Article Text

Abstract
Background Despite appropriate care, most patients do not survive traumatic cardiac arrest, and many survivors suffer from permanent neurological disability. The prevalence of non-dismal neurological outcomes remains unclear.
Objectives The aim of the current review is to summarize and assess the quality of reporting of the neurological outcomes in traumatic cardiac arrest survivors.
Data sources A systematic review of Embase, Medline, PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and ProQuest databases was performed from inception of the database to July 2020.
Study eligibility criteria Observational cohort studies that reported neurological outcomes of patients surviving traumatic cardiac arrest were included.
Participants and interventions Patients who were resuscitated following traumatic cardiac arrest.
Study appraisal and synthesis methods The quality of the included studies was assessed using ROBINS-I (Risk of Bias in Non-Randomized Studies - of Interventions) for observational studies.
Results From 4295 retrieved studies, 40 were included (n=23 644 patients). The survival rate was 9.2% (n=2168 patients). Neurological status was primarily assessed at discharge. Overall, 45.8% of the survivors had good or moderate neurological recovery, 29.0% had severe neurological disability or suffered a vegetative state, and 25.2% had missing neurological outcomes. Seventeen studies qualitatively described neurological outcomes based on patient disposition and 23 studies used standardized outcome scales. 28 studies had a serious risk of bias and 12 had moderate risk of bias.
Limitations The existing literature is characterized by inadequate outcome reporting and a high risk of bias, which limit our ability to prognosticate in this patient population.
Conclusions or implications of key findings Good and moderate neurological recoveries are frequently reported in patients who survive traumatic cardiac arrest. Prospective studies focused on quality of survivorship in traumatic arrest are urgently needed.
Level of evidence Systematic review, level IV.
PROSPERO registration number CRD42020198482.
- outcomes
- traumatic
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Traumatic cardiac arrest (TCA) occurs due to severe injury, most commonly from traumatic brain injury and hemorrhage.1 Despite appropriate care, TCA has been associated with extremely low survival rates, with 2% of patients surviving to hospital discharge.2 Some authors have even concluded that resuscitation of patients with TCA is futile and costly.3 However, recent data from prospectively registered trauma systems in England, Spain, and North America have suggested that outcomes from TCA may be better than previously expected, with overall survival rates between 5.7% and 7.5%.4–6 Advances in damage control resuscitation and our understanding of its pathophysiology have led to improvements in the contemporary management of TCA, which is at least partially responsible for the observed increase in overall survival.7
The prognostication of patients with TCA is an important consideration for patients, families, and health providers that initiate resuscitative efforts, as after survival the main treatment goal is a favorable neurological outcome.3 8 Poor outcomes after cardiac arrest of any etiology have been attributed to hypoxic-ischemic brain injury.9 The extent of this brain injury is an important predictor of unfavorable neurological outcomes, which are defined by death from neurological cause, persistent vegetative state, or severe neurological disability.9 Most studies examining cardiac arrest outcomes use the Cerebral Performance Categories (CPCs) or the Glasgow Outcome Scale (GOS) to report neurological status.9 Other scales that have demonstrated value in assessing the neurological outcome of survivors include the modified Rankin Scale (mRS), the Extended Glasgow Coma Scale (GOSE), and the Functional Independence Measure (FIM).10–12 Despite the existence of several validated measures, in many neuroprognostication studies, neurological outcomes are generally dichotomized as “good” or “poor”, with no consensus on how a poor outcome is defined.9 The neurological outcome of these patients remains unclear in the current literature. Among TCA survivors, residual neurological deficits have generally been found to be severe and disabling in small observational studies.13 14 However, a systematic review in 2012 found that more than half of TCA survivors either make a full neurological recovery or have moderate deficits.15
Although previous literature has focused on summarizing the proportion of survivors and identifying resuscitation techniques to reduce mortality in traumatic arrest, minimal evidence exists that assesses the quality of neurological outcome data. Hence, we performed a systematic review to summarize the neurological outcomes of patients who survive TCA. Particular attention was placed on the variation of reporting and definitions of these outcomes between studies.
Methods
This review was conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.16 The protocol for this study was registered with the International Prospective Register of Systematic Reviews.
Inclusion criteria
Eligible studies included observational cohort studies that enrolled patients who experienced cardiopulmonary arrest following trauma and reported neurological outcomes. Studies examining pediatric patients were included. We excluded case reports, case series studies, reviews, and animal studies. Studies published in the English language were included. There were no restrictions on the length of follow-up, geographical location, or publication date.
