Article Text

Statistics from Altmetric.com
Case presentation
A teenage man was involved in a forklift rollover resulting in a crush injury to his pelvis, left thigh, and right forearm. He presented to a level three trauma center with a Glasgow Coma Scale of 15 and was stabilized, including endotracheal intubation, placement of a left chest tube for pneumothorax, application of a right upper extremity tourniquet, application of a pelvic binder, and massive transfusion. Angiography was performed for pelvic bleeding concerns and demonstrated thrombosis at the iliac bifurcation (figure 1).
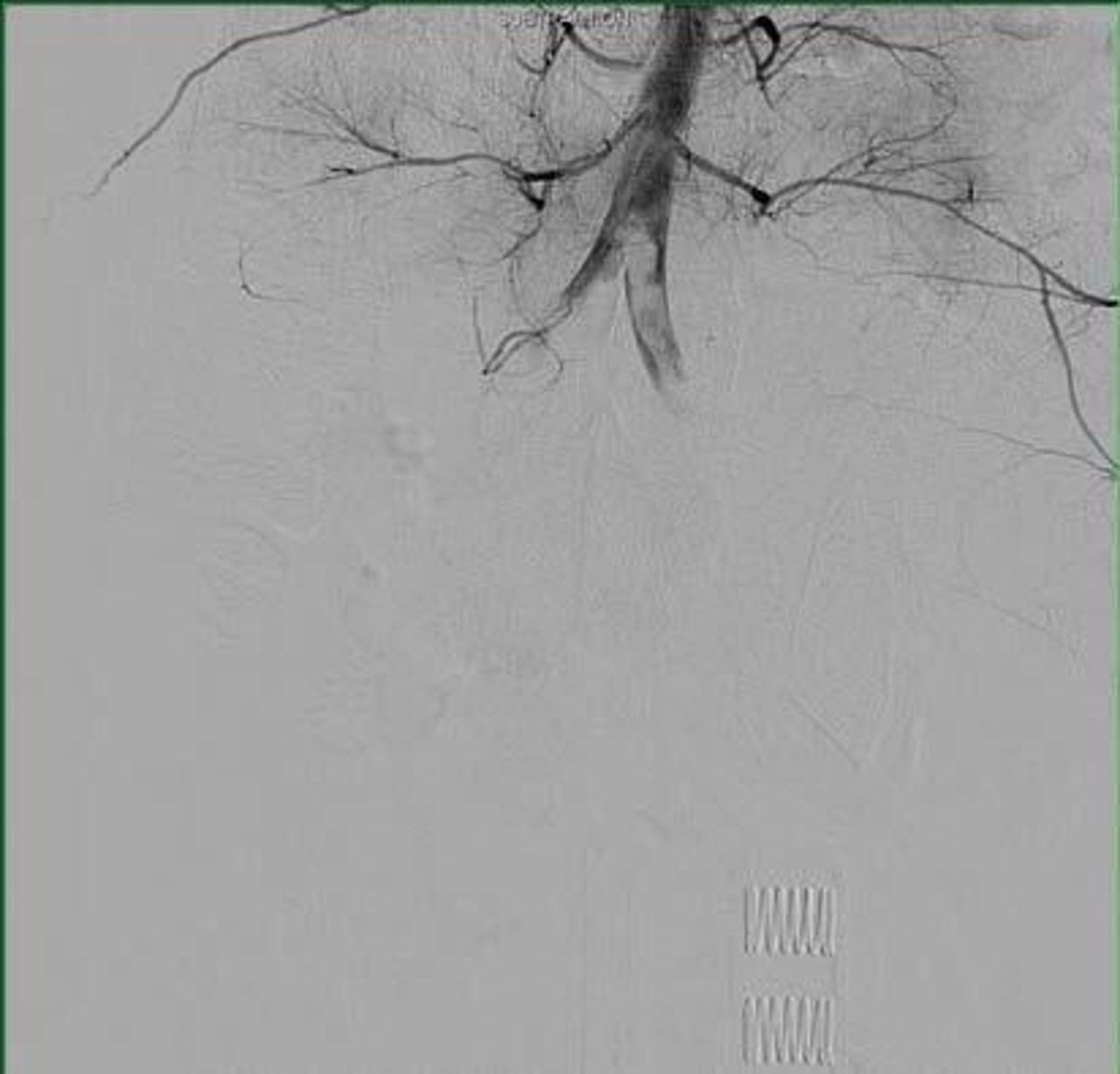
Angiography demonstrating obstructed flow at the level of the common iliac arteries bilaterally.
Due to the complexity of his injuries, he was transferred to a level one trauma center where his examination was notable for a large left groin wound with gross feculent contamination. He had significant left thigh and perineal degloving and absence of bilateral lower extremity pulses. His right upper extremity remained with a tourniquet in place above the elbow, and nearly complete amputation distally. The patient was taken immediately to the operating room where he was found to have ischemic left colon and rectum, perineal degloving, and avulsion of the bladder dome. He sustained catastrophic disruption of his pelvic ring including spinopelvic dissociation, severe comminuted fractures throughout the entire left innominate bone, and complete dissociation of the right hemipelvis (figure 2). All bone was dysvascular. There were no viable targets for revascularization of the right lower extremity. The right upper extremity was ischemic and not viable distal to the tourniquet, which had been in place for greater than 6 hours.

