to include only mild to moderate trauma patients (excluding all major traumas) and used propensity matching methodology to find the association between sAKI and mortality.
Methods
Data source and inclusion and exclusion criteria
The National Trauma Database (NTDB) participant use files of 2017 and 2018 were accessed for the study. NTDB is the largest trauma database for injured patients. Trauma centers across the USA deposit the data of injured patients voluntarily. Currently, more than 800 centers participate in the data sharing program with NTDB. Included in the study are all patients aged 18 years old and above who sustained an ISS of <16 and who were brought to a level I or level II trauma center with signs of life and were admitted to the hospital for more than 1 day. The patients who sustained cardiac arrest at the scene and all emergency room deaths were excluded from the study. All patients with severe head injury including initial Glasgow Coma Scale (GCS) score of ≤8 or midline shift on brain imaging study or abnormal pupillary reactions were excluded. Patients who received intracranial monitoring for head injury were also excluded from the study. Patients who were discharged from the hospital within 24 hours of admission were excluded as well.
sAKI was defined as an abrupt decrease in kidney function, either a three times increase in serum creatinine (SCr) level from the baseline or an increase in SCr to ≥4.0 mg/dL (≥353.6 µmol/L), initiation of renal replacement therapy, or anuria for≥12 hours.13
Outcomes
The primary outcome of the study was overall in-hospital mortality. The secondary outcomes were hospital length of stay (LOS) and discharge disposition.
Statistics
Patient demographic information and outcomes were summarized using summary statistics (median with IQR (first quartile to third quartile) for continuous variables, and frequency and percentage for categorical variables). To compare the two groups, with and without sAKI, the Wilcoxon rank-sum test was used for continuous variables, and the χ2 test was used for categorical variables. Logistic regression analysis was performed to identify risk factors for sAKI among patients with mild to moderate traumatic injury.
Then the propensity score for ‘sAKI’ was calculated for each subject. One-to-one matching was performed using the ‘nearest neighbor’ approach with a caliper of 0.25 SD as the matching method to pair a subject who developed sAKI with a subject who did not develop sAKI. The propensity score matching was performed using the R package ‘MatchIt’.14 The variables used for calculating the propensity score were age, race (white), sex, hypotension at initial presentation, ISS, GCS score, and comorbidities (alcoholism, anticoagulant, bleeding disorder, chemotherapy, cirrhosis, chronic obstructive pulmonary disease, cerebrovascular accidents, dementia, diabetes, disseminated cancer, functional dependency, congestive heart failure, hypertension on medication, myocardial infarction, peripheral arterial disease, smoking, and steroid and substance abuse). All definitions of the comorbidities were strictly followed from the data dictionary. After matching, the numerical and graphical diagnostics were used to evaluate the improvement. The patient demographic information and outcomes from the matched subjects were summarized as mentioned previously. The Wilcoxon signed-rank test was used to compare the continuous variables between matched groups. McNemar’s test was used to compare the categorical variables between matched groups. For the length of total hospital stay, the Kaplan-Meier procedure was used to estimate the median time, and the SE was estimated using Greenwood’s formula. The Kaplan-Meier curves were generated. The log-rank test was used to compare the time (Kaplan-Meier curves) between the two groups. The two-sided p value was reported for each test. A p value of <0.01 was considered an indication of statistical significance. Statistical analysis was performed using the R language.15
Results
Patients’ characteristics and univariate analysis
A total of 655 872 patients fulfilled the inclusion criteria with complete information (figure 1).

Flow diagram of selection of patients in severe acute kidney injury study. ED, emergency department; GCS, Glasgow Coma Scale; ISS, Injury Severity Score; LOS, length of stay; PUF, participant use file; SBP, systolic blood pressure; TBI,traumatic brain injury; ICP, intracranial pressure; NA,not available
Out of the total, 1896 patients were found to have sAKI. There were significant differences found between the groups who developed sAKI versus who did not. Those differences were more pronounced on age, race and certain comorbidities. The median age of the patients in the sAKI group was 71 years versus 57 years and the patients were predominantly Caucasians (77.9% vs. 74.3%) when compared with patients who did not develop sAKI. Patients with sAKI suffered from higher severity of injury (ISS 9 (5 to 10) vs. 8 (4 to 9)), and a higher proportion of patients presented with hypotension (4.3% vs. 1.3%) (table 1).
Comparison of patients with and without AKI before matching
Risk factors for sAKI in this cohort included male gender, older age, and higher severity of injury within the mild to moderate category. Hypotension (systolic blood pressure <90 mm Hg) was the strongest predictor with an estimated OR of 3.35 (95% CI 2.68 to 4.19, p<0.001). White race was associated with an elevated risk of sAKI (OR 1.22, 95% CI 1.09 to 1.36; p<0.001), whereas Asian race was associated with lower risk of sAKI (OR 0.49, 95% CI 0.31 to 0.77; p=0.002).
