Article Text

Abstract
Background There are a variety of devices capable of performing resuscitative endovascular balloon occlusion of the aorta (REBOA), with most containing compliant balloon material. While compliant material is ideal for balloon inflation due to its “cushioning” effect, it can be problematic to “control” during deflation. The COBRA-OS (Control Of Bleeding, Resuscitation, Arterial Occlusion System) was designed to optimize inflation and deflation of its compliant balloon and was tested in vitro and in vivo with respect to its overinflation and partial REBOA abilities.
Methods For overinflation, the COBRA-OS was inflated in three differently sized inner diameter (ID) vinyl tubes until balloon rupture. It was then overinflated in six harvested swine aortas and in all three REBOA zones of three anesthetized swine. For partial REBOA, the COBRA-OS underwent incremental deflation in a pulsatile benchtop aortic model and in zone 1 of three anesthetized swine.
Results For overinflation, compared with the known aortic rupture threshold of 4 atm, the COBRA-OS exceeded this value in only the smallest of the vinyl tubes: 8 mm ID tube, 6.5 atm; 9.5 mm ID tube, 3.5 atm; 13 mm ID tube, 1.5 atm. It also demonstrated greater than 500% overinflation ability without aortic damage in vitro and caused no aortic damage when inflated to maximum inflation volume in vivo. For partial REBOA, the COBRA-OS was able to provide a titration window of between 3 mL and 4 mL in both the pulsatile vascular model (3.4±0.12 mL) and anesthetized swine (3.8±0.35 mL).
Discussion The COBRA-OS demonstrated the ability to have a cushioning effect during inflation combined with titration control on deflation in vitro and in vivo. This study suggests that despite its balloon compliance, both safe overinflation and partial REBOA can be successfully achieved with the COBRA-OS.
Level of evidence Basic science.
- animal experimentation
- aorta
- hemorrhage
- minimally invasive surgical procedures
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The balloon segments of most resuscitative endovascular balloon occlusion of the aorta (REBOA) devices are made of a compliant material that is meant to help decrease the rare but potentially lethal risk of aortic damage when occluding the aorta compared with semicompliant or non-compliant balloons.
Although compliant material is ideal for balloon inflation due to its “cushioning” effect, it can be problematic to “control” during deflation due to the difficulty of titrating flow past the balloon and therefore limits partial REBOA (p-REBOA) applications.
WHAT THIS STUDY ADDS
The COBRA-OS (Control Of Bleeding, Resuscitation, Arterial Occlusion System) is a novel 4 French REBOA device that has a cushioning effect during inflation combined with titration control on deflation.
This study suggests that despite its balloon compliance, both safe overinflation and p-REBOA can be successfully achieved with the COBRA-OS.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study suggests that the COBRA-OS demonstrates safety if accidentally overinflated during REBOA and can be used for p-REBOA applications.
Background
Endovascular resuscitation and trauma management techniques1 continue to evolve and resuscitative endovascular balloon occlusion of the aorta (REBOA) is one of the tools available. REBOA provides temporary aortic control in non-compressible torso hemorrhage and allows time for definitive surgical hemostasis. There are a variety of REBOA devices capable of achieving aortic occlusion, each with its own advantages and disadvantages.2 The balloon segments of most of these devices are made of a compliant material that is meant to help decrease the rare but potentially lethal risk of aortic damage when occluding the aorta compared with semicompliant or non-compliant balloons.3 While compliant material is ideal for balloon inflation due to its “cushioning” effect, it can be problematic to “control” during deflation due to the difficulty of titrating flow past the balloon. This can lead to significant hypotension on deflation and can limit partial REBOA (p-REBOA) applications. Because of the limitations of traditional compliant balloons, there has been recent emergence of p-REBOA-specific devices incorporating semicompliant balloon materials.4 5
The COBRA-OS (Control Of Bleeding, Resuscitation, Arterial Occlusion System) (Front Line Medical Technologies, London, Ontario, Canada) is a REBOA device that currently has Food and Drug Administration clearance and Health Canada approval. Apart from having the lowest profile of any commercially available REBOA device at 4 French (Fr), the compliant balloon segment of the device was specifically designed to have even safer overinflation ability than traditional compliant balloons and enable more control on deflation for p-REBOA applications. This descriptive study had the dual purpose of investigating how well the COBRA-OS provides a “cushion” during inflation and conversely “control” on deflation. The aim for the “cushion” portion of the study was to determine device balloon characteristics (internal pressure, footprint lengthening, circumferential stretch ratio) and the propensity to cause aortic tissue damage during varying degrees of severe overinflation. For the “control” portion of the study, the aim was to determine how controlled the COBRA-OS was with incremental deflation from full occlusion to determine the applicability to partial aortic occlusion techniques.
