Article Text

Abstract
Background Hemorrhagic shock is a major cause of mortality in low-income and middle-income countries (LMICs). Many institutions in LMICs lack the resources to adequately prescribe balanced resuscitation. This study aims to describe the implementation of a whole blood (WB) program in Latin America and to discuss the outcomes of the patients who received WB.
Methods We conducted a retrospective review of patients resuscitated with WB from 2013 to 2019. Five units of O+ WB were made available on a consistent basis for patients presenting in hemorrhagic shock. Variables collected included gender, age, service treating the patient, units of WB administered, units of components administered, admission vital signs, admission hemoglobin, shock index, Revised Trauma Score in trauma patients, intraoperative crystalloid (lactated Ringer’s or normal saline) and colloid (5% human albumin) administration, symptoms of transfusion reaction, length of stay, and in-hospital mortality.
Results The sample includes a total of 101 patients, 57 of which were trauma and acute care surgery patients and 44 of which were obstetrics and gynecology patients. No patients developed symptoms consistent with a transfusion reaction. The average shock index was 1.16 (±0.55). On average, patients received 1.66 (±0.80) units of WB. Overall mortality was 13.86% (14 of 101) in the first 24 hours and 5.94% (6 of 101) after 24 hours.
Discussion Implementing a WB protocol is achievable in LMICs. WB allows for more efficient delivery of hemostatic resuscitation and is ideal for resource-restrained settings. To our knowledge, this is the first description of a WB program implemented in a civilian hospital in Latin America.
Level of evidence Level IV.
- global surgery
- whole blood
- hemorrhage
- shock
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Hemorrhagic shock kills an estimated 1.9 million people annually worldwide.1 Prompt management of hemorrhagic shock is essential. Several decades of experience have shown that extensive volume resuscitation with crystalloid can lead to an exacerbation of the “lethal triad” of trauma-induced coagulopathy, hypothermia, and acidosis2–5; this phenomenon has recently been modified to include hypocalcemia and therefore has been termed the “lethal diamond.”6 Evidence during the past decade suggests a more balanced resuscitation involving the replacement of lost blood with a 1:1:1 transfusion with red blood cells (RBCs), fresh frozen plasma (FFP), and platelets, mimicking the whole blood (WB) that is lost.7–9 Adherence to a 1:1:1 ratio, however, remains challenging even in high-resource settings.10 Many regions of the world do not have the blood bank capabilities to adequately supply and respond to the challenging demands of providing and sustaining a timely and efficient 1:1:1 resuscitation strategy.11 12 As such, there has been renewed interest in WB transfusion programs as an initial approach to damage control resuscitation.
Hospital Vicente Corral Moscoso (HVCM) is a public hospital located in Southern Ecuador and serves as a referral center for more than two million inhabitants.13 A WB transfusion program was implemented in 2013 to address the issue of inadequate hemostatic resuscitation for patients in hemorrhagic shock. The aims of this article are to describe the logistics of the implementation of a WB transfusion protocol at our institution, review the outcomes of exsanguinating trauma and acute care surgery (TACS) and obstetrics and gynecology populations who received WB, and demonstrate the feasibility of a WB program in a low-income and middle-income country (LMIC).
Methods
We performed a mixed methods analysis of the WB resuscitation program at the HVCM. To document the details of the program, we interviewed members of the blood bank staff, hospital administration, and clinical leadership of the hospital who were instrumental in establishing the program. To characterize the safety profile of WB transfusions in our program, we identified patients who received WB transfusion from 2013 to 2019. The following datapoints were collected: sex, age, service treating the patient, units of WB administered, units of components administered, admission vital signs, admission hemoglobin, shock index, intraoperative crystalloid and colloid administration, length of stay, and in-hospital mortality. In trauma patients, the Revised Trauma Score (RTS) was calculated. We also collected information suggestive of symptomatic acute transfusion reactions including evidence of anaphylaxis, urticaria, rash, jaundice, hemoglobinuria, and respiratory difficulty in the immediate post-transfusion period. No laboratory tests were sent post-transfusion to detect subclinical transfusion reactions. Post-transfusion laboratory values were not available in all patients.
We used SPSS V.26 for statistical analysis.