Propensity matching analysis
The propensity matching created 1896 pairs of patients. There was more than 90% improvement on standardized mean difference of many variables after the matching (figure 2 and table 2).

Histogram showing improvement in variables after propensity matching.
Comparison of patients with and without AKI after matching
Outcomes
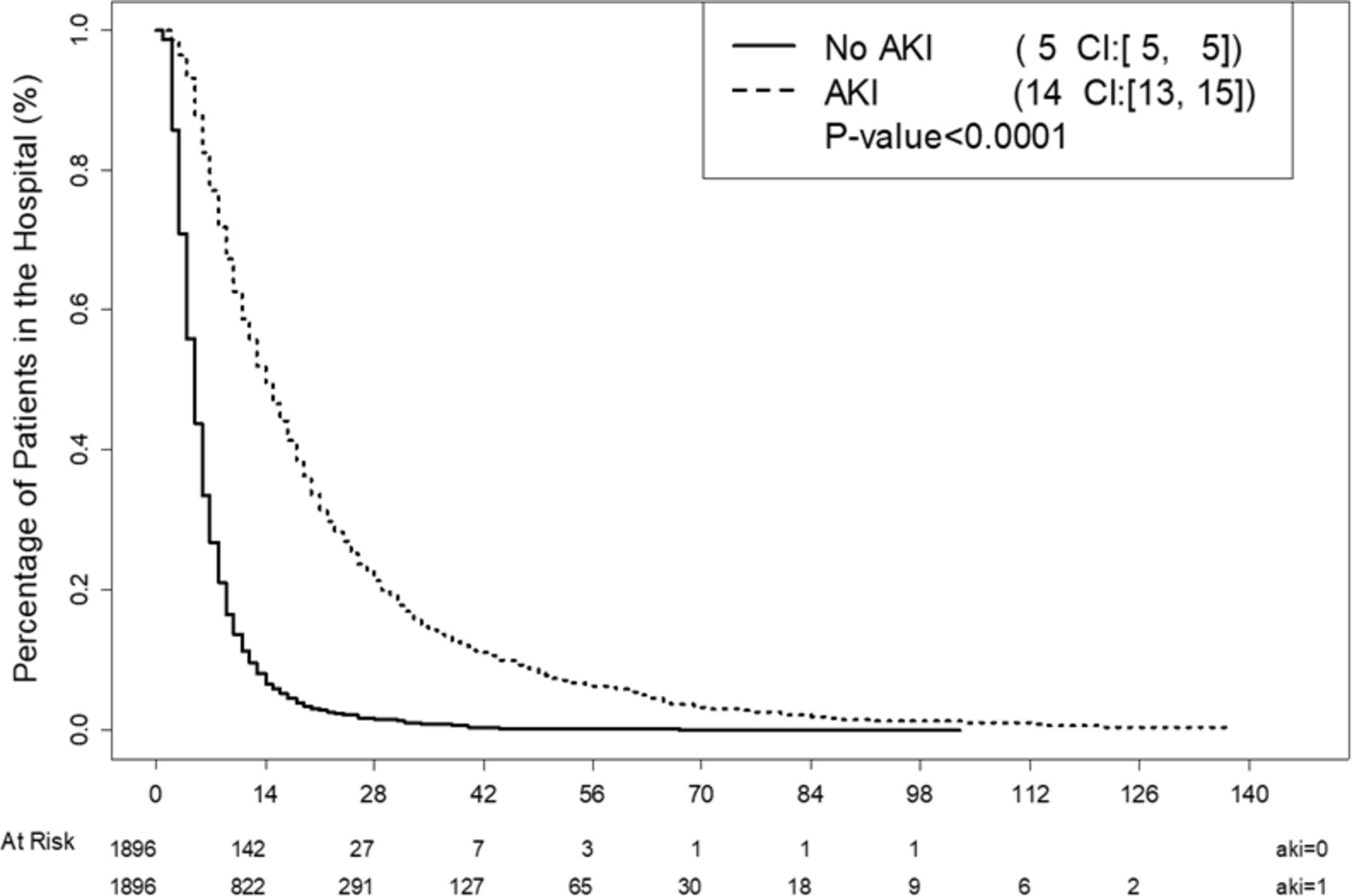
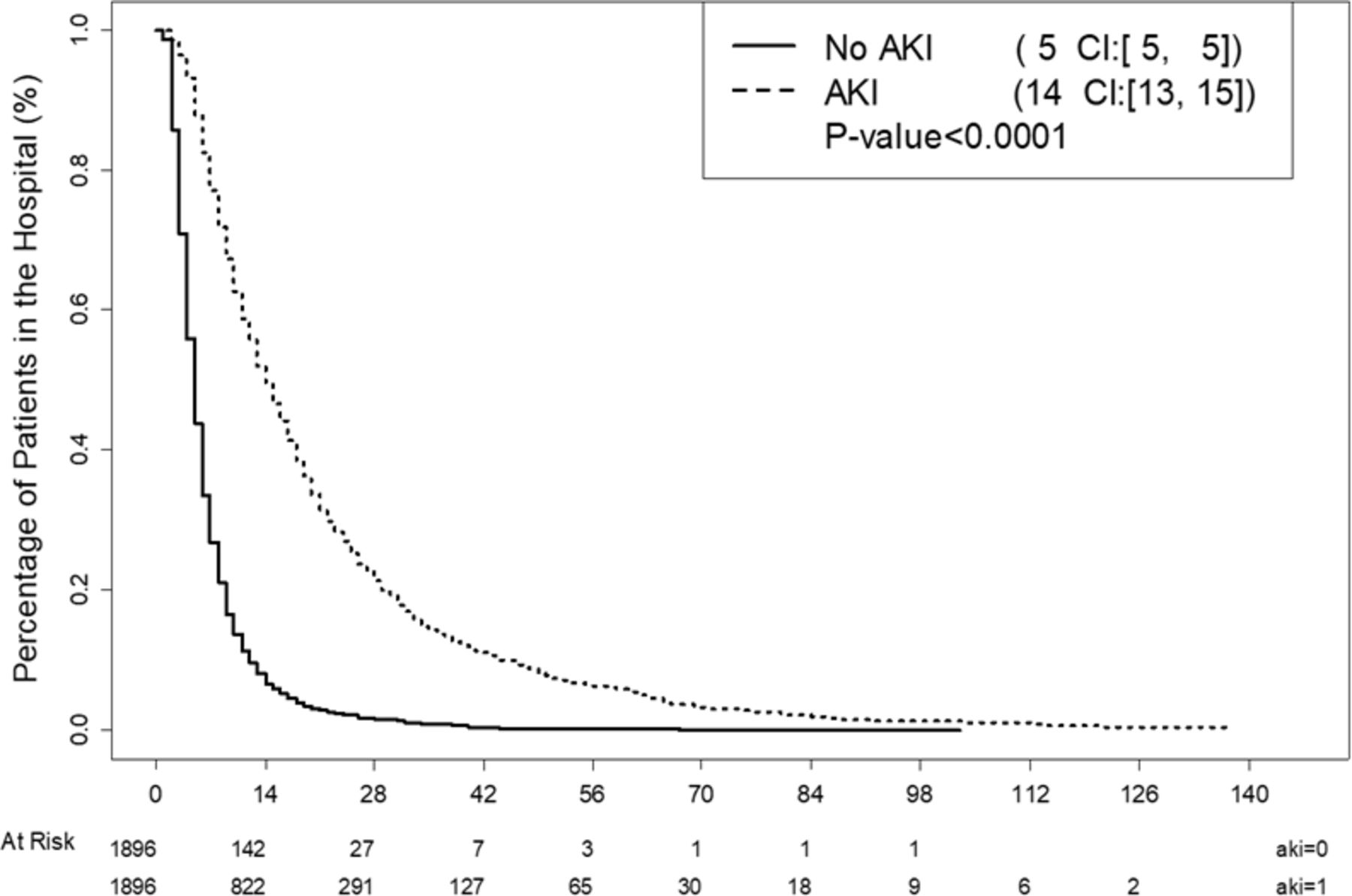
The overall in-hospital mortality was 20.6% in patients with sAKI compared with 2.1% without sAKI. Similarly, the median hospital LOS in patients with sAKI was 14 days (13 to 15) versus 5 days (5 to 5). The median intensive care unit (ICU) stay and ventilator days were prolonged in sAKI when compared with patients who did not develop sAKI (9 days (9 to 10) vs. 3 (3 to 3), p<0.0001, and 14 (12 to 15) vs. 3 (2 to 5), p<0.001) (figure 3 and table 3).
{kind=link}
{kind=link}
{kind=link}
Hospital length of stay between the AKI and no-AKI groups. AKI, acute kidney injury.
Mortality and hospital LOS in matched sample
Higher proportion (34.2% vs. 25.2%) of patients with sAKI was placed in the skilled nursing facility compared with patients without sAKI (table 4).
Discharge disposition of patients who survived hospital admission in matched sample
When the in-hospital complications were compared with the two groups, patients with sAKI had a significantly higher complication rate that included pneumonia, sepsis, DVT, PE, etc (table 5).