Study selection and data abstraction
A systematic search of Embase, Medline, PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and ProQuest was conducted from the inception of the database to July 2020. A librarian with methodological and content expertise was consulted to create the search strategies (online supplemental table 1). Medical subject headings and Emtree headings were used in their respective databases.
Supplemental material
Two reviewers (DS and CM) independently screened the title and abstract of all included studies. Duplicate studies were removed using Covidence.17 Studies that met the inclusion criteria were reviewed in full text by the same two reviewers independently (figure 1). Disagreements were resolved by consensus or by the decision of a third independent reviewer (CE). Interobserver agreements for the title/abstract and full text stages were calculated using Cohen’s κ statistics.18
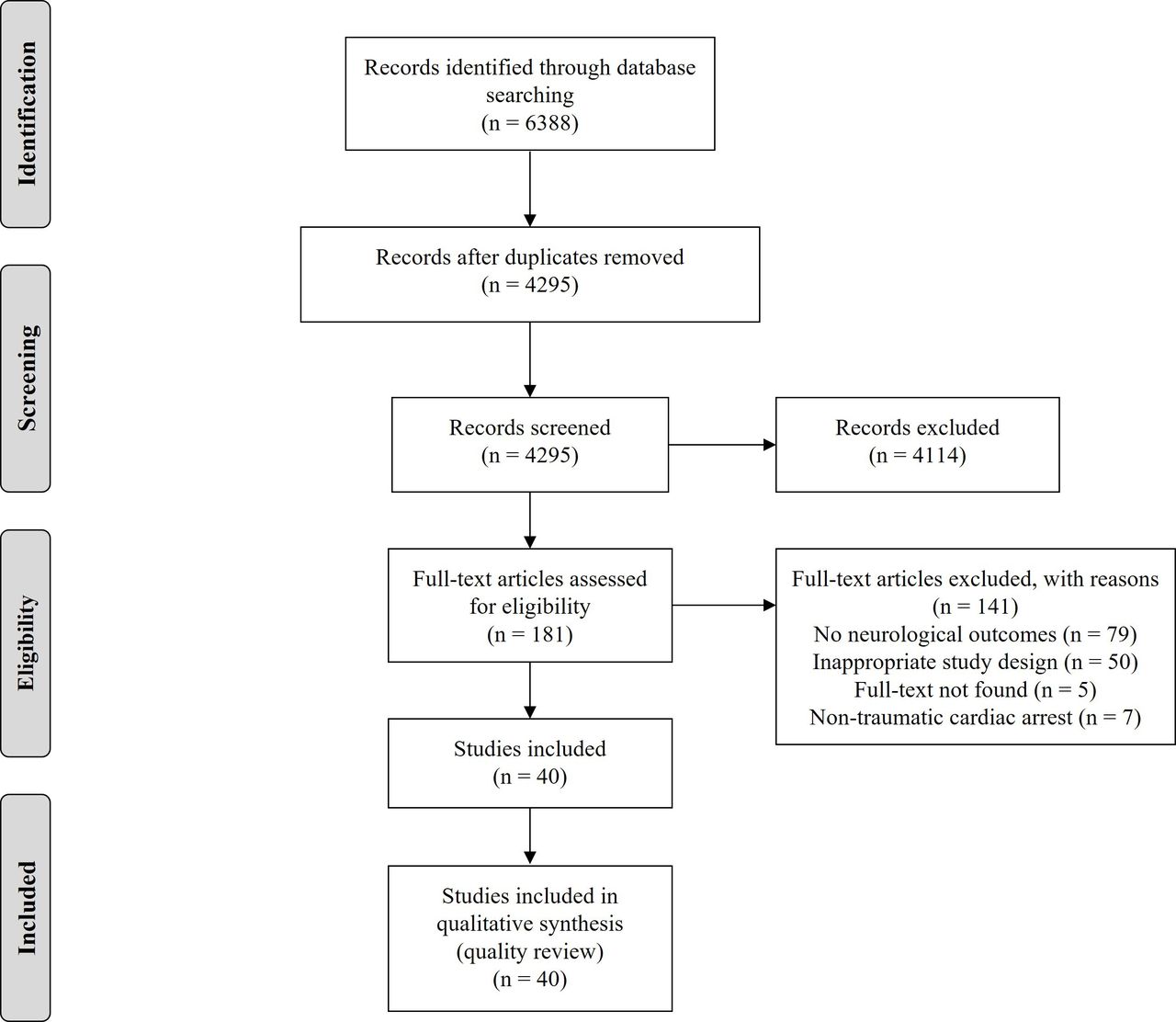
{kind=link}
PRISMA diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data were abstracted by two independent reviewers using a piloted data abstraction form (Microsoft Excel). The primary outcome was the neurological status of TCA survivors which was abstracted from each study. Additionally, the methods used to assess neurological outcome, the mechanism of trauma, and the time point when neurological status was measured were abstracted.