Results
WB transfusion protocol at the HVCM
Five units of type O+ WB were made available daily and released to patients presenting in hemorrhagic shock, as determined by the attending surgeon taking care of the patient. There is often a delay of only a few minutes in starting WB transfusion once it is ordered by a physician as five units are always set aside for patients presenting in shock. After the type O+ WB is dispensed, the blood bank then proceeds to type and cross the patient using Bio-Rad Saxo ID-Reader (Bio-Rad Laboratories Saxo ID-Reader, Herculues, CA, USA). Initial resuscitation was begun in the emergency department and extended into the operating room in most cases, or is begun in the operating room. Given resource limitations, a warming device was not routinely available. The patient is transfused with WB until vital signs stabilized per the clinical judgment of the attending surgeon or until the blood bank is depleted of WB, after which type-specific RBCs and FFP are dispensed according to their availability in the blood bank. The decision to transition from WB to component therapy is not based on laboratory parameters at our institution as point-of-care laboratory tests are not available at our institution to allow for rapid decision making. The resuscitation strategy at the HVCM is largely based on clinical examination, as tools such as thromboelastography used at some institutions to guide blood-based resuscitation are not available.
Blood donation and collection
WB is obtained through voluntary unpaid donation or replacement donation. These practices enabled a consistent supply of five units of WB available at all times. The blood must be collected in no more than 12 minutes with constant manual or mechanical activation so as to prevent the activation of the clotting cascade. The use of aseptic technique is paramount for quality control and prevention of bacterial contamination. The sterile material used in this process is disposable. The extraction bags are quadruple bags including CPD+SAG-Mannitol Buffy-Coat. The filtration system is used only when the blood is fractionated into components.
WB processing, storage, and administration
After a unit of blood is donated, it is quarantined for 8 hours, during which time the ABO type and Rh (D) type are determined. The WB is screened for the following serologic markers according to the WHO standards14: syphilis, hepatitis C, hepatitis B and HIV. Plasma antibody titers are not measured prior to the transfusion of WB. If the blood tests negative for infectious diseases, it is refrigerated at 4°C to 6°C and available for 48 hours. As such, the product dispensed at the HVCM is considered cold, fresh WB. Donation, processing, and dispensing of the cold, fresh WB occurred in the same facility within HVCM.
Leukoreduction is not routinely performed on the units of WB due to the inability to preserve platelets. After 48 hours, if the blood is not used, it is fractionated into components. The RBCs and frozen plasma are then made available for up 35 to 42 days and 1 year, respectively. Platelets are not available to patients at the HVCM after fractionation. Given the relative scarcity of blood products in the region, the platelets obtained through fractionation are primarily sent to the local cancer hospital. The blood bank stock is then replaced by the aforementioned methods, thereby minimizing any interruptions in blood product availability. At our hospital, a 48-hour cut-off has allowed for balance of the need for WB in the hemorrhaging patient and hemocomponents for other patients within the hospital.
Outcomes of patients managed with WB
There were 101 TACS or obstetrics and gynecology patients identified to have received resuscitation with WB. Fifty-seven patients presented to the TACS service and 44 patients presented to the obstetrics and gynecology service, with an average shock index of 1.16 (±0.55) (table 1). Admission vital signs and laboratory values can be found in table 2.
Demographics of patients receiving whole blood transfusion (N=101)
Admission vital signs and laboratory values of patients resuscitated with whole blood
On average, TACS patients received 1.75 (SD±0.93) units of WB, and obstetrics and gynecology patients received 1.55 (SD±0.59) units of WB. An average of 1.91 (SD±2.68) and 1.74 (SD±1.91) units of packed red blood cells (pRBCs) were administered to TACS and obstetrics and gynecology patients, respectively, after WB. An average of 1.30 (SD±2.59) and 0.84 (SD±1.86) units of FFP were administered to TACS and obstetrics and gynecology patients, respectively, after WB. Platelets, as previously mentioned, are rarely available at our institution.
TACS patients
Of the 57 patients on the TACS service, 47 were trauma patients and 10 were emergency general surgery patients. The average RTS in the trauma population was 6.06 (±1.89) and the average shock index was 1.18 (±51). Anatomic injury data were not available to calculate the Injury Severity Score. Of the 47 trauma patients, 24 suffered penetrating trauma and 23 suffered blunt trauma. Hemorrhage was localized in the abdomen in 12 (25.53%) patients, thorax in 11 (23.40%) patients, extremities in 10 (21.27%) patients, thorax and abdomen in 6 (12.76%) patients, face in 2 (4.26%) patients, pelvis in 2 (4.26%) patients, spine in 1 (2.13%) patient, and neck in 1 (2.13%) patient. In the case of two patients (4.26%), the cause of hemorrhage was unknown as these patients died prior to complete assessment.