3D CT reconstruction of the pelvic bones demonstrating significant bony destruction.
The sigmoid colon and rectum were resected and the ureters ligated. The Orthopedic team performed an acute internal left hemipelvectomy. On the right, an above knee guillotine amputation was performed, allowing more proximal tissue to demarcate viability for later coverage. The right upper extremity was amputated above the elbow. The patient was transferred to the intensive care unit for ongoing resuscitation.
On hospital day (HD) 1, the patient underwent percutaneous placement of bilateral nephrostomy tubes. On HD2, he returned to the operating room for creation of an end colostomy and additional debridement, leaving him with a non-viable right pelvis, including the innominate and sacrum, genitalia, and right lower extremity. On HD4, he was extubated, allowing for a multidisciplinary goals of care discussion with the patient and his family. The patient determined his goal was for longevity and recovery.
What would you do?
Advise comfort measures.
Aggressive debridement with attempt at primary closure.
Hemicorporectomy with non-permanent mesh.
Hemicorporectomy with permanent mesh.
What we did and why
Removal of the non-viable tissue required amputation through the L4/L5 disk space with ligation of the thecal sac to prevent cerebrospinal fluid leakage. Necrotic pelvic bone, genitalia, muscle, and soft tissue of the abdominal wall were debrided. The iliac vessels were resected to the level of the common iliacs and oversewn. A temporary abdominal closure was applied with bowel bag covering the open pelvic floor.
On HD7, the patient returned to the operating room for closure of his abdomen. A 35 by 35 cm Phasix ST mesh (Becton, Dickinson and Company, Franklin Lakes, NJ), constructed of knitted absorbable monofilament poly-4-hydroxybutyrate fibers coated with a hydrogel, was used to re-enforce the lower abdomen and create a sling for the abdominal contents. The mesh was laid into the retroperitoneum with the coated side facing the abdominal contents. We made two slits to accommodate the ends of the ureters that were brought up to sit on top of the mesh. We folded the mesh and cut a slit anteriorly to produce a more conical shape, which we plicated with non-absorbable suture. We then fixed the mesh laterally to the fascia and muscle of the body wall bilaterally. Approaching from below, we sutured the mesh to the fascia overlying the lumbar spine. We then fixed the mesh to the anterior abdominal fascia lateral to the rectus bilaterally. The bilateral rectus muscles and paraspinous muscles were closed together in two layers over the mesh, and skin was closed primarily over two drains (figure 3). The patient’s hospital course was complicated by pulmonary embolism, ileus, pneumonia, intra-abdominal abscess, and acute respiratory failure.

{kind=link}
{kind=link}
{kind=link}
Patient’s lower abdomen at the time of final debridement (A) and after closure of hemicorporectomy (B).
Durable closure of the abdominal cavity was a concern when formalizing the hemicorporectomy. Intra-abdominal mesh placement was chosen to recreate some structure to the lower abdomen, with the goal to prevent evisceration while not further diminishing pulmonary capacity. The field had been highly contaminated and there is limited guidance in the published research regarding mesh use for hemicorporectomy after injury. However, extrapolating from mesh use in a contaminated field during closure of the abdomen after trauma laparotomy, use was considered reasonable. Absorbable, coated mesh was selected to reduce the adhesive burden should the patient later require additional abdominal operations, such as urostomy creation. One year postoperatively, he has completed his inpatient rehabilitation and is living at home.
Ethics statements
Ethics approval
This case report was conducted following the University of Washington policy on case reports. This policy requires a HIPPA release obtained from the subject of the report.
Acknowledgments
The authors would like to acknowledge the entire multidisciplinary team who provided outstanding care in this case.
Footnotes
Contributors Guarantor: SPM. Idea and literature review: ML and SPM. Writing: ML and SPM. Photographs: SPM. Critical editing of article: LM, CB, CPK, and BR.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, nor the U.S. Government.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.