Article Text

Statistics from Altmetric.com
Case description
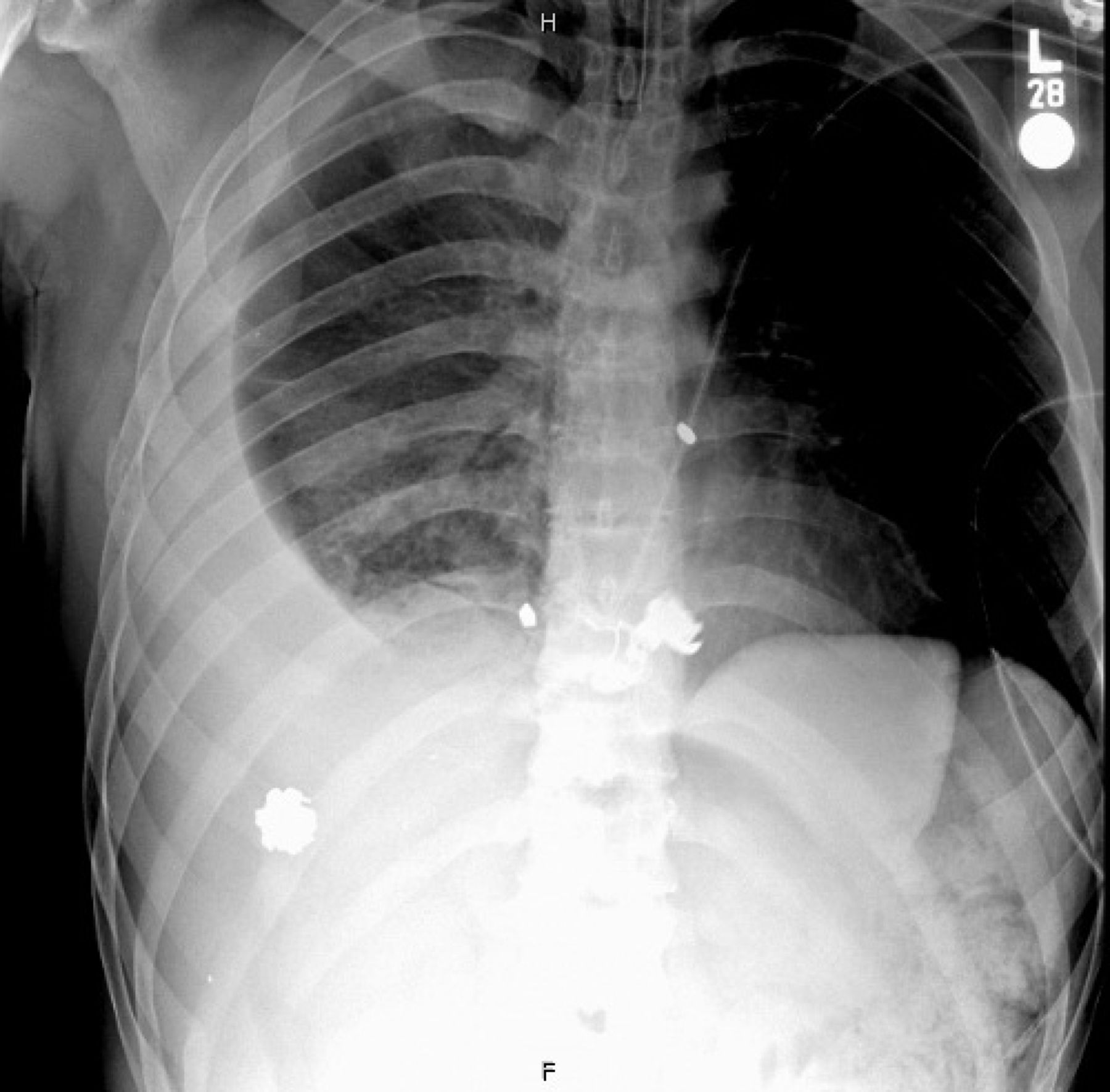
This is a case of a patient in his 20s who presented with seven gunshot wounds to his extremities and abdomen. On arrival, the patient was intubated, and the massive transfusion protocol was initiated. Focused abdominal sonogram for trauma (FAST) demonstrated questionable pericardial fluid and positive intraperitoneal fluid. Chest radiography (chest X-ray; CXR) demonstrated a right hemopneumothorax, right lateral fifth rib fracture, right anterior fifth costal cartilage fracture and bullet shrapnel overlying right hemithorax (figure 1).