The remaining 10 patients were emergency general surgery patients. WB transfusion was used for intraoperative bleeding in a patient undergoing a repair of a ruptured abdominal aortic aneurysm (n=3, 30.00%), an open necrosectomy for infected pancreatic necrosis (n=1, 10.00%), a bowel resection for ischemic gut (n=1, 10.00%), a repair of an iliac artery aneurysm (n=1, 10.00%), repair of the superficial femoral artery after excision of a left groin mass (n=1, 10.00%), control of gallbladder fossa hemorrhage after laparoscopic cholecystectomy (n=1, 10.00%), control of splenic hemorrhage after splenic biopsy (n=1, 10.00%), and control of hypogastric artery bleeding after spinal surgery (n=1, 10.00%).
Length of stay in the intensive care unit was 4.79 (SD±5.85) days, and overall length of stay was 13.07 (SD±15.33) days in TACS patients.
Obstetrics and gynecology patients
Forty-four patients presented to the obstetrics and gynecology service, with an average shock index of 1.15 (±0.58). Thirty-six (81.81%) patients suffered postpartum hemorrhage either after cesarean section or vaginal delivery. Postpartum hemorrhage was found to be due to uterine atony in 18 (50.00%) patients, placenta accreta spectrum or placenta previa in 8 (22.22%) patients, a tear in the vaginal mucosa in 4 (11.11%) patients, retained products in 3 (8.33%) patients, and uterine rupture in 2 (5.56%) patients. One (2.78%) patient had bleeding from an extrauterine vessel after a cesarean section. The remaining eight patients (18.18%) suffered hemorrhage due to other gynecologic emergencies including incomplete abortion in three (37.50%) patients, ruptured ectopic pregnancy in two (25.0%) patients, fibroids in one (12.50%) patient, postoperative bleeding after hysterectomy in one (12.50%) patient, and a hemorrhagic ovarian cyst in one (12.50%) patient. The only mortality in this cohort died due to complications related to hemorrhage from Hemolysis, Elevated Liver enzymes and Low Platelets (HELLP) syndrome.
Length of stay in the intensive care unit was 1.84 (SD±2.77) days, and overall length of stay was 5.86 (SD±4.56) days in obstetrics and gynecology patients.
Adverse outcomes
Importantly, none of the patients in our series developed symptomatology consistent with acute transfusion reaction. This includes anaphylaxis, urticaria, rash, jaundice, and hemoglobinuria per the records from both the nurse and the primary surgical team. No patients were diagnosed with Transfusion-related acute lung injury (TRALI) or transfusion-associated circulatory overload (TACO) in the medical record. However, many of these patients were critically ill and therefore intubated in the perioperative period, making the diagnosis challenging. The cause of death in one trauma patient who suffered massive hemorrhagic shock from a penetrating brachial artery injury was noted to be massive pulmonary edema in the setting of multisystem organ failure. This could be consistent with a diagnosis of TRALI.
Overall mortality was 13.86% in the first 24 hours and 5.94% after 24 hours. The shock index of patients who died in the first 24 hours and after 24 hours was 1.42 (SD±0.64) and 1.29 (SD±0.48), respectively. By comparison, patients who survived had an average shock index of 1.09 (SD±00.53). Of those patients who died in the first 24 hours after transfusion, the cause of death was attributed to hemorrhage in 11 patients, 3 of whom arrested prior to any operative intervention, 6 of whom arrested in the operating room, and 3 of whom arrested shortly after surgery. The two remaining patients died due to a subarachnoid hemorrhage and irreversible shock postoperatively. One death in the maternal population occurred due to hemorrhage in a patient presenting with HELLP syndrome, severe pre-eclampsia, and intrauterine fetal demise. The patient was found to have evidence of severe coagulopathy and a hepatic hematoma after undergoing a cesarean section; this patient unfortunately died before operative intervention could be undertaken.