Methods
This study conforms with the ARRIVE (Animal Research: Reporting of In Vivo Experiments) guidelines and a complete checklist has been uploaded as online supplemental digital content 1. In vitro experimentation was performed prior to animal study initiation to ensure that there was adequate rationale to proceed with in vivo experiments. A swine model was chosen for the in vivo portion of the study because the model has been used extensively for aortic occlusion studies, resulting in a large volume of data on the vascular response and its correlation to human vascular response. The minimum number of animals possible was used in this study and did not duplicate any previous work. Due to this being a feasibility and mainly descriptive study, no power calculations were performed to determine the sample size and no randomization or blinding occurred. Numerical data are presented as mean with SD. The protocol (study no: 3101-554N) was reviewed and approved by the testing facility’s Institutional Animal Care and Use Committee. The review ensured compliance with the Canadian Council on Animal Care regulations. The testing facility is accredited by the AAALAC (Association for Assessment and Accreditation of Laboratory Animal Care) International and the Canadian Council on Animal Care.
Supplemental material
The in vivo experiments were performed on three female domestic farm pigs Sus scrofa (Landrace-Yorkshire), with weights ranging from 78.4 kg to 93.0 kg. The animals were anesthetized with ketamine, azaperone, and atropine administered intramuscularly. An intravenous catheter was placed in an appropriate vein and anesthesia induction for tracheal intubation was achieved with propofol intravenously. On induction of anesthesia, the animals were intubated and supported with passive ventilation. Isoflurane in oxygen was administered to maintain a surgical plane of anesthesia and intravenous fluid therapy was initiated and maintained throughout the procedure. Once anesthetized, the following intra-arterial access sites were gained on each of the animals: 7 Fr sheath in the left carotid artery for proximal arterial pressure monitoring, 7 Fr sheath in the left femoral artery for distal arterial pressure monitoring and angiography, and a 4 Fr sheath in the right femoral artery for aortic occlusion with the COBRA-OS. Fluoroscopic guidance and angiography were used to assess anatomy and identify the proper location for device positioning and aortic diameters. Proximal and distal mean arterial pressures (MAPs) were recorded every 5 seconds using an Emka data acquisition unit throughout the duration of the study. p-REBOA experiments were performed first, followed by overinflation experiments, and once complete the animals were killed and sent for necropsy.
Cushioning: overinflation ability
In vitro
The pressure that can be generated within a balloon segment during inflation is directly proportional to blood vessel rupture risk, and therefore the COBRA-OS was inflated until failure in stiff vinyl tubes to investigate the maximum pressure that could be produced inside the balloons. The COBRA-OS was inflated until the balloon segment made circumferential wall contact and then was serially inflated by 1 mL increments in three differently sized inner diameter (ID) vinyl tubes (7.94 mm, 9.53 mm, 12.7 mm) until balloon rupture occurred. A digital inflation device (Blue Diamond Digital Inflation Device, Merit Medical, UT) was used to inflate the balloons and record the inflation pressure at each inflation step as well as the maximum pressure just prior to rupture. Balloon footprint length was also measured at each step.
To further investigate the overinflation ability of the COBRA-OS, fresh thoracic aortic tissue from six female domestic farm pigs (Landrace-Yorkshire) weighing approximately 70 kg were obtained from a local commercial pig farm immediately after killing the animal. Institutional approval was not required as this was a postmortem study. The COBRA-OS devices were inflated initially to 13 mL (maximum as per Instructions For Use [IFU], 25 mm diameter) and then serially inflated by 10 mL increments until the balloon or aorta ruptured. At baseline and each inflation step, the measured aortic diameter and the length of the balloon were recorded using a Vernier caliper. The measured aortic diameters were compared with baseline aortic diameters to calculate a circumferential stretch ratio.
In vivo
To investigate the safety of inflation to maximum IFU volume in vivo and to further the idea of “fixed-volume aortic occlusion (FVAO)”,6 swine with aortas intentionally undersized compared with humans were used. The COBRA-OS was inflated until aortic occlusion was confirmed and then intentionally overinflated to 13 mL (maximum as per IFU, 25 mm diameter) in zone 1 (mid-descending thoracic aorta), zone 2 (renal arteries), and zone 3 (aortic bifurcation) in all three animals. Angiograms were performed at each of these zones to measure aortic diameters. Animals were killed and a limited necropsy was performed for gross examination of the treatment sites for evidence of damage. Anatomic markers, treatment angiographic images, and procedural notes were used to help identify the treated vessel sites as accurately as possible.
Control: p-REBOA ability
In vitro
The COBRA-OS was tested on a closed-loop, three dimensional-printed vascular model with a pulsatile pump. Pressures above and below the balloon were measured using a digital pressure monitor (Compass device, Centurion Medical Products, Memphis, TN). The device was inflated until occlusion of the aorta (21 mm diameter) and then serially deflated by 0.2 mL increments every 30 seconds until pressures above and below the balloon equalized. This was repeated two further times to confirm the results.
In vivo
The COBRA-OS was placed in zone 1 (mid-descending thoracic aorta) and inflated until aortic occlusion was confirmed in all three animals. The device was then serially deflated by 0.2 mL increments every 30 seconds until pressures above and below the balloon equalized. Fluoroscopy was used to visualize the balloon on deflation to monitor its shape.