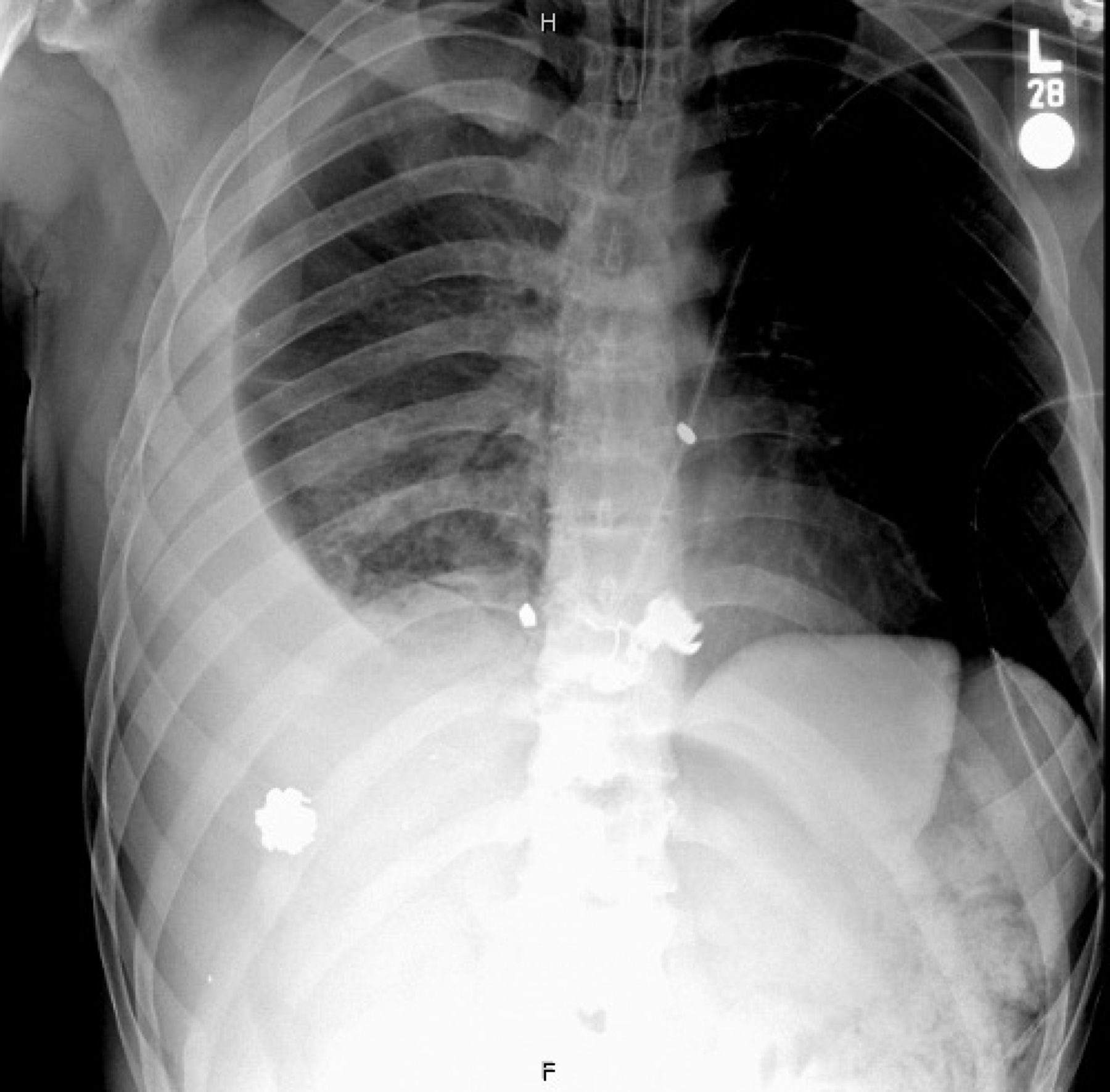
Chest X-ray taken in the trauma bay showing bullet shrapnel overlying right hemithorax and mid-chest with large right-sided hydropneumothorax and opacification of right lung. Cardiomediastinal silhouette is partially obscured by the right lung. Right-sided rib fracture is also noted.