Of the six patients who died after 24 hours, three suffered sepsis leading to multisystem organ failure. Two patients were declared brain dead and one patient suffered irreversible shock after blunt force trauma to the chest not responsive to treatment.
Discussion
The HVCM is at the forefront of using WB transfusion in patients with hemorrhagic shock in Latin America. Our experience shows that WB transfusion represents a feasible strategy for achieving hemostatic resuscitation in patients presenting in hemorrhagic shock, especially in LMICs. Through the implementation of a WB program, we were able to establish a program where patients would receive balanced resuscitation. Prior to the implementation of a WB program, patients were resuscitated with whatever components were available in the blood bank, which included a varying and often scarce number of pRBCs and FFP. The products dispensed from the blood bank and administered were not reliably documented, making a comparison before and after the implementation of this program impossible. Of the patients resuscitated with WB, we do not describe any symptoms consistent with transfusion reactions.
The use of WB is not a new concept. Prior to the adoption of component therapy in 1970s, resuscitation of patients in hemorrhagic shock with WB was commonplace.15 Component therapy was popularized for logistical reasons and was never proven to be as efficacious as WB in hemorrhagic shock.16 Recent literature from the military suggests that WB may have superior or equivalent outcomes when compared with component therapy. Two retrospective combat casualty analyses compared the use of fresh WB with component therapy.17 18 One study described a mortality benefit in the WB group at 24 hours and 30 days,18 whereas the other found no statistically significant difference in mortality, death due to exsanguination, multisystem organ failure, or sepsis.17 Nessen et al19 showed that, in the experience with forward surgical teams in Afghanistan, use of Fresh whole blood (FWB) in addition to RBCs and FFP was associated with improved in-hospital survival compared with RBCs and FFP alone. Within