Results
Cushioning: overinflation ability
In vitro
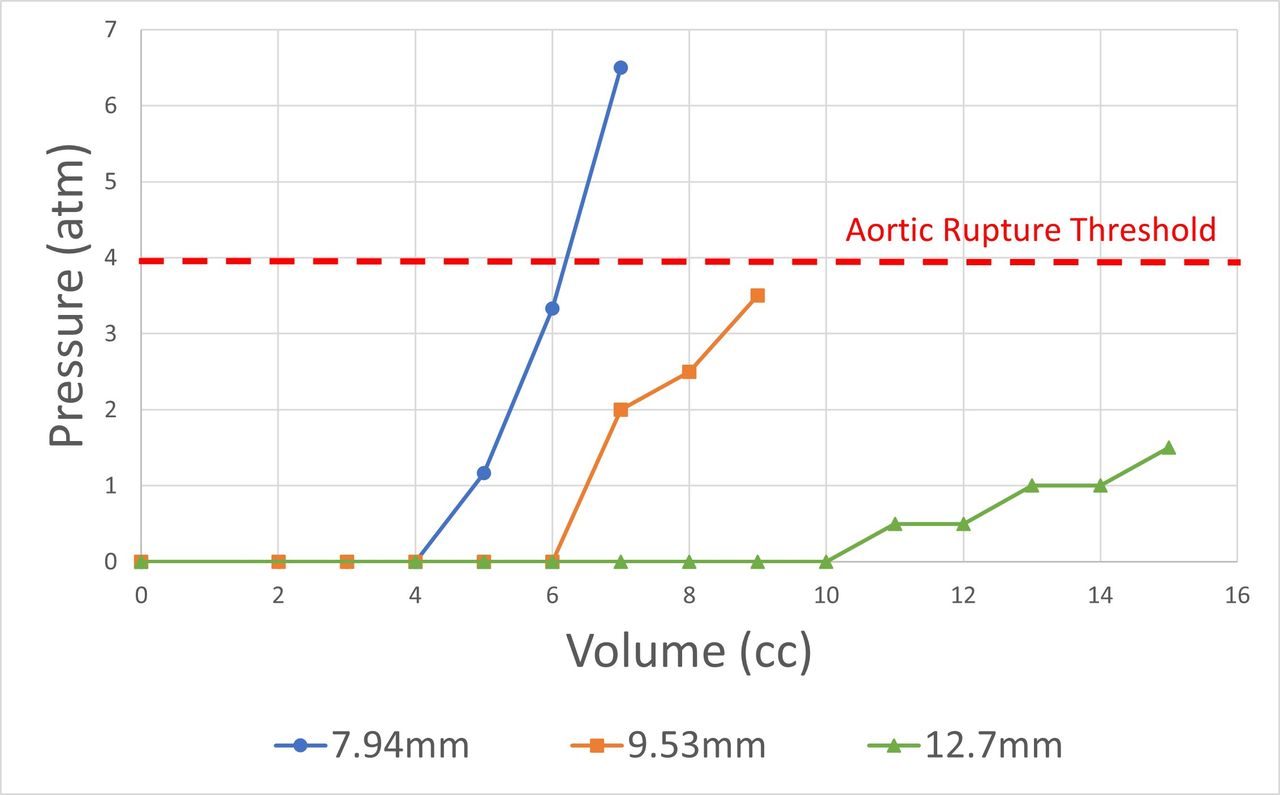
In the 7.94 mm ID tube, the COBRA-OS generated a maximal internal pressure of 6.5 atm, while in the 9.53 mm and 12.7 mm ID tubes the devices generated maximal internal pressures of 3.5 atm and 1.5 atm, respectively (table 1, figure 1). The footprint lengths at rupture ranged from 90 mm to 110 mm.