Data analysis
Patients from the included studies were placed into one of four categories to describe their neurological outcome: good, moderate, poor, or vegetative. A “good” neurological outcome was defined as a full neurological recovery or having minor deficits. A “moderate” outcome was defined as having neurological disability that partially affects daily activities but having full independence. A “poor” outcome was defined as requiring any level of dependency or personal assistance in daily living. A “vegetative” outcome was defined by unresponsiveness to external stimuli and a decreased level of awareness.
The proportion of patients with “favorable” neurological outcomes (ie, patients with good or moderate outcome) versus patients with “unfavorable” neurological outcomes (ie, patients with poor or vegetative outcome) was also calculated.
Quality assessment
The quality of included studies was assessed using ROBINS-I (Risk of Bias in Non-Randomized Studies - of Interventions) tool for observational studies. The overall risk of bias was rated as critical, serious, moderate, or low. Quality assessment was completed by two independent reviewers (DS and CM), with all conflicts resolved by consensus or discussion with a third reviewer (CE).
Results
Study characteristics
After the removal of duplicates, the literature search generated 4295 citations for title and abstract review. One hundred and eighty-one qualified for full-text screening, of which 40 were included in our analysis (figure 1). The title and abstract screening showed almost perfect agreement (κ=0.83), and similar agreement was found for the full-text screening (κ=0.87). Of the included studies, 35 were retrospective cohort studies and 5 were prospective cohort studies (table 1). The included studies were published between 1983 and 2019, with 12 studies published in the past 5 years.
Characteristics of included studies
Patient characteristics
There were 23 644 patients included, with 2168 (9.2%) surviving to hospital discharge. The mortality rate was 90.8%. Blunt trauma (n=8687 patients) and penetrating trauma (n=3489 patients) were the main mechanisms of traumatic arrest, whereas the remaining trauma mechanisms were not classified (n=11 468) (table 1). Nine studies examined pediatric patients only (n=1714 patients), 9 studies examined adults only (n=3821 patients), and 22 studies examined a mixed population (n=18 109 patients) without providing information of how many pediatric patients were included.
Neurological outcome reporting
Seventeen studies qualitatively described their neurological outcome based on patient disposition after discharge (eg, home, nursing care, or rehabilitation) and the level of assistance required in daily activities. Thirteen studies used the GOS and reported the number of patients in each GOS category (GOS 1–5). Eight studies used the CPC and one study used the Pediatric Cerebral Performance Categories (PCPC) to assess neurological outcome.
Seven studies dichotomized neurological outcomes into “good” or “poor” categories using the GOS, CPC, or PCPC scales. Six of the seven studies considered a “good” neurological outcome as patients with CPC 1 and 2 or GOS 4 and 5 (ie, good, mild, or moderate deficits) and a “poor” neurological outcome as those with CPC 3 and 5 or GOS 1 and 3 (ie, severe or vegetative). One study used the PCPC and defined a “good” outcome as PCPC 1 and 2 (good or mild deficits) and a “poor” outcome as PCPC 3 and 5 (moderate or severe deficits, or vegetative).
One study used the FIM to assess neurological status. This study reported an average FIM score for the survivors and the number of patients who had obtained the lowest score (required assistance in daily life). The functional status of the other patients was not reported.
Neurological status was recorded primarily at patient discharge, but some studies reported outcomes up to a 4-year follow-up period.
Overall neurological outcomes
The neurological outcomes of individual studies are reported in table 2. Based on the 32 studies (n=1507 patients) that reported the number of patients for each neurological outcome category, 538 (35.7%) had good outcomes, 392 (26.0%) had moderate outcomes, 408 (27.1%) had poor outcomes, and 169 (11.2%) were vegetative.