the civilian sector, retrospective analyses suggest superiority or equivalence of WB with regard to mortality and overall blood product use.20–23 The only randomized control trial in trauma patients, to our knowledge, compared modified WB (leukoreduced WB with additional platelet transfusion) with component therapy. After excluding patients with traumatic brain injury, a decrease in the use of component therapy was demonstrated in patients who received modified WB.24
A recent systematic review and meta-analysis comparing WB with component therapy found no difference in 24-hour or 30-day mortality. Importantly, this study highlighted the heterogeneity in the literature on WB transfusion in trauma. No study in this analysis was from the civilian setting in an LMIC.25 WB has important implications in LMICs, of which our work is only scratching the surface.
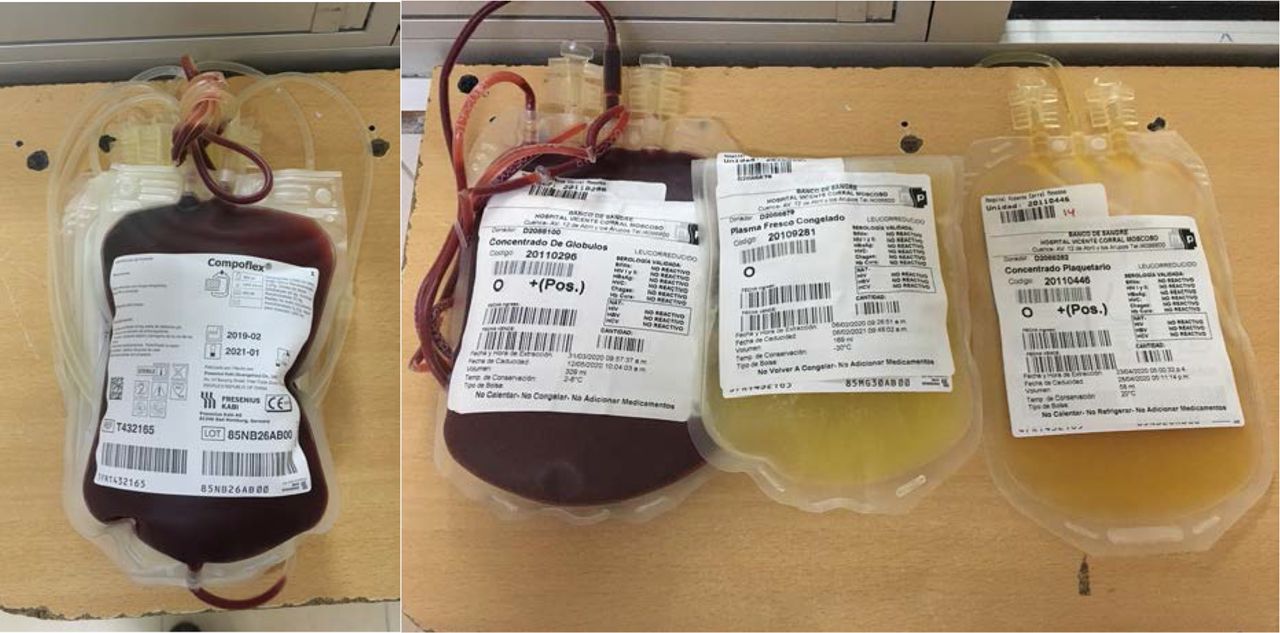
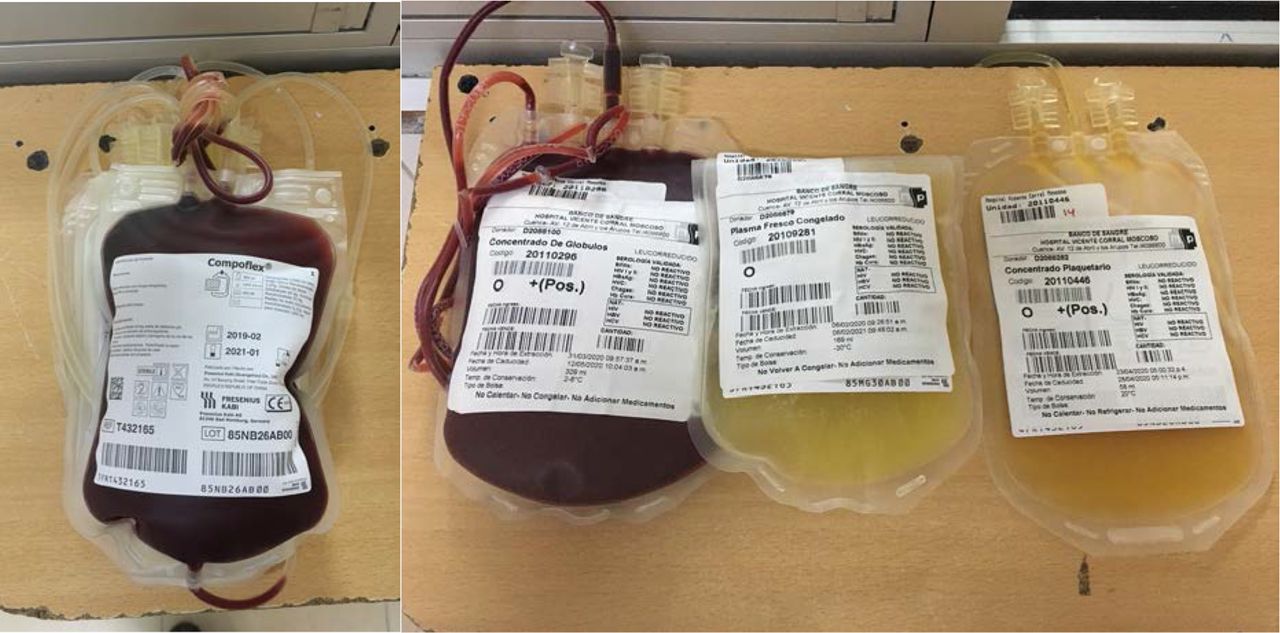
WB has both financial and logistical benefits compared with component therapy.26 WB has the advantage of being easy to store, transport, and administer to patients. Its use is ideal for resource-constrained environments and prehospital settings,16 27 especially those that do not have ready access to all blood components, delivering the product that would otherwise require three bags in one bag (figure 1).16 Moreover, when separated components are transfused, each unit contains an increased amount of anticoagulants and additives that contribute to a patient’s overall coagulopathy compared with one unit of WB.18 28 Spinella et al18 found that, in patients receiving massive transfusion, those receiving component therapy received a median of 825 mL of additional additives and anticoagulants compared with the group resuscitated with WB. Additionally, it has been asserted that the administration of WB may actually be safer for patients with respect to risk of transmission of bloodborne diseases, exposing them to one donor instead of multiple donors.29
{kind=link}
(Left) One unit of cold, fresh whole blood. (Right) One unit of packed red blood cells, fresh frozen plasma, and platelets.
