Article Text

Abstract
Background The Brain Trauma Foundation recommends intracranial pressure (ICP) monitor placement for patients with severe traumatic brain injury (TBI). Adherence with these guidelines in elderly patients is unknown. We hypothesized that disparities in ICP monitor placement would exist based on patient age.
Methods Using the National Trauma Data Bank (2010–2014), we identified patients admitted for blunt TBI with admission Glasgow Coma Scale (GCS) scores of 3–8. Patients were excluded if they had a non-Head Abbreviated Injury Scale (AIS) score ≥3, hospital length of stay <24 hours or were discharged from the emergency department. Demographic data, ICP monitor placement, GCS, AIS-Head, Injury Severity Score, and outcome measures were collected. Propensity score matching between ICP monitor and non-ICP monitor patients was used for logistic regression and Cox multivariate regression analyses.
Results Of the 30 710 patients with blunt TBI with GCS scores of 3–8 included in our study, 4093 were treated with an ICP monitor. ICP monitor placement rates significantly decreased with increasing age. Multivariable analysis demonstrated that patients treated with an ICP monitor were more likely to be younger, male, have private/commercial insurance, and receive care at an institution with three or more neurosurgeons.
Conclusion Patients ≥65 years of age with severe blunt TBI are less likely to be treated with an ICP monitor than younger patients. Age disparities in adherence to Brain Trauma Foundation guidelines may alter the outcomes for patients with severe TBI.
Level of evidence Level IV.
- traumatic brain injury
- intracranial pressure monitor
- surgical disparities
- age disparities
- neurotrauma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Traumatic brain injury (TBI) is a considerable cause of morbidity and mortality in the USA. From 2007 to 2013, the number of TBIs sustained in the USA increased significantly.1 According to the Centers for Disease Control and Prevention, TBI was responsible for approximately 2.5 million emergency department visits, 300 000 hospitalizations and 56 000 deaths in 2013 alone.1 In addition to the increasing prevalence of TBI, these injuries significantly add to the national financial burden of healthcare, accounting for direct and indirect costs totaling $60 billion in the year 2000.2
Monitoring and control of intracranial pressure (ICP) have been studied as a means of reducing secondary insults after TBI.3 In the past 40 years many studies have looked at the efficacy of ICP monitor placement, but there is still a lack of consensus on indications for use.4 5 The Brain Trauma Foundation (BTF) has published guidelines for ICP monitor use, however the impact of these guidelines on patient outcomes remains uncertain.4 The most recent edition of the BTF guidelines recommends the use of ICP monitoring in patients with a survivable, severe TBI (defined as Glasgow Coma Scale, or GCS, scores of 3–8) with an abnormal CT scan.6 ICP monitoring may also be indicated in patients with severe TBI with a normal CT scan and two of the following features: age >40, unilateral or bilateral motor posturing, or systolic blood pressure <90 mm Hg.6 Since the publication of these guidelines, many studies have assessed their efficacy, with mixed results. A lack of consensus on the role of ICP monitoring in patients with severe TBI persists.
Elderly patients (aged 65 and older) have the highest rate of TBI-related deaths with mortality rates increasing in recent years.1 This elevated mortality rate has been attributed to the higher risk of falls in this age group. Despite the high risk of mortality in elderly patients with severe TBI, the evidence for ICP monitor efficacy in this subgroup is limited.7 There is a void in the literature on the effect of ICP monitoring specifically in the elderly, as well as whether or not deferring ICP monitor placement in these patients is appropriate. Our study was developed to evaluate for potential age disparities in ICP monitor placement. We hypothesized that ICP monitors would be placed less frequently in elderly patients with severe TBI compared with younger patients.
