Article Text

Statistics from Altmetric.com
Case summary
Duodenal stump blowout is a feared complication of Billroth II reconstruction after gastrectomy. Most commonly presenting in the early postoperative period, there is significant variation in the surgical management of the difficult duodenal stump due to complexity. Here, we report a highly unusual case of a delayed duodenal stump perforation secondary to a golf-ball sized enterolith without evidence of a cholecystoenteric fistula or afferent loop obstruction in a patient with a remote history of distal gastrectomy with Billroth II reconstruction. An 84-year-old man status post vagotomy and antrectomy with Billroth II reconstruction for peptic ulcer disease (PUD) 40 years ago presented with the acute onset of abdominal pain of 6 hours duration. The patient had focal peritonitis in the right upper quadrant (RUQ), hypoxia requiring 3 L of oxygen by nasal cannula and tachycardia with heart rate of 100 beats per minute. Laboratory findings were significant for a leukocytosis of 14 820/µL and metabolic acidosis. A CT scan demonstrated free air around the duodenal stump and RUQ stranding with a large hyperenhancing stone in the proximal duodenal stump and a normal gallbladder without pneumobilia (figure 1).

CT scan demonstrating enterolith and duodenal perforation.
What would you do?
Enteroscopic stone retrieval and percutaneous drainage.
Pancreaticoduodenectomy.
Exploration, stone extraction, cholecystectomy, primary duodenal repair.
Exploration, stone extraction, primary duodenal repair, drainage.
What we did and why
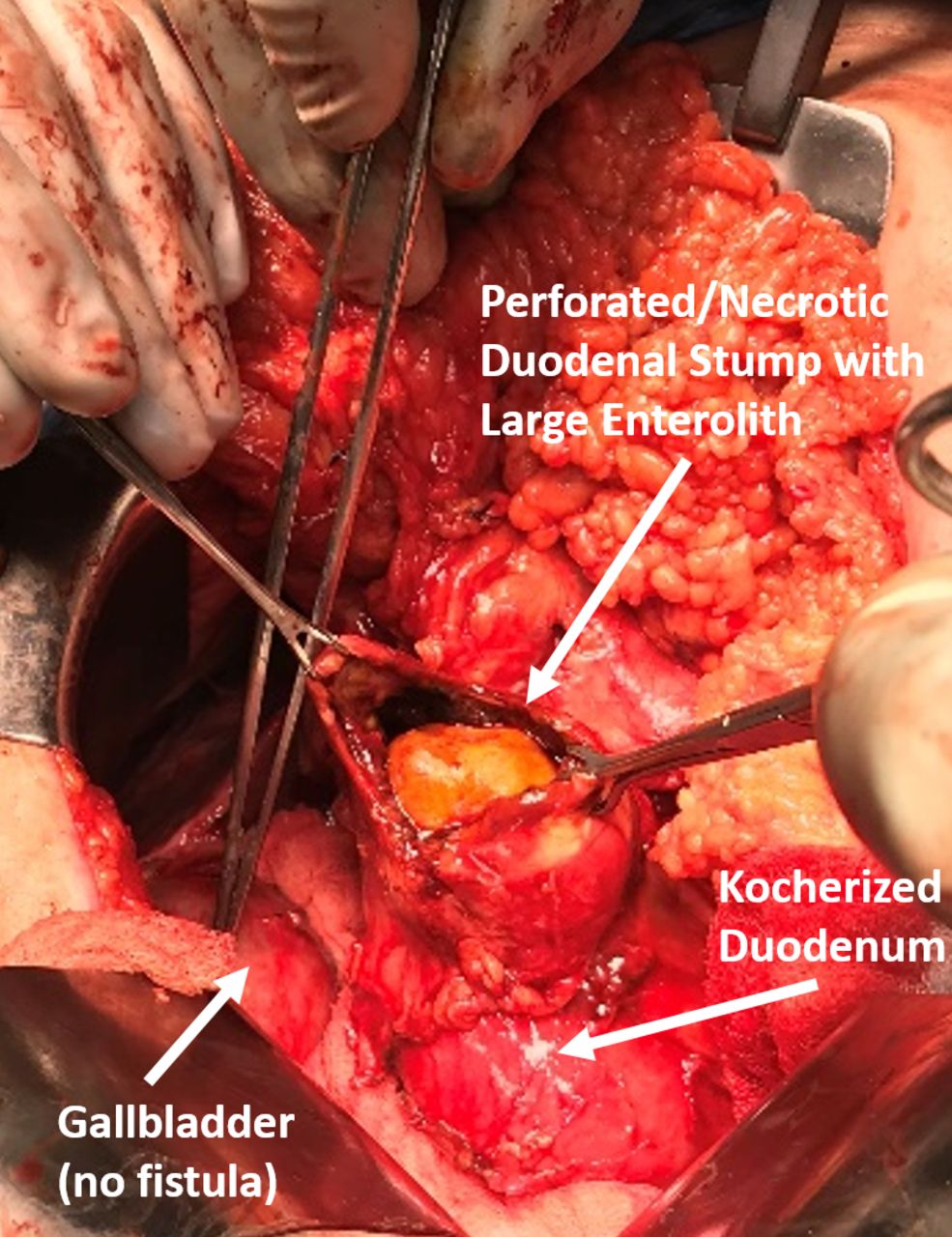
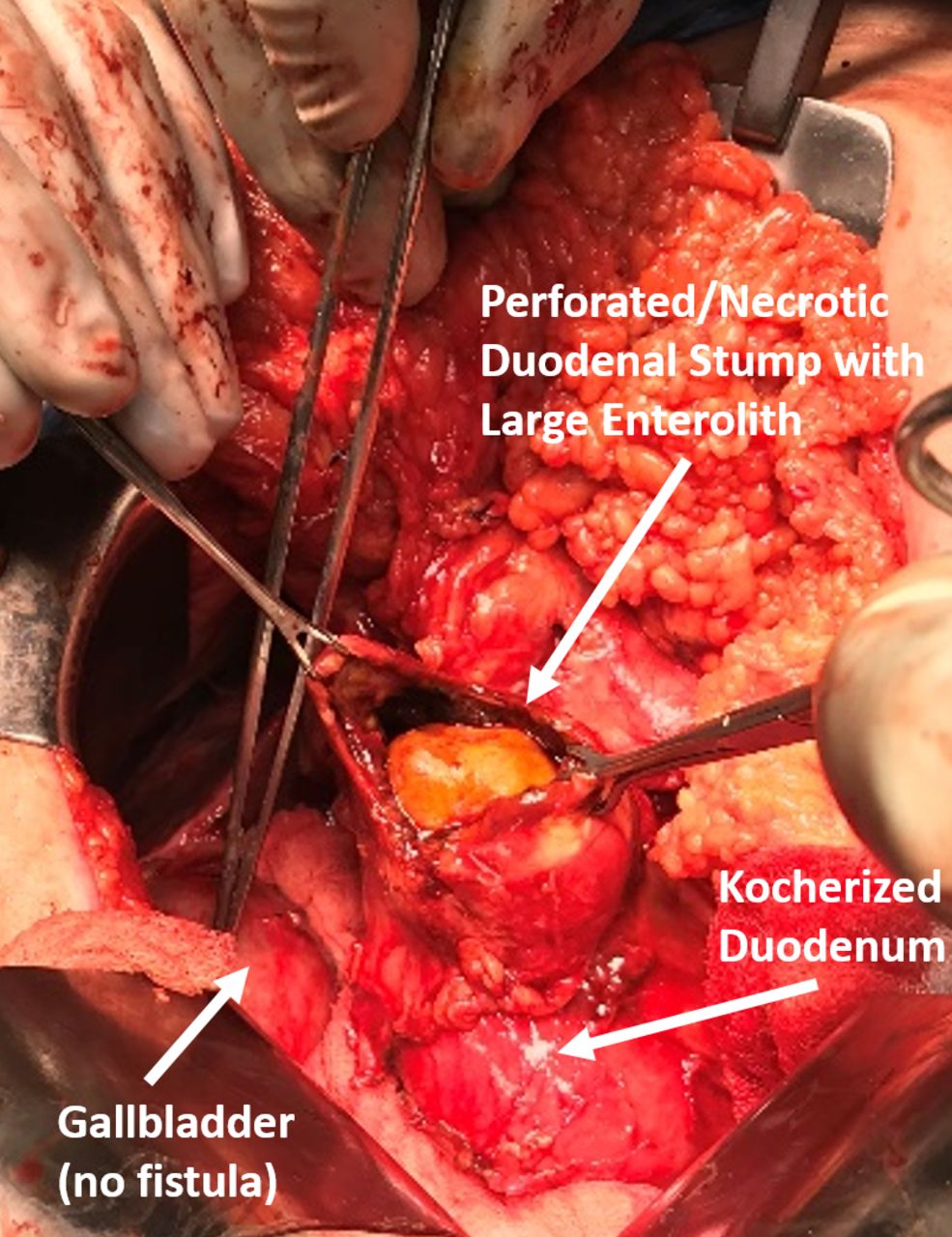