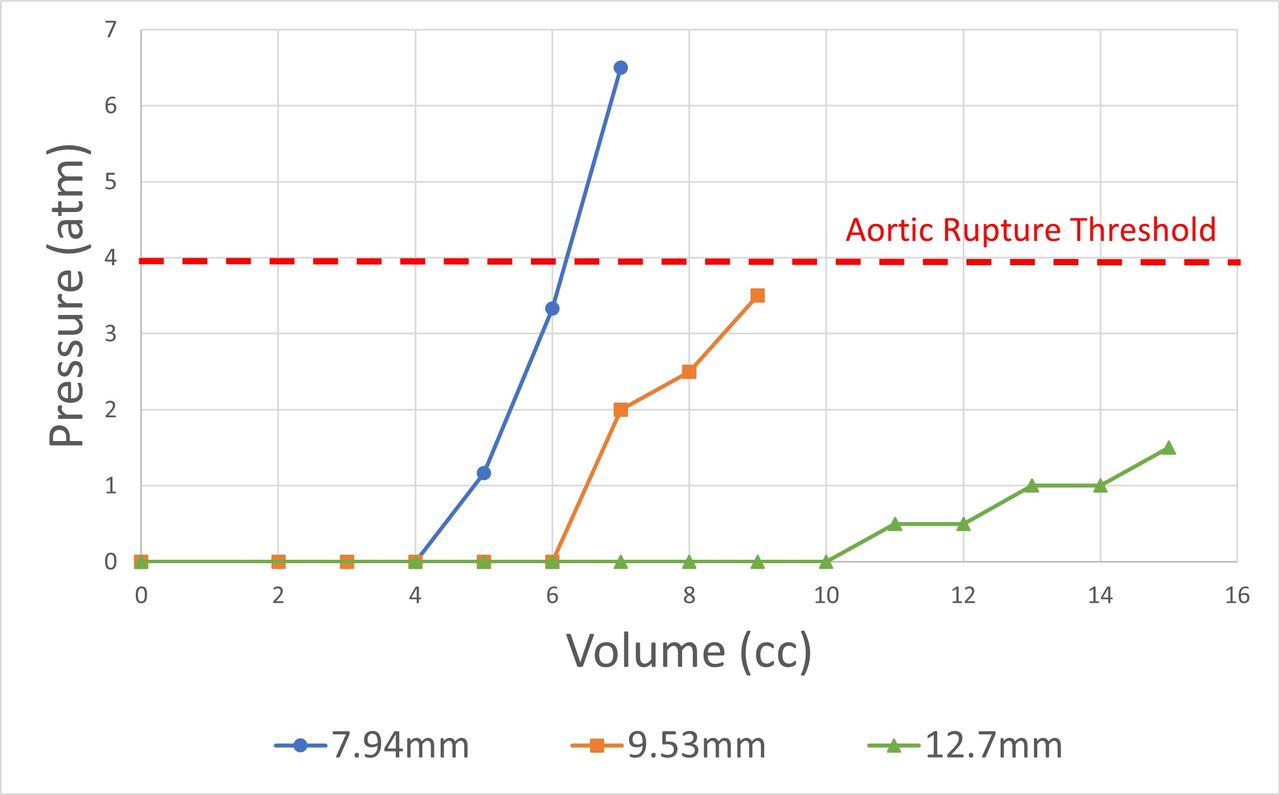
Graph of internal pressures generated by the COBRA-OS inflated to balloon rupture in three differently sized inner diameter vinyl tubes. COBRA-OS, Control Of Bleeding, Resuscitation, Arterial Occlusion System.
COBRA-OS devices inflated to balloon rupture in three differently sized inner diameter vinyl tubes
The mean diameter of the harvested thoracic aortas was 21±0.10 mm and all balloons ruptured before causing gross intimal damage. The mean balloon overinflation volume at rupture for the COBRA-OS was 86±6.2 mL, which represents a 562% increase over the IFU volume (13 mL), and the mean footprint length at rupture was 130±14 mm (figure 2). The mean circumferential stretch ratio at balloon rupture was 1.53±0.04.

Image of the COBRA-OS inflated to 80 mL in a swine thoracic aorta just prior to rupture of the balloon. COBRA-OS, Control Of Bleeding, Resuscitation, Arterial Occlusion System.
In vivo
The mean weight of the animals used in the study was 84±6.6 kg. In zone 1, the mean aortic diameter was 15.0±0.4 mm, the mean occlusion volume was 6.0±1.0 mL, and the mean overinflation percentage above maximum IFU (13 mL, 25 mm diameter) was 117±37%. In zone 2, the mean aortic diameter was 14.4±0.4 mm, the mean occlusion volume was 5.4±0.6 mL, and the mean overinflation percentage was 141±24%. In zone 3, the mean aortic diameter was 12.0±1.1 mm, the mean occlusion volume was 5.0±0 mL, and the mean overinflation percentage was 160±0%. On necropsy, there was no evidence of intimal damage or thrombus in any treatment zone.
Control: p-REBOA ability
In vitro using the closed-loop pulsatile model, proximal and distal pressures returned to baseline over a mean deflation volume of 3.4±0.12 mL for the COBRA-OS. Subsequently, in vivo, proximal and distal pressures equalized in a linear fashion over a mean deflation volume of 3.8±0.35 mL (figure 3). The COBRA-OS device maintained its overall shape throughout deflation (figure 4).