Neurological outcomes of included studies
In six studies (n=115 patients) that reported dichotomous outcomes, 62 patients (53.9%) had “good” outcomes and 53 patients (46.1%) had “poor” outcomes. In the one study (n=38 patients) that used the PCPC, 12 (31.6%) had “good” outcomes and 26 (68.4%) had “poor” outcomes. One study (n=184 patients) that used the FIM reported an average score of 38.9 (range: 18–126), 7 patients with severe deficits and 177 patients that had either good recovery or moderate or severe deficits.
Based on all 40 studies (n=2168 patients) included in this review, 992 (45.8%) had favorable outcomes, 630 (29.0%) had unfavorable outcomes, and 546 (25.2%) were missing. The results of the studies that used the PCPC and the FIM were included in the missing category, as the neurological status of the survivors was unclear and could not be categorized.
Neurological outcomes for pediatric studies
Of the seven studies (n=87 patients) that examined only pediatric populations and reported the number of patients for each neurological outcome category, 37 (42.5%) had good outcomes, 19 (21.8%) had moderate outcomes, 18 (20.7%) had poor outcomes, and 13 (14.9%) were vegetative. Hence, 56 patients (64.4%) had favorable outcomes and 31 (35.6%) had unfavorable outcomes.
Neurological outcomes for adult studies
Of the nine studies (n=164 patients) that examined only adult populations, 119 patients (72.6%) had favorable outcomes, 41 (25.0%) had unfavorable outcomes, and 4 (2.4%) had missing outcomes. Of the six studies (n=129 patients) that reported the number of patients for each neurological outcome category, 87 (67.4%) had good outcomes, 15 (11.6%) had moderate outcomes, 6 (4.7%) had poor outcomes, 17 (13.2%) were vegetative, and 4 (3.1%) had missing outcomes.
Assessment of quality
The quality of all included studies (n=40 studies) was assessed. Twenty-eight studies were at a serious risk of bias and 12 studies were at a moderate risk of bias (table 3). In general, the studies were well reported. The confounding domain was the primary source of bias, as most studies did not consider many potential confounders, including age, resuscitation technique, and type of trauma. The outcome measurement domain was also a significant source of bias, as most studies used physician-reported neurological outcomes, which were described qualitatively in the studies. Hence, these studies were rated as a serious risk of bias in this domain. Finally, there was moderate to serious risk of bias for selective reporting, as some studies did not report outcomes for each neurological category.
Quality review of included studies
Discussion
The current review is the first study to focus on neurological outcomes across a large patient population (n=23 644 patients). We report a survival rate of 9.2%, which is one of the most optimistic findings to date for outcomes following TCA. In the current review, favorable neurological outcomes were frequently reported (45.8% with full recovery or moderate disability), suggesting that outcomes from TCA may be more favorable than previously expected.3
Previous literature suggests that prognosis after traumatic arrest is extremely poor. Many studies reported only a small number of survivors, all with severe neurological disability.3 14 19 20 However, in 2012, new studies were conducted and a systematic review found that good and moderate neurological outcomes were reported in 57.4% of survivors.15 A large retrospective study published in 2016 supports these findings and reported good and moderate neurological outcomes in up to 75.0% of survivors.21 Despite these findings, neurological outcomes continue to be debated, as newer studies with larger numbers of survivors report good and moderate outcomes in only 4.3% to 27.0% of survivors.22 23 The findings of the current review suggest that those who survive traumatic arrest may have a favorable prognosis. The observed improvement in neurological outcomes is likely connected to novel advances in damage control resuscitation and refinement of treatment of guidelines.7
A secondary aim of this review was to assess the quality of the reporting of neurological outcomes. In most of the included studies, neurological status was qualitatively described. As the exact deficits were often not described, it was difficult to quantify the extent of the impairments and classify the neurological outcomes of these patients. Alternatively, patient disposition (eg, home, nursing care, rehabilitation) and dependence on daily support had to be used as indicators of neurological status. Furthermore, as an outcome measurement scale was not used, there is likely some degree of variation and biases among physician-reported outcomes. Several included studies reported dichotomous outcomes using a standardized scale by combining CPC 1 to 2 (good and moderate) as a “good” outcome and CPC 3 to 5 (severe, vegetative, death) as a “poor” outcome. However, the definition of a “good” and “poor” outcome varied between studies as CPC 3 was historically considered a “good” outcome.24 This reflects the differing values and preferences in the evaluation of neurological outcomes after arrest; therefore, reporting the exact deficits of the survivors is a key component of their neuroprognostication, as there may be a large difference between a moderate disability and a fully recovered patient.