The patient was taken emergently for an exploratory laparotomy. He was found to have ballistic injuries to his liver (caudate and dome), diaphragm, stomach and colon. He underwent posterior stomach wedge resection, resection of distal colon and was left in discontinuity. Due to the possible pericardial effusion seen on FAST, an intraoperative transesophageal echocardiography (TEE) was performed by the cardiac anesthesiology team, which was determined to be normal. At the end of the case, a temporary abdominal closure was placed, and he was transferred to the surgical intensive care unit.
Postoperatively, completion CT was obtained. This demonstrated multiple bullet fragments over the right upper quadrant, pelvis, and surprisingly, in the right atrium at the atrioventricular junction and tricuspid valve with possible right atrial wall injury (figure 2). The patient had continued transfusion requirements.

Chest CT with lung window showing ballistic fragment in the right atrium at the atrioventricular junction/valve, no pericardial collection, and a collapsed inferior vena cava.
What would you do next?
Continue resuscitative care given normal intraoperative TEE.
Placement of right chest tube.
Consult vascular surgery for endovascular repair.
Consult cardiothoracic surgery for sternotomy.
What we did and why
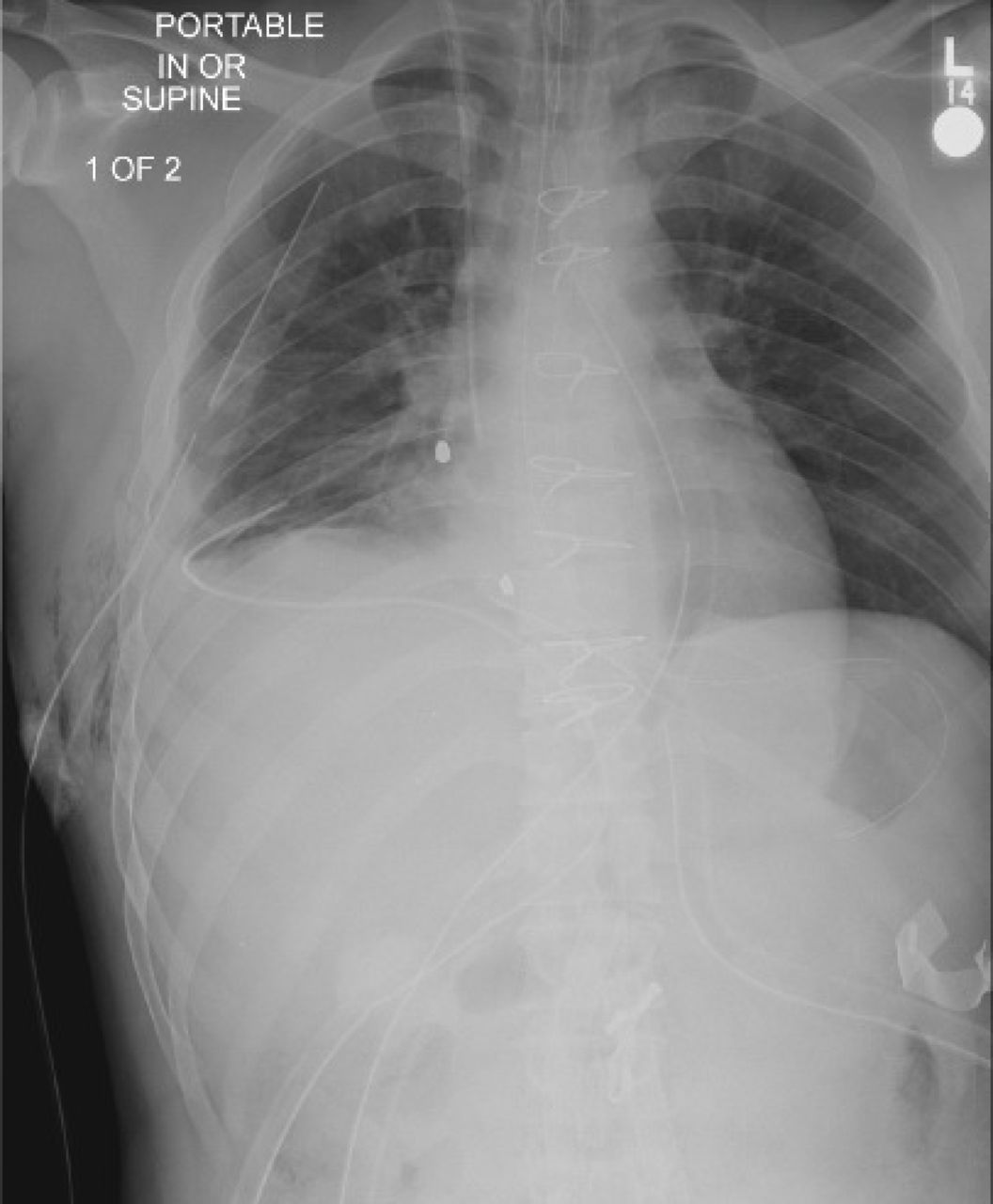
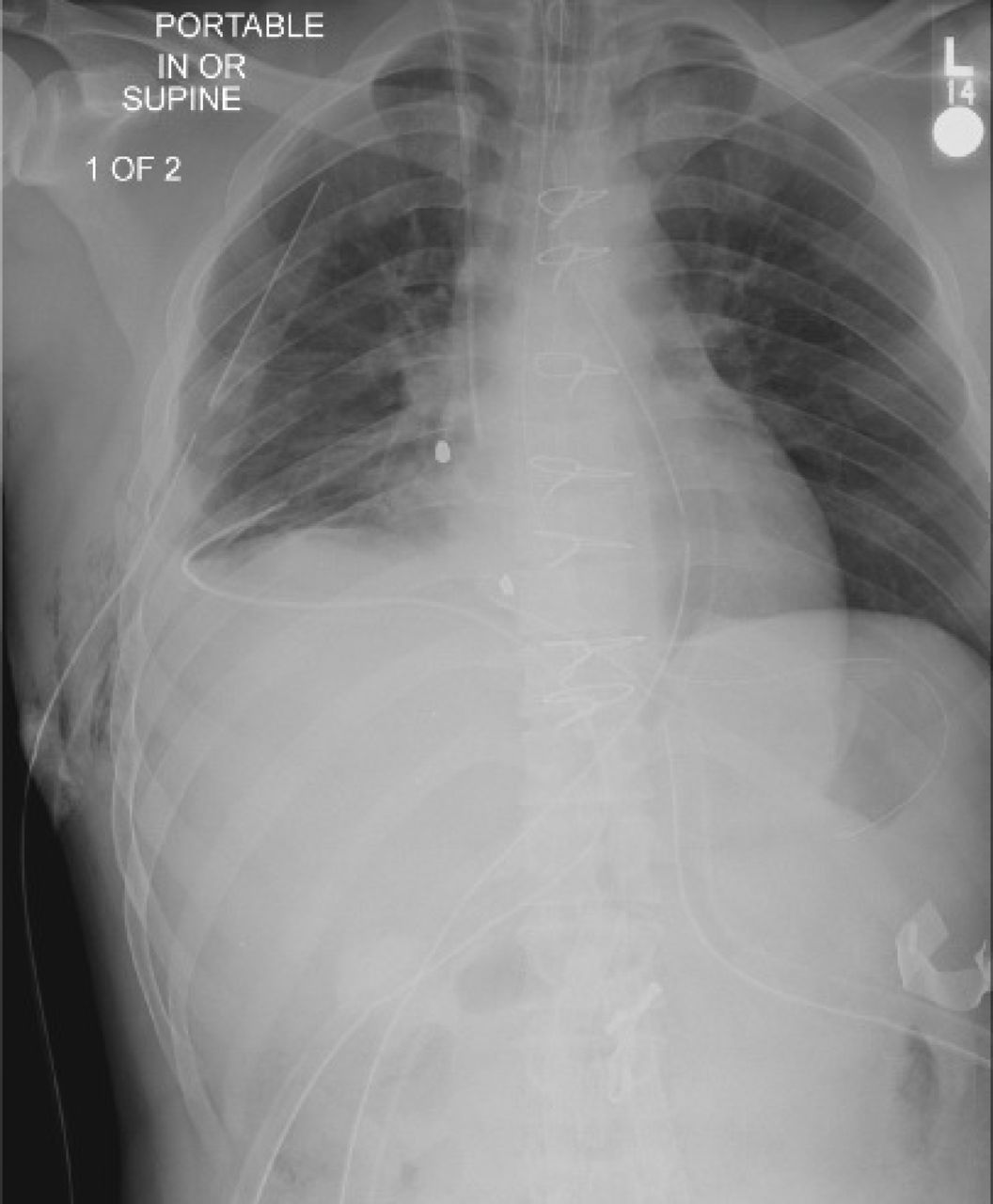
Cardiothoracic surgery was consulted, and a formal transthoracic echocardiography (TTE) was completed, now showing a bright 2.3×1.3 cm echodense object in the right atrium with collapsed inferior vena cava (IVC). Given the patient’s continued hemodynamic instability, the decision was made to return to the operating room. Interestingly, a second TEE done by anesthesia intraoperatively was negative again for intracardiac injuries. The patient was placed on cardiopulmonary bypass and a right atriotomy was performed where the bullet was found entangled in the tricuspid valve