In-hospital complications in the matched data
Discussion
Our study showed very high mortality (20.6% vs. 2.1%) in patients with a minor and moderate injury who suffered from sAKI when compared with patients who did not develop sAKI. Patients with sAKI stayed approximately three times longer in the hospital, and a significantly higher number of patients were discharged to a skilled nursing facility.
The mortality associated with minor to moderate injury is lower than severe injury. McHale and colleagues evaluated the Trauma Audit and Research Network dataset for England and found 30 days’ mortality at 4.2% in patients whose ISS was between 9 and 15 and at 3.6% for ISS of <9.16 The mortality was also related to age distribution. The mortality of 85+ years of age was 10.1% versus 1.3% when compared with patients 40 years to 64 years of age with minor to moderate injury. The study did not evaluate patients with in-hospital infection or sAKI. The current analysis suggests that the occurrence of sAKI is associated with a 10-fold increase in mortality in minor to moderate trauma.
Our study also found three times longer hospital LOS and ICU stay and approximately five times longer on ventilator days in patients who developed sAKI versus no sAKI. The patients with sAKI were found to have increased occurrence of in-hospital complication that may have resulted in longer stays in the hospital. As important, we found a 44% of patients in the need for skilled facility placement post hospitalization in those with sAKI. A recent review identified the importance of examining non-mortality outcomes in trauma, given the significant long-term effects on both the individual and society.17 Thus, preventing the long-term consequences of disability remains an important goal of the care of the trauma patient. In this regard, sAKI is an important entity even in minor to moderate trauma, given the effects on mortality and non-mortality outcomes. Identifying means to prevent sAKI or treat to resolve it should be a goal of future studies in this population.
Prior studies evaluated the risk of sAKI in trauma patients found to have a median ISS of >17.5 18 The patients with sAKI who died in these studies had an ISS of >25. Higher ISS is also a known factor for mortality. Therefore, we excluded all patients who had an ISS of ≥16. Despite that, the mortality of the trauma patients with sAKI was approximately 10-fold higher than those who did not develop sAKI. Further analysis of the data showed that advanced age, black race, male gender, higher ISS, and presence of hypotension were associated with sAKI, which is consistent with prior studies.5 18 The majority of risk factors identified in the current analysis are not modifiable (age, gender, and race). However, hypotension conferred a threefold increase in sAKI risk. Thus, despite seeming lower severity of trauma, using all preventive measure that includes aggressive resuscitation remains relevant to preventing sAKI.12 Recently, STOP THE BLEED program, which was started a few years ago, is being implemented across the country by emergency medical service providers, law enforcement agents on the ground and by standard.19 More patients with extremity injury with hemorrhage are being brought to the hospital with tourniquet. Recent whole blood transfusion at the scene and during transportation on hypotensive patients has shown survival benefit.20 Ultimately knowing the cause of AKI is important in providing preventive measures or therapeutics; however, in the current analysis, the exact cause of sAKI is not known. Direct trauma to the kidney is a less frequent event, but indirect impact of immunomodulation after a trauma may be a factor that causes the susceptibility of patients for developing sAKI even in a seemingly minor traumatic injury.21
Limitations
Our study is the first to evaluate the outcomes of sAKI in trauma patients with minor and moderate injury and showed an associated extremely high mortality. However, our study is limited by its retrospective nature. We opted to perform the propensity matching analysis to limit the selection bias. Nevertheless, some potentially important covariates were unavailable for direct evaluation. For instance, due to the unavailability of data relating to the response of resuscitation to the shock state, we could not adjust for the duration of shock and outcomes. Despite the minimization of confounding with propensity score matching, residual confounding cannot be completely eliminated. The NTDB does not provide the exact SCr level or creatinine clearance of the patients. Furthermore, the timing of sAKI is also not available from the database. It is important for all providers to be aware of the consequences of sAKI that minor injuries can turn into devastating events.
Conclusion
The occurrence of sAKI injury in minor to moderate trauma is less than 1%. However, patients with sAKI had an associated three times longer hospital stay and a 10-fold increase in mortality when compared with patients who did not develop sAKI. Future studies should identify means to prevent the development of or progression to sAKI in minor to moderate traumatic injury.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data are available from the American College of Surgeon committee on Trauma.
Ethics statements
Patient consent for publication
Ethics approval
All procedures followed were in accordance with the ethical standards of the institutional review board (IRB) of Meridian Health and with the Helsinki Declaration of 1975, as revised in 2008. Since the data of Trauma Quality Improvement Program (TQIP) are deidentified patient information available to the researchers, the study was exempted from Meridian Health IRB review.
Footnotes
Contributors NA conceived and designed the study and was responsible for retrieving the study data, while YHK performed the data analysis. RM and AA interpreted the data and significantly contributed to the writing of the manuscript. NA accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.