Methods
Study population
To assess a widely representative population of isolated patients with TBI, we used records submitted to the National Trauma Data Bank (NTDB) from 2010 to 2014. Of the 480 347 patients in the trauma registry, we identified those patients admitted for blunt TBI with admission GCS scores between 3 and 8. Patients were subsequently excluded if they had a hospital length of stay (LOS) <24 hours, were discharged from the emergency department, transferred out to another healthcare facility, or had a non-Head Abbreviated Injury Scale (AIS) score ≥3. Our methodology is shown in figure 1.
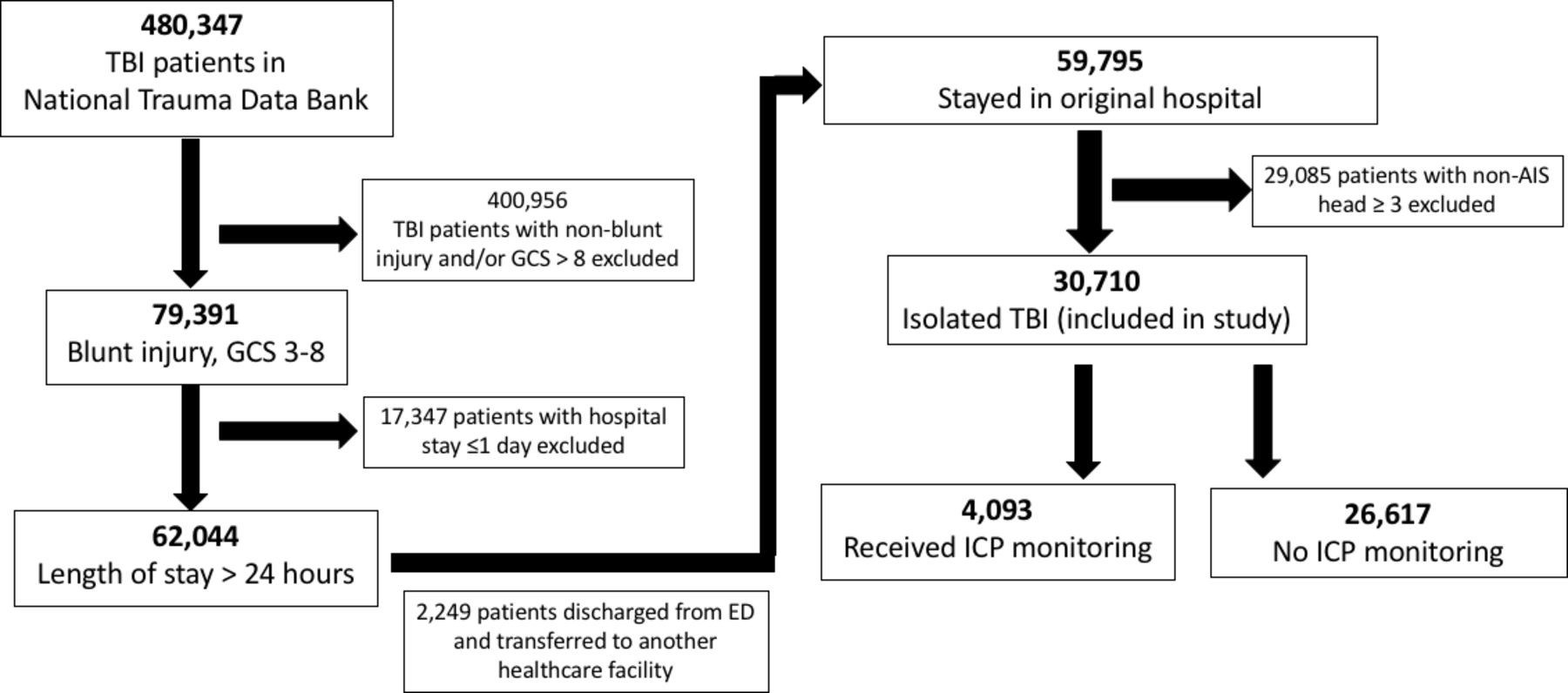
CONSORT diagram of study methodology using the National Trauma Data Bank. AIS, Abbreviated Injury Scale; ED, emergency department; GCS, Glasgow Coma Scale; ICP, intracranial pressure; TBI, traumatic brain injury.