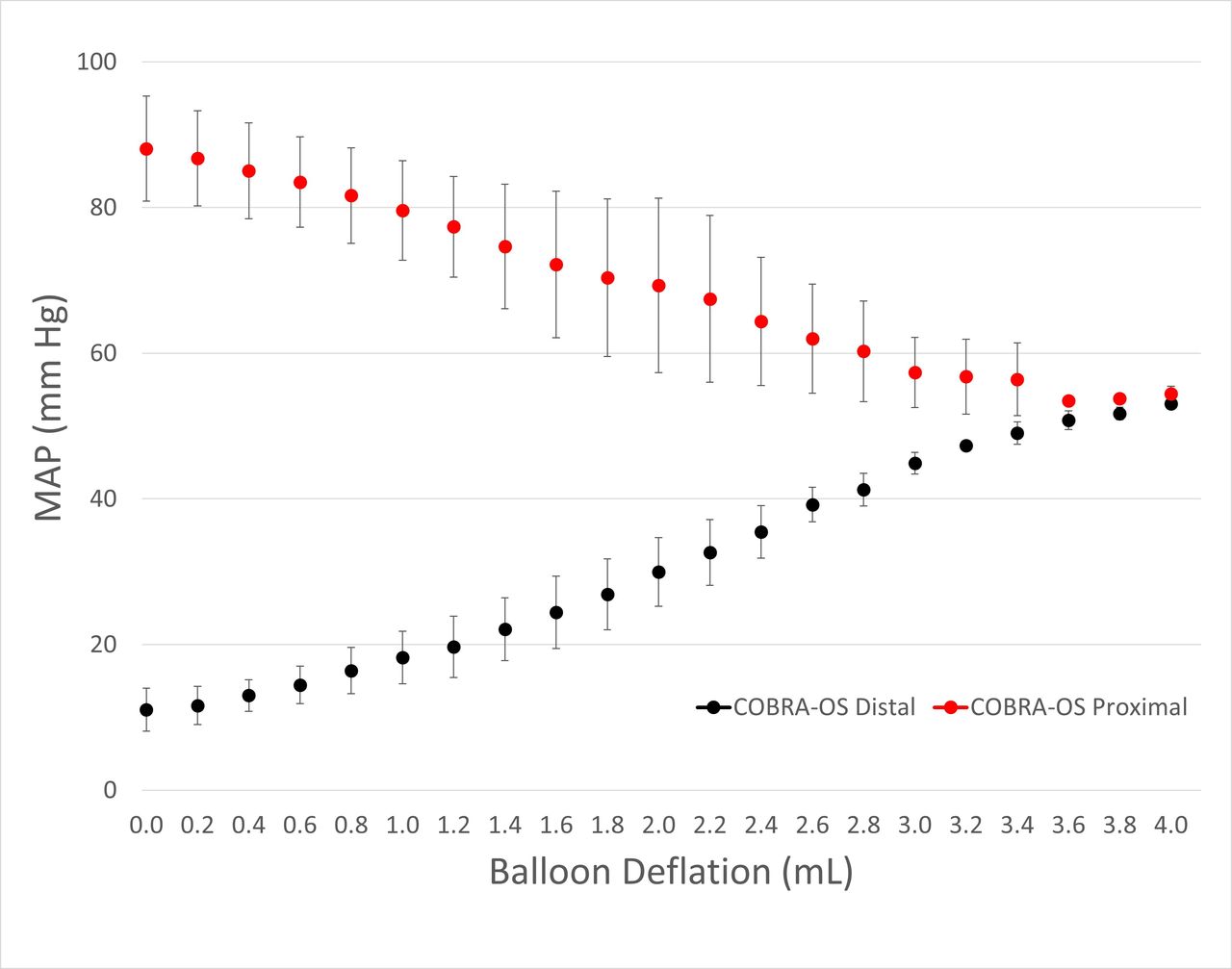
Graph of the mean proximal and distal mean arterial pressures (MAPs) produced by incremental balloon deflation of the COBRA-OS in vivo. COBRA-OS, Control Of Bleeding, Resuscitation, Arterial Occlusion System.

Fluoroscopic image of the COBRA-OS maintaining its shape through deflation. COBRA-OS, Control Of Bleeding, Resuscitation, Arterial Occlusion System.
Discussion
The COBRA-OS is a 4 Fr REBOA device that was designed to optimize inflation and deflation of its compliant balloon. These in vitro and in vivo studies show that the COBRA-OS has safe overinflation ability and a linear, relatively wide window of titration control for p-REBOA applications.
Aortic rupture during REBOA is a rare but potentially lethal complication. Although infrequent with most current generation REBOA devices, there are a variety of circumstances whereby additional overinflation ability might prove useful. REBOA in pediatric trauma is currently being investigated,7 and since pediatric aortic sizes are smaller and more variable depending on age, balloon overinflation may occur, predisposing patients to aortic injury. The issue of variable blood vessel sizes also occurs when performing balloon occlusion for proximal control in arteries other than the aorta, such as in the axillary/subclavian artery or iliac artery, before vascular repair.8 The iliac artery itself can also be iatrogenically injured during zone 3 REBOA due to migration of the balloon caudally, and the additional overinflation ability of the COBRA-OS has previously been found to help prevent this complication in an animal model.9 Further, safe overinflation may be useful in patients that are severely hypotensive when proximal and distal occlusion confirmation techniques may not be accurate and during REBOA with an overzealous inexperienced user who might inadvertently overinflate.