Access to transfusion therapy and the “blood drought” create significant barriers to safe surgery in LMICs.30 The use of WB is potentially beneficial in countries where keeping up with a 1:1:1 transfusion ratio is not feasible. In resource-limited settings such as our institution in Southern Ecuador, a WB program has allowed us to streamline the prompt and expeditious administration of all blood components at once, thus ensuring higher concentrations of all primordial elements and thereby securing hemostatic strategy for patients in hemorrhagic shock. Prior to the implementation of this program, there was no way to guarantee the availability of balanced hemostatic resuscitation to patients in hemorrhagic shock.
It must be noted that Cuenca, Ecuador provides a favorable setting for implementing a WB program as 80% population is type O+ and 2% is type O− per the blood bank records.31 In our sample, most patients had type O+ blood, thereby making it easier to identify donors and more likely that a patient receiving a type O+ transfusion will be receiving a transfusion from a donor with the same blood type. The context for transfusion of patients in our region is distinct from the literature that typically recommends transfusion at a hemoglobin of 7 g/dL.32 Located at 2560 m above sea level, the average hemoglobin in this population is higher than at lower altitudes, estimated to range between 14.6 g/dL and 15.2 g/dL in women and 16.8 g/dL and 17.4 g/dL in men.33 As such, patients at our institution are often transfused at a higher threshold, typically 9 g/dL to 10 g/dL.
The primary concern with the transfusion of group O WB to non-group O recipients involves the possibility of minor ABO mismatch. This is typically mitigated by transfusion of only type-specific WB or through the transfusion of whole units with low titers of antibody (most commonly <256 by the saline dilution, immediate spin method), known as low-titer O whole blood (LTOWB).16 Numerous studies documented the safety of LTOWB, demonstrating that it does not increase risk of transfusion reaction.15 16 20 21 29 34 35 ,36 However, at the HVCM, anti-A and anti-B titers are not measured prior to administration of blood products. Data supporting the transfusion of untitered WB are scarce in the literature. In a safety analysis of the transfusion of stored WB, Yazer et al23 found that there was no statistically significant difference in the amount of incompatible plasma transfused in a unit of WB compared with the amount of incompatible plasma transfused in any unit of platelets (p=0.38). Sperry et al recently demonstrated a rate of adverse events possibly related to transfusions of 2.2% in a description of AB plasma and A plasma with low-titer B antibodies administered to patients in hemorrhagic shock in the prehospital setting.37 Severe intravascular hemolytic transfusion reactions caused by minor mismatch are a relatively rare phenomenon19 that may be difficult to detect in an otherwise critically ill patient and may not have been detected with the n of 101 in our series. While, again, we do not report any patients who developed symptomatology that was recognized as a hemolytic transfusion reaction, hemolysis laboratory tests post-transfusion were not routinely ordered. Several studies have documented that WB does not have evidence of increased hemolytic reactions with administration of up to four units.20 21 38
This study is limited in that it is a single-institution and retrospective study. There are many challenges that come with conducting research in a resource-limited setting, many of which affected this study. Although more patients were identified than described, many files were unable to be located in medical records. Documentation at HVCM continues to be written by hand, and many of the patient charts in medical records are missed pages or written illegibly. It should also be noted that documentation prior to the implementation of the TACS service (2012) was scarce. As such, the ability to compare this sample with patients resuscitated during an earlier time period is limited. The paucity of data in the paper charts also limited our ability to reliably determine the vital signs and laboratory values after transfusion.
Conclusion
In summary, our experience demonstrates that WB administration in patients presenting with hemorrhagic shock can be an achievable alternative therapy to 1:1:1 resuscitation especially in settings with limited resources, where access to all blood products may not be feasible. Further studies comparing WB with component therapy in this population are needed. To our knowledge, this is the first description of a WB program implemented in a civilian setting in Latin America.
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the ethical committee of our institution, Hospital Vicente Corral Moscoso, and the academic committee of research of the University of Azuay Medicine Faculty.
References
Footnotes
Contributors Data collection, data analysis, article writing: AH. Data collection, article writing: MEGA. Data collection, data analysis: JRN, DSA, SGPP. Critical review of the article: NFL, RPA, HSA, LFdC, CCA. Critical review of the article, final approval of the article for submission: JCP, JCS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.