leaflet and posterior leaflet. His postoperative CXR demonstrated interval removal of bullet fragments (figure 3). The following day, the patient returned to the operating room for colostomy, left hemidiaphragm repair and primary abdominal closure. He continued to do well and was discharged 3 weeks later. He ultimately underwent an elective redo sternotomy and tricuspid valve repair.
{kind=link}
{kind=link}
{kind=link}
Postoperative CXR after median sternotomy with removal of bullet fragment. Two small bullet fragments remain projecting over the right cardiac border.
Bullet embolism is an extremely rare phenomenon among the 32 000 deaths and over 67 000 injuries caused by firearms each year. This case elucidated lessons regarding both diagnosis and management. The diagnosis of bullet emboli can prove to be clinically challenging, particularly in the setting of a hemodynamically unstable trauma patient. Our case demonstrates an unfortunate case of an initially undetected bullet embolus. On review with a cardiac radiologist, both TEEs performed by anesthesia were incomplete examinations. On the transgastric view, the ultrasonographer looked at only the left ventricle, mitral valve and aorta, but did not turn the probe to capture the tricuspid valve, which would have shown the bullet. Additionally, the four-chamber view looked at only the septal and anterior leaflets, whereas the bullet was lodged in the posterior leaflet. These lapses highlight the importance of complete examinations, preferably conducted by cardiologists, and especially in the context of a high suspicion for cardiac injury.
Given these findings, our patient’s bullet likely embolized in transit to the hospital as there were no myocardial surface injuries. Bullet embolism into the systemic circulation is usually arterial. Our patient had a venous bullet embolism to the right heart. We think it originated from one of the liver lacerations, entered a large hepatic vein or the IVC, and traveled to