Although the GOS and CPC scales were commonly used, alternatives such as the mRS and the GOSE were not used in any of the included studies. The CPC is heavily weighted toward mental functions and has been criticized for being inadequate to assess functional status at hospital discharge,25 26 which is supported by significant variability in quality-of-life measures for patients with similar CPC scores.27 28 Alternatively, the mRS and GOSE scales consider work capacities, social activities, and return to social life.9 11 29 However, most studies assessed neurological status at discharge, which may be inadequate regardless of the scale used. Most criteria rely on whether patients can perform daily activities, which are not undertaken while in hospital.11 As cardiac arrest survivors tend to report cognitive impairment and restricted societal participation after hospital discharge,30 early assessments may overestimate the neurological outcomes. Hence, repeated assessments over time with multiple scales are recommended to accurately assess the functional progression of these patients.
This review has several limitations. To start, our overall neurological outcome may be an overestimate given that patients with moderate deficits and favorable discharge dispositions were assumed to have a favorable outcome. Furthermore, the favorable neurological recovery rate that we provide here is based on a diverse patient population and does not account for the mechanism of trauma (blunt vs. penetrating), the patient age group (adult vs. pediatric), the time point when neurological status is assessed, or special resuscitative techniques. Previous literature has demonstrated varying effects of these factors in neurological outcomes. The effect of the mechanism of injury on traumatic arrest outcomes has been controversial. Whereas some cohort studies suggest that good outcomes can be achieved in select patient groups, especially in those with penetrating injuries,31 32 other studies suggest that the mechanism of injury is not associated with better outcomes (neurological recovery or survival).22 33 Hence, it would be valuable to assess the effect of the mechanism of injury on the neurological recovery following arrest. Although only a few studies assess traumatic arrest in the pediatric population, there is a general consensus that the functional outcomes are poorer compared with adults.15 34 35 In the length of follow-up after cardiac arrest, there is evidence that significant recovery can occur between 1 and 6 months36 and long-term recovery after 1 year.37 The majority of the studies we included assessed neurological outcomes at patient discharge or after resuscitation (table 2), suggesting that we underestimated the prevalence of good neurological recovery in the current review. Special resuscitative techniques, such as emergency thoracotomy and therapeutic hypothermia, have some demonstrated benefits in neurological outcomes after traumatic arrest for select patient populations.38–42 Based on the effects of these factors on neurological recovery, we recommend for future studies evaluating outcomes after traumatic arrest (1) reporting the mechanism of injury for survivors in each neurological outcome category, (2) reporting the age group (adult vs. pediatric) in each neurological outcome category, (3) assessing neurological outcomes 1 year after the arrest if resources allow or >30 days if necessary,36 and (4) reporting special resuscitative techniques in individual survivors in each neurological outcome category.
Overall, the strength of the scientific evidence for neurological outcomes after TCA is low. Although we identified some large national registry studies, most studies were retrospective cohorts.4 5 43 Five prospective studies were included, but only one was a multicenter study.44 Furthermore, our quality assessment revealed a moderate to serious risk of bias in our included studies due to confounding and selective reporting domains. Our outcome of interest was often qualitatively described, and some studies briefly reported neurological outcomes for only one category (eg, vegetative state). As a result, many studies without sufficient data were excluded, and the extent of the selective reporting bias we identified may be an underestimate.
Good and moderate neurological outcomes are frequently reported in patients who survive TCA. However, stronger evidence is needed to prognosticate this patient population as neurological outcomes are often inadequately reported. Future studies should identify and adjust for appropriate confounding variables and report the prevalence of each neurological category. Multicenter prospective studies that focus on the quality of survivorship are urgently needed.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Si Hong Yu (Health Sciences Librarian at Queen’s University) for his help with the development of the search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at This study was presented as an oral presentation at the Annual Meeting of the Trauma Association of Canada in a virtual format on April 12, 2021.
Contributors DS, CM, and CE conceived the study design. DS and CM created the literature search. DS and CM collected data and conducted the quality assessment with assistance from CE. DS drafted the article. CM prepared the figure and tables, and all authors contributed substantially to revision. All authors take responsibility for the article as a whole. DS is the guarantor of the article and accepts responsibility for the integrity of the published work.
Funding External funding was received from the Queen’s Department of Emergency Medicine in the Emergency Medicine Summer Studentship Award (DS and CM).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.