Covariates
Demographic data collected on our study population included patient age, sex, race and insurance status. Clinical characteristics included mechanism of injury, GCS, AIS-Head, Injury Severity Score (ISS), rates of craniotomy/craniectomy and other neurosurgical procedures, types of intracranial injuries, ICP monitor placement, complications, hospital LOS, intensive care unit (ICU) LOS, and mortality. We also collected hospital teaching status, number of hospital beds and the number of neurosurgeons at the patient’s hospital.
Statistical analysis
All statistical analyses were computed via SPSS Statistics V.24, with a significance level of p<0.05. We used logistic regression to control for demographic and clinical parameters. To directly compare the ICP monitor versus non-ICP monitor groups we used a bivariate analysis.
Results
Demographics and clinical characteristics
The clinical characteristics of our study population can be found in table 1. After applying our study inclusion and exclusion criteria, we identified 4093 patients with blunt TBI with GCS scores of 3–8 who received an ICP monitor (table 2). Patients who received an ICP monitor were significantly younger than those not receiving a monitor (p<0.001). Patients who received an ICP monitor also had higher ISS (p<0.001), higher AIS-Head scores (p<0.001), and higher rates of neurosurgical procedures including craniotomy and craniectomy (both p<0.001). In addition, ICP monitor use was associated with a longer hospital stay (median 15 vs. 12 days, p<0.001), ICU stay (median 11 vs. 4 days, p<0.001), and more ventilator days (median 9 vs. 3 days, p<0.001). Patients treated with an ICP monitor were more likely to have private insurance, and a lower rate of ICP monitor placement was seen in Medicare patients (table 3). Hospitals staffed with at least three neurosurgeons favored ICP monitor placement. Finally, ICP monitor placement was associated with a higher rate of mortality (30.7% vs. 27.2%, p<0.001, table 2).
Demographics of patients with isolated traumatic brain injury
Demographics and clinical characteristics (NTDB 2010–2014)
Insurance status and hospital data (NTDB 2010–2014)
ICP monitor placement decreases with age
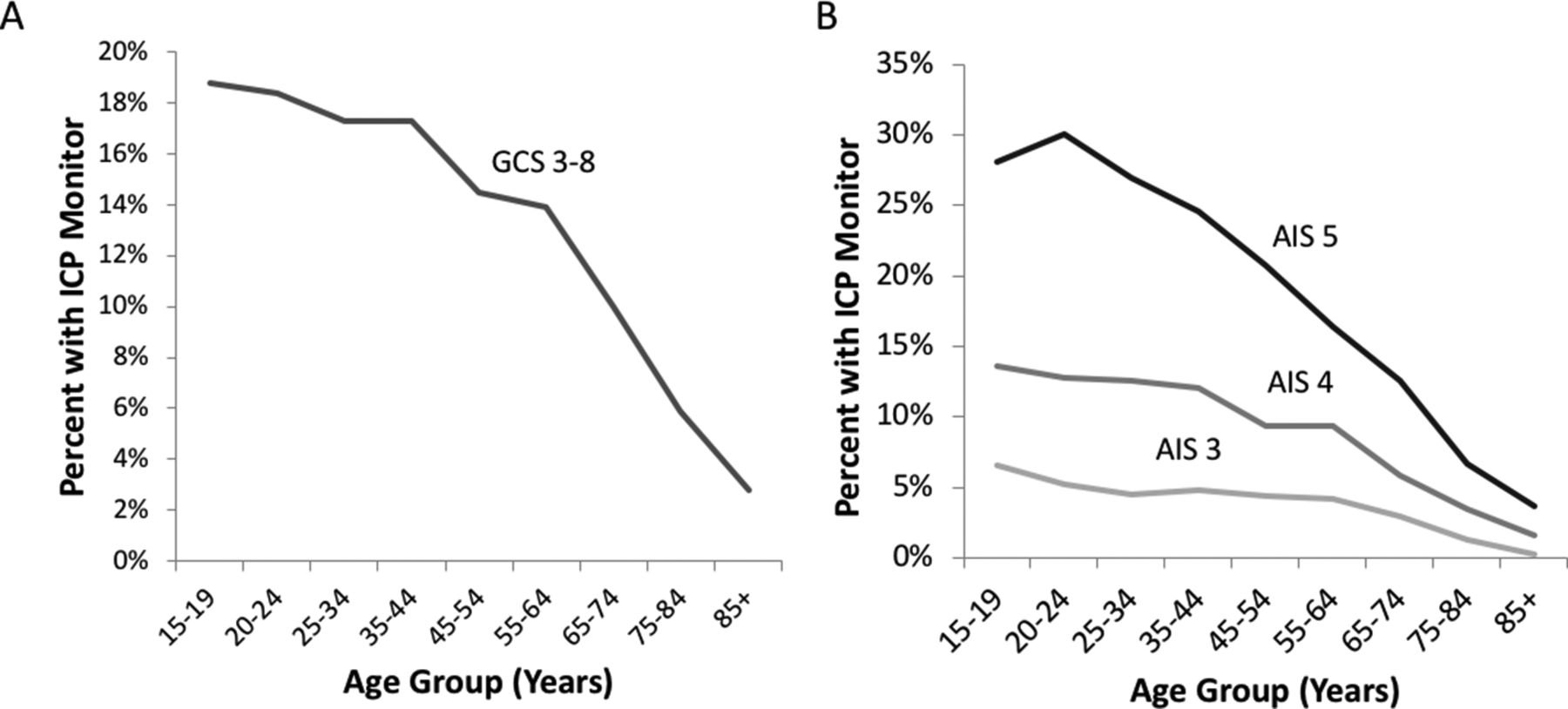