In our study, inflation of devices in the vinyl tubes showed that as the tube diameter increased, the pressure generated by the devices decreased and the balloons ruptured at lower internal pressures. The quoted rupture pressure of the aortic wall is 4 atm10 and the COBRA-OS went beyond 4 atm only in the smallest diameter tube (7.94 mm ID), which is much smaller than typical adult human aortic diameters. Circumferential stretch ratio has been used to determine aortic failure in multiple previous studies.11–14 The ER-REBOA (Prytime Medical, TX) was previously investigated for rupture risk and the authors found the circumferential stretch ratio at aortic failure to be 1.8, which aligns with other studies that report 1.7.11 The ER-REBOA was only inflated to 24 mL (maximum as per the manufacturer’s IFU) and three ruptures occurred in 14 specimens. In contrast, the COBRA-OS had no ruptures in harvested aortas and never generated a circumferential stretch ratio greater than 1.6 despite greater than 500% overinflation. This overinflation ability was further confirmed in vivo whereby significant overinflation to maximum IFU inflation volume resulted in no vessel damage or rupture of the balloons. The mean aortic diameter was only 15 mm in zone 1, and even smaller in the other zones, which represented an undersized human aorta (average diameter of 22–23 mm).15 This furthers the possibility of having a “fixed-volume aortic occlusion” device that allows significant overinflation to simplify procedures for providers that may have less experience or skill. Thus, monitoring proximal or distal pressures to confirm occlusion would not be needed and instead providers would inflate to a set single volume (13 mL) in all patients.6
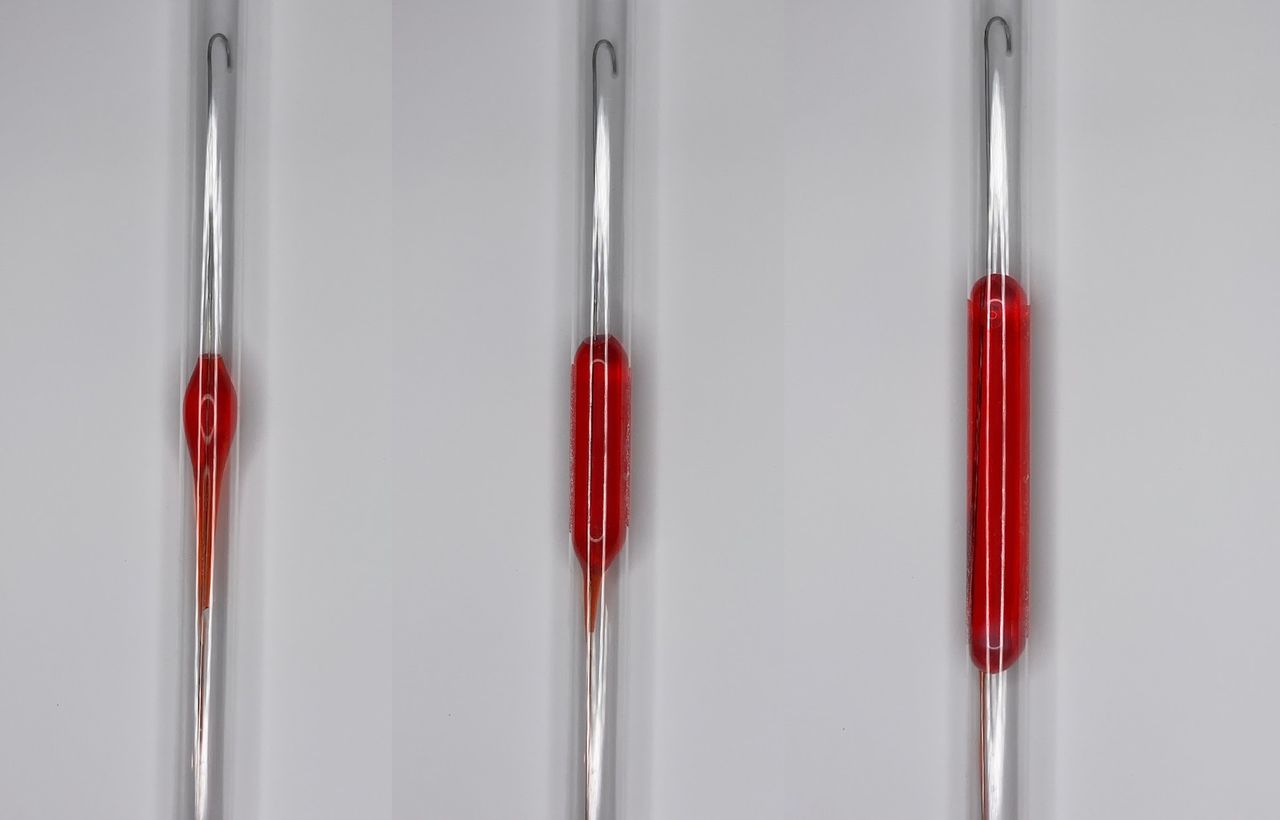
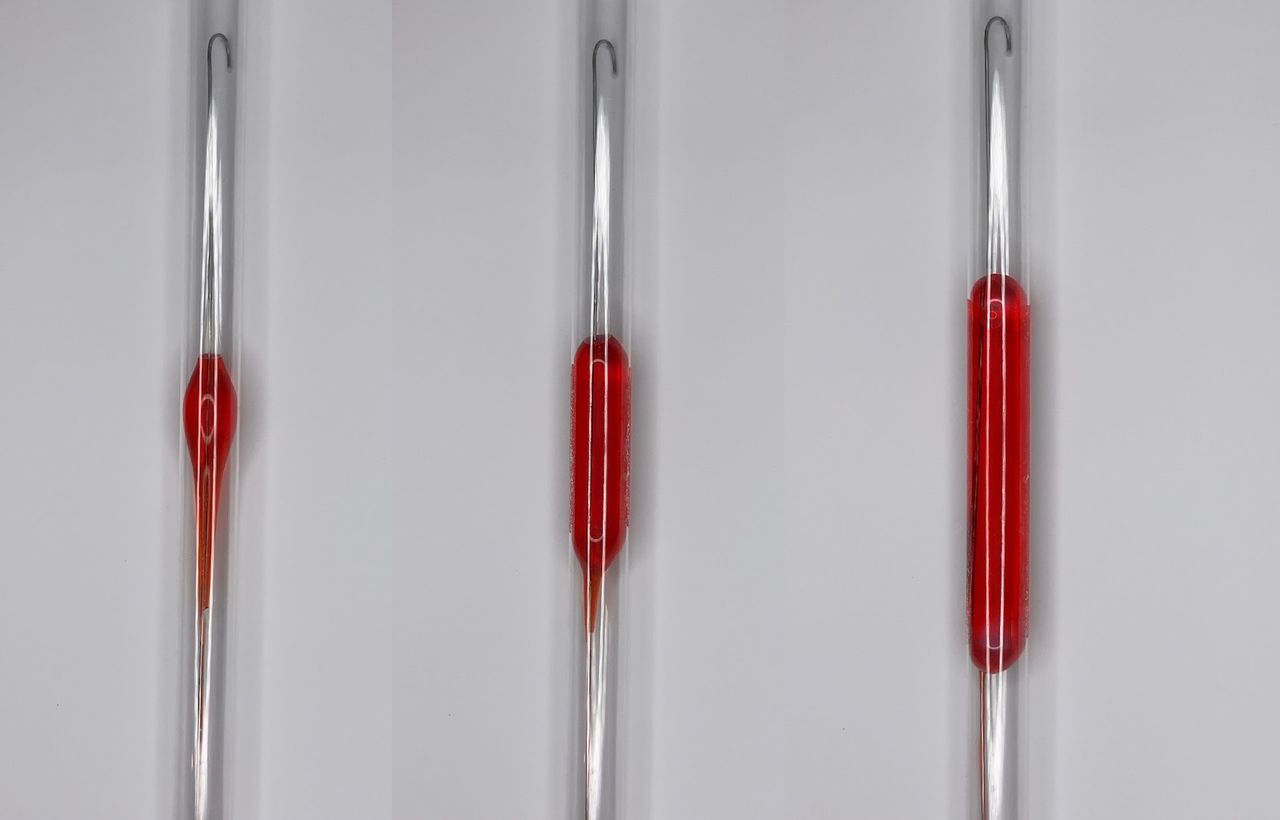
The “cushioning” effect of the COBRA-OS is mainly due to its unique “Safety Shoulder Reservoir.” The compliant balloon material extends beyond the balloon footprint with a proximal tapered segment (shoulder). As the COBRA-OS inflates and meets the wall of the vessel and continues inflating, the additional volume and pressure is offloaded into the reservoir, resulting in lengthening of the balloon caudally as opposed to having the balloon continue to increase in diameter if accidental overinflation occurs (figure 5). It is important to note that when used as per IFU, the footprint of the COBRA-OS remains at 4 cm to 6 cm during full aortic occlusion. The balloon only grows in length if a user does not monitor when cessation of distal flow is achieved and instead inadvertently continues to inflate.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Image showing three serial inflations of the COBRA-OS demonstrating the proximal safety shoulder reservoir. COBRA-OS, Control Of Bleeding, Resuscitation, Arterial Occlusion System.