In this patient, immediate operative intervention was undertaken. After extensive adhesiolysis, a small amount of purulence was visualized in the RUQ around the duodenum. A perforation in the proximal duodenal stump secondary to direct erosion from a 3 cm gallstone was encountered. The duodenum was kocherized demonstrating no cholecystoduodenal fistula. The proximal duodenum in the area of perforation was friable and necrotic; however, the second and third portions of the duodenum were normal in course and caliber. The gallbladder was secondarily inflamed but felt normal without evidence of stones. The proximal duodenal stump was debrided to healthy bleeding tissue with immediate return of bile and a large stone was removed (figure 2). Through the duodenotomy, a normal appearing ampulla could be visualized/palpated 2–3 cm from the perforation with free extrusion of bile; therefore, we repaired the duodenum primarily without further evaluation of the biliary tree. Had the ampulla not been easily visualized, a cholecystectomy would have been performed with pediatric feeding tube placement through the cystic duct and exiting the ampulla to allow for direct visualization and palpation of the extrahepatic biliary tree to avoid iatrogenic injury with duodenal closure. Given the patient’s age and absence of preceding symptoms of colic, it was felt that the gallbladder was likely not the source, but rather stasis in the proximal afferent limb, now repaired flush to the ampulla, therefore we elected not to perform cholecystectomy. The duodenal wall was closed in layers. The repair was drained with two closed suction drains. Postoperatively, nasogastric decompression and antibiotics were