We evaluated ICP monitor use stratified by age and TBI severity. For patients with admission GCS scores of 3–8, ICP monitor placement decreased with increasing patient age (figure 2A). For example, 17% of patients aged 45–54 with admission GCS scores of 3–8 had an ICP monitor placed as compared with 10% of patients aged 65–74, and only 6% of patients aged 75–84. We also examined ICP monitor placement rates stratified by age group and AIS-Head scores (figure 2B), finding decreased rates of ICP monitor placement with increasing age for all AIS-Head groups (each p<0.001). The decrease in monitor placement rates by age was most significant for patients with AIS scores of 4 and 5. Next, we performed multivariable analysis to identify predictors for ICP monitor placement (table 4). Patients aged 65 and over were significantly less likely to have a monitor placed than those <65 years of age (adjusted OR 0.41, 95% CI 0.36 to 0.46). Male patients were also more likely to have an ICP monitor placed (adjusted OR 1.10, 95% CI 1.02 to 1.19). Additional predictors of ICP monitor placement included private insurance and treatment at an institution staffed by three or more neurosurgeons (table 4).
Multivariable analysis for predictors of ICP monitor placement (NTDB 2010–2014)

{kind=link}
{kind=link}
Percentage of patients who received an ICP monitor, stratified by (A) GCS and (B) AIS-Head scores. AIS, Abbreviated Injury Scale; GCS, Glasgow Coma Scale; ICP, intracranial pressure.
Discussion
For acute management of TBI, providers rely on literature including the BTF guidelines to support their clinical decision-making. In the 2016 fourth edition of the Guidelines for the Management of Severe Traumatic Brain Injury, the BTF provides a Level IIB recommendation for ICP monitoring in patients with severe TBI to reduce in-hospital and 2-week mortality.6 The previous (third) edition guidelines discussed the recommendation of ICP monitoring for severe TBI (GCS scores of 3–8) with either an abnormal CT scan, or two or more of the following: ‘age over 40 years, unilateral or bilateral motor posturing, or systolic blood pressure (BP) <90 mm Hg.’8Since the third edition was published, there have not been any new studies providing further guidance on which patients should receive ICP monitoring.6 In our study, we demonstrated that despite the universal inclusion of all patients with severe TBI, there is in fact an age disparity in ICP monitor placement.