p-REBOA is a newer technique that is being investigated to potentially mitigate the harmful effects of prolonged aortic occlusion, allowing for hypertension above the balloon, some degree of partial flow past the balloon to perfuse organs, and permissive hypotension below the balloon to help limit hemorrhage.16 As mentioned previously, traditional compliant balloons have difficulty achieving this for a variety of reasons, although many authors have reported on p-REBOA using older generation REBOA devices.17 18 The ideal degree of “fine tuning” is completely unknown and most studies have targeted a single distal MAP (20–40 mm Hg) as opposed to continuously manipulating the amount of partial flow past the balloon according to physiological needs.18 Therefore, a large titration window is likely not required if the p-REBOA device can hit and maintain a set target distal pressure range. Additionally, it is unknown if intermittent REBOA is a useful alternative strategy to p-REBOA, where balloon titration ability would not be needed.19
One of the main concerns with current REBOA techniques is the use of a 7 Fr sheath, which can limit the outflow to a patient’s limb and may be further exacerbated over a planned longer p-REBOA period. Despite the possible benefits of partial occlusion with a 7 Fr sheath, these may have to be balanced with an elevated risk of limb complications due to the outflow obstruction.20 Reported limb complications that happen after complete REBOA using a 7 Fr sheath primarily affect the access site limb, as opposed to both limbs, implying that this is more related to the unilateral sheath combined with aortic occlusion as opposed to the aortic occlusion itself. A recent large retrospective study by Laverty et al20 and the AORTA (Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery) investigators reported 24 of 352 (7%) arterial access-related limb ischemic complications using the 7 Fr ER-REBOA (Prytime Medical). The use of a 4 Fr REBOA device with p-REBOA abilities, such as the COBRA-OS, may help to mitigate these complications in both partial and complete REBOA.