maintained for 72 hours followed by slow resumption of enteral nutrition. The patient recovered without incident, discharging to home on the 7th postoperative day after removal of surgical drains and has been seen in follow-up with no further symptoms and doing well.
{kind=link}
{kind=link}
Duodenal stump perforation with enterolith.
A rare late complication after gastrectomy with reconstruction is duodenal stump blowout or afferent loop syndrome. Typically, afferent loop syndrome or duodenal stump blowout occur in the first 7 days from operation and are rare complications, occurring in 0.3%–5% of cases.1–3 However, recent case reports have highlighted unusual cases of afferent loop syndrome occurring decades after initial operation due to the formation of enteroliths, some of which have been managed with less invasive modalities.1 2 4–9 Enteroliths in the afferent loop can lead to obstruction and duodenal stump perforation and pose complex surgical decision-making to the acute care general surgeon.1 10
Historically, PUD was treated surgically. Advances in medical therapy and our understanding of PUD including H elicobacter pylori eradication and acid suppression have more than halved the incidence of operations for the treatment of PUD.11 With the ageing North American population, the acute care surgeon will be confronted with delayed complications of remote ulcer surgery such as the case described above.12
Footnotes
Contributors AEC contributed to the conception and design. SLB contributed to the critical revision, approval of final submission and supervised the study. All authors contributed to the writing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.