Studies attempting to show a benefit after ICP monitor placement have produced mixed results. Recent studies by MacLaughlin et al and Agrawal et al have shown significant survival benefit in patients who meet BTF guideline criteria and receive an ICP monitor.9 10 Unfortunately, several additional articles assessing patients who met BTF ICP monitor placement guidelines found higher mortality rates in patients who received an ICP monitor.4 11 12 A recent meta-analysis by Shen et al of 18 studies including over 25 000 patients with severe TBI concluded that ICP monitoring significantly reduced overall mortality, hospital mortality, and 2-week and 6-month mortality rates.13 However, another recent meta-analysis of patients with TBI showed that ICP monitors improve prognosis, but do not affect hospital mortality rates.14 This wide range of outcomes has led to the weak level of evidence regarding monitor use in recent guidelines, though the recommendation for monitor use remains. This knowledge deficit is particularly acute in trauma subpopulations, such as elderly patients, and leaves many questions unanswered. Elderly patients who suffer from a TBI have a 1-year mortality or morbidity rate of over 80%; it is unclear if this could be improved by avoiding the discrepancy in monitor use that we identify.15 Recent studies focusing on specific age demographics again had mixed results, however. These include an observational study showing improved hospital and 6-month mortality with ICP monitor placement in the elderly,7 as compared with a 2007–2008 NTDB study that did not find a survival benefit in patients over 55 years.5
ICP monitor placement is a safe procedure with a low-risk profile. ICP monitors are associated with some complications, including cerebrospinal fluid leak and infection, with reported rates between 0% and 5%.16–18 Placement may be performed by a wide array of specialists, with studies showing excellent outcomes with placement by trauma surgeons, neurosurgeons, general surgeons and mid-level practitioners.16–18 It is unclear whether the risks of monitor placement or the risk-to-benefit ratio changes with age.
The strength of this study lies on its sampling population. Using the NTDB, we analyzed close to half a million trauma patients across the country during a 5-year period. Our sample comes from the largest national trauma registry, providing the best possible representation of trauma patients in the USA. A potential limitation to this study is the reliance on GCS as a marker of TBI. Previous studies have questioned the utility of GCS in classifying degrees of central nervous system injury, and a study by Salottolo et al showed that GCS can be significantly affected by age, as older patients tend to have higher GCS scores for the same severity of TBI than younger patients.19 Although we used both AIS-Head and GCS as measures for brain injury severity, this potential variance does question the validity of using admission GCS scores of 3–8 as an inclusion criterion in the study as well as in the BTF guidelines. Substance abuse, in particular alcohol use, has also been shown to reduce GCS, and could potentially serve as a confounder in TBI severity.20 However, rates of alcohol and substance abuse were the same in both ICP and non-ICP monitoring groups, with no statistically significant differences (table 2). To remain in accordance with current BTF guidelines, we used GCS as a primary marker of TBI severity, despite potential issues with this selection criterion. Although this study provides ample data from the hospital admission after the inciting incident, there are insufficient data regarding long-term follow-up or functional status. This allows us to only report the immediate effects of ICP monitoring, but we are unable to comment on the long-term outcomes of this type of management.
Conclusion
Patients ≥65 years of age with severe blunt TBI are less likely to be treated with an ICP monitor when compared with younger patients. Age disparities in adherence to BTF guidelines may result in worse outcomes for patients with severe TBI.
References
Footnotes
Contributors All authors contributed to the study design, data analysis, and article preparation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The UC San Diego Institutional Review Board reviewed and approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open-access repository.