Our in vitro and in vivo studies revealed that the COBRA-OS has a window of p-REBOA titration ability between 3 mL and 4 mL of volume removed from the balloon. Functionally speaking, it was easy to take small 0.2 mL aliquots from the balloon with the supplied 10 mL syringe (0.2 mL gradations) to achieve this. Removing small aliquots has been difficult to achieve in the past with previous devices because all other REBOA devices before the COBRA-OS had large inflation lumens, and when you opened the stopcock to deflate, the inflation fluid quickly drained from the device, even without drawing back on the syringe, making precise deflation unachievable. In response to this, DuBose21 described a technique that used a 3 mL syringe attached to a three-way stopcock to help precisely control deflation over 0.1 mL increments.17 A previous animal study investigated incremental deflation of the ER-REBOA following 60 minutes of full occlusion in a hemorrhagic model and found that rapid return of flow occurred over a single 0.5 mL step.17 The single inflation lumen of the COBRA-OS is much smaller than in other REBOA devices, which allows small aliquots of inflation medium to be removed from the balloon more easily compared with other devices. It is worth noting that the minimum time it takes once you open the stopcock and withdraw on the syringe to go from full occlusion to full equalization of proximal and distal blood pressures is probably a more useful measure of a device’s p-REBOA ability as opposed to titration windows. For an average diameter human aorta, this happens very quickly with other REBOA devices, while this cannot happen any faster than 10 to 15 seconds with the COBRA-OS (see online supplemental digital content 2).
Supplementary video
The balloon material of the COBRA-OS is compliant, and the offset shape is designed to counteract the “tear-drop” shape that normally forms when deflating the balloon of older generation REBOA devices.22 This tear-drop effect makes most spherical balloons act more like an “on/off switch” as opposed to the preferred “dimmer switch.”23 Additionally, the COBRA-OS balloon has mechanical properties that allow it to maintain its overall shape throughout inflation and deflation cycles as seen in vivo from fluoroscopy images and is demonstrated in online supplemental digital content 3. This design feature was implemented so that once a target distal pressure was reached, there would be less balloon volume manipulation required to maintain the desired distal MAP.
Supplementary video
In clinical practice, p-REBOA with the COBRA-OS can be performed by first transducing the sidearm of the supplied 4 Fr sheath for distal MAP measurements. With full aortic occlusion, the MAP is close to 0 and no pulsatile wave form is seen. The stopcock is then opened, and withdrawal of the syringe is performed until a pulsatile wave form first appears. A preferred distal MAP can then be adjusted by removing 0.2 mL to 0.4 mL aliquots until the target MAP is achieved. It is important to note that for efficiency these small incremental inflations or deflations are only done after the wave form first appears and not from full occlusion as was done in this study.
There are several limitations to the current study. The experiments were mainly performed to investigate the function and performance of the COBRA-OS and therefore highly controlled in vitro and in vivo models were used. Future in vivo studies should investigate these properties in a hemorrhagic animal model with prolonged occlusion to better simulate clinical use environments. Also, flow was not measured in vivo as previously done in other studies.24 Proximal and distal pressures alone were used in this study because it is the only clinically available option currently to estimate the degree of p-REBOA. With regard to aortic rupture risk, swine aorta is reasonable for comparison with human aorta but the walls are known to be thicker and therefore direct correlation to humans is cautioned.
Conclusion
The COBRA-OS has demonstrated the ability to have a cushioning effect during inflation combined with titration control on deflation in vitro and in vivo. This study suggests that despite its balloon compliance, both safe overinflation and p-REBOA can be successfully achieved with the COBRA-OS. These features may be useful when performing REBOA clinically.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank Seema Gogna for her assistance in helping with the animal lab research.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at Data from this article were presented at the Trauma Association of Canada Annual Meeting on April 8, 2022.
Contributors APo and APa were involved in study design. APo and APa were involved in data collection. All authors were involved in data analysis, data interpretation and critical revisions. The first draft of the article was written by APo and is the author responsible for the overall content as the guarantor .
Funding This study was funded by Front Line Medical Technologies (paid for the animal study expenses).
Competing interests APo and APa are cofounders and have an equity stake in Front Line Medical Technologies. LJM is Chair of the Scientific Advisory Board, has an equity stake, and receives consulting fees from Front Line Medical Technologies. NP is on the Scientific Advisory Board and owns shares in the company.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.