the right heart. While it is not possible to definitively confirm the source, we hypothesize that the bullet did not enter the retrohepatic IVC directly given the extent of hepatic vein injuries and lack of IVC injuries on the CT scan. Additionally, the bleeding would have been torrential, which it was not.
Due to the rarity of bullet emboli cases, there are controversies related to management. It is generally agreed that arterial or paradoxical emboli should be retrieved as soon as diagnosed given the high risk of ischemic complications. Although venous bullet embolization can be asymptomatic, the complications include valvular destruction, endocarditis, sepsis, venous thrombosis and hypoxia. Therefore, it is generally accepted that symptomatic venous emboli require extraction. For asymptomatic patients, there is debate between expectant versus operative removal, and open versus endovascular techniques. In our case, the patient was hemodynamically unstable with continued transfusion requirements, tricuspid regurgitation and the possibility of further embolization to the pulmonary vasculature, which prompted surgical exploration. Due to the location of the bullet, in the tricuspid leaflet, a sternotomy with arteriotomy was the ideal approach.
Overall, this case demonstrated lessons on diagnosis and management of a rare firearm sequelae.
Footnotes
Contributors YZ is the first author and was responsible for drafting the article. MP and WB are both surgical residents who were involved in the case and provided critical revisions. AG, RDB, and KAD are attending surgeons who contributed to patient care and decision-making. SAJB is a trauma radiology attending who helped in reviewing the images. FL is the senior author and an attending surgeon who was responsible for project oversight.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Patient provided phone consent due to COVID-19 restrictions
Provenance and peer review Not commissioned; internally peer reviewed.