Article Text

Abstract
It is often that the acute care surgeon will be called on to evaluate the pregnant patient with abdominal pain. Most of the diagnostic and management decisions regarding pregnant patients will follow the usual tenets of surgery; however, there are important differences in the pregnant patient to be aware of to avoid pitfalls which can lead to complications for both mother and fetus. This review hopes to describe the most common emergencies facing the surgeon caring for the pregnant patient and the latest management options.
- pregnancy
- emergency general surgery
- pregnant
- emergency surgery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
There are more than 8000 urgent non-obstetrical surgical procedures performed each year, impacting up to 2% of all pregnancies.1 The evaluation of the pregnant patient must weigh the risks and benefits of diagnostic methodology and therapy on the mother, and the fetus as well. Complicating care is the fact that the normal physiologic and anatomic changes that occur in pregnancy may make it difficult to interpret signs usually used in early diagnosis of emergency conditions. The delay in diagnosis and treatment of the surgical abdomen in the pregnant patient because of fear of unnecessary procedures and tests contributes to the high complication rate in this patient population. Attention to detail, heightened suspicion, serial physical examination, clinical awareness and systematic evaluation can help avert unnecessary maternal complications and fetal loss from emergency surgical conditions. This review will highlight the more common causes of the acute abdomen in pregnancy with suggested treatment options. Appropriate diagnostic tests or procedures should never be avoided or delayed simply because of pregnancy; never penalize a patient for being pregnant.
Normal physiologic and anatomic changes in pregnancy
The physiologic changes that comprise maternal adaptation to pregnancy involve almost every organ system. The plasma volume in pregnancy increases by almost 50%, whereas the red cell mass increases by only 20%, resulting in the ‘physiologic anemia of pregnancy’. It is not uncommon to see a baseline hematocrit of 31%–33%.2 The increased plasma volume allows the pregnant patient to withstand a significant amount of blood loss before any overt manifestations of shock appear. Cardiac output increases beginning in the second trimester. Uterine blood flow also increases as the fetus grows, comprising 20% of cardiac output by term. This system is highly regulated and extremely sensitive to external agents such as catecholamine and maternal intravascular volume loss. Maternal hemorrhage can be compensated by decreased uterine flow. Maternal hypovolemia may be marked by fetal distress before any evidence of maternal tachycardia or hypotension is present.
Oxygen consumption and resting ventilation increase in pregnancy as a result of an increase in tidal volume caused by rising progesterone levels. This results in a respiratory alkalosis with a pCO2 of approximately 30 mm Hg and a metabolic compensation with bicarbonate levels in the 19–20 mEq/L range.3 Gastrointestinal motility is decreased, and in addition to the reduction in resting lower esophageal pressure, pregnant patients are more likely to experience gastroesophageal reflux and have an increased risk of aspiration with general anesthesia.
Hematologically, in addition to the decrease in hemoglobin levels seen from the physiologic anemia, there is a relative leukocytosis. Typically, the white cell count will range from 12 000/mm3 to 15 000/mm3 and can reach as high as 25 000/mm3, often complicating the diagnosis of infection.3 The state of relative hypercoagulability in pregnant patients is well known to increase the risk for thromboembolic complications.4
Anatomically, the uterus becomes an intra-abdominal organ at approximately 12 weeks of gestation. At 20 weeks the uterus can be palpated at the umbilicus, and by 36 weeks the uterus reaches the costal margin. The growing uterus can complicate invasive procedures such as port placement in laparoscopic surgery. As the uterus enlarges, maternal organs are displaced upwards; in the late stages of pregnancy the majority of the gastrointestinal tract may be found above the inferior costal margins. The diaphragm may also be elevated by as much as 4 cm. Finally, as the pregnancy progresses, uterine compression of the vena cava decreases venous return, resulting in a 30% drop in cardiac output. This ‘supine hypotensive syndrome’ can be alleviated by displacing the uterus from the vena cava by positioning the patient in the left lateral decubitus position or at least placing pillows under the patient’s right side to elevate it slightly.4
Pregnancy is associated with reduced ureteral tone and peristalsis, which can lead to a dilated ureter and hydronephrosis. This is due in part to mechanical compression on the ureters as the uterus enlarges, with the rate of right-sided hydronephrosis significantly higher than the left side.5 These changes can lead to infection or urolithiasis.6
Radiological issues in the pregnant patient
The key concern regarding imaging during pregnancy is the effect of ionizing radiation on the growing fetus. The risks of radiation include fetal death, growth retardation, microcephaly, malformations, mental retardation and childhood cancers.7 Knowledge of the effects of radiation on fetal development has been extrapolated from animal studies and observations of exposed human populations, particularly those of Hiroshima and Nagasaki.8 9 While the American College of Obstetricians and Gynecologists states that exposure of <5 rads has not been associated with an increase in fetal anomalies or pregnancy loss,10 clinically, the fetal dose of concern for teratogenesis is probably in the range of 10–20 rads.11 When deciding on the appropriate workup for any pregnant patient, always remember the principle that a ‘pregnant patient should not be penalized for being pregnant’.
A typical ‘PanScan’ (CT imaging of the head, cervical spine, chest, abdomen and pelvis) usually delivers <5 rads. An abdominal CT scan can be performed to evaluate abdominal pathology with only 0.3 rads.7 Ultrasound is useful in identifying appendicitis, cholecystitis and free fluid after abdominal trauma, and poses no known risk to the growing fetus. MRI is emerging as a useful test to evaluate the abdomen in pregnant patients.12 13
Radiation exposure during endoscopic retrograde cholangiopancreatography (ERCP) can be reduced to a level significantly below 5 rads. In several series that measured the amount of radiation exposure during ERCP, pregnant patients were exposed to anywhere from 0.04 to 0.18 rads, without any short-term complications to the pregnancy and newborns.14 15 There has been noted to be a clear correlation between the lengths of fluoroscopy time with radiation exposure. Precautions such as using lead shielding (placed underneath the pregnant patient), maximizing distance between the patient and the X-ray source, and decreasing fluoroscopy times are recommended to minimize exposure.16 The technique of ERCP without using any radiation for pregnant patients has been described.17Magnetic resonance cholangiopancreatography (MRCP), choledochoscopy and endoscopic ultrasound have all been used to confirm clearance of the biliary system without the use of radiation following ERCP.18
Laparoscopy in pregnancy
Laparoscopy has emerged as a diagnostic and therapeutic tool in the care of the pregnant patient with abdominal pain.19 Laparoscopy is well tolerated by both mother and fetus with minimal adverse effects in all trimesters.20 21 Although a 2012 meta-analysis of 11 studies found low-grade evidence that laparoscopic compared with open appendectomy was associated with a higher rate of fetal loss,22 a more recent Nationwide Inpatient Sample study of 20 000 patients found a three times higher risk of an adverse obstetrical outcome associated with open surgery.23 Our preference is to favor the laparoscopic approach as long as it appears safe for trochar insertion depending on the body habitus and degree of pregnancy. Open trochar placement (Hasson technique) or insertion of the Veress needle into an alternate site (Palmer’s point) is recommended to avoid injury to the uterus during entry.24 25 Palmer’s point is described in the left upper quadrant, 3 cm below the costal margin in the midclavicular line.26 In the late second trimester and beyond, laparoscopy becomes technically difficult and an open incision (vertical or over the point of maximal tenderness) can be used. The surgeon should avoid manipulation of the uterus during the procedure. Immediate preoperative and postoperative fetal monitoring should be used in all viable pregnancies of 24 weeks and older.27 28
Acute abdomen in the pregnant patient
Approximately 1 in 635 women require non-obstetrical abdominal surgery during pregnancy.29 Making the diagnosis is often problematic for the following reasons: the expanding uterus, which displaces other intra-abdominal organs and thus makes physical exam difficult30; the high prevalence of nausea, vomiting and abdominal pain routinely encountered in the normal obstetric patient31 and the general reluctance to operate unnecessarily on a gravid patient.1 Acute appendicitis and cholecystitis are the most common non-obstetrical emergencies requiring surgery during pregnancy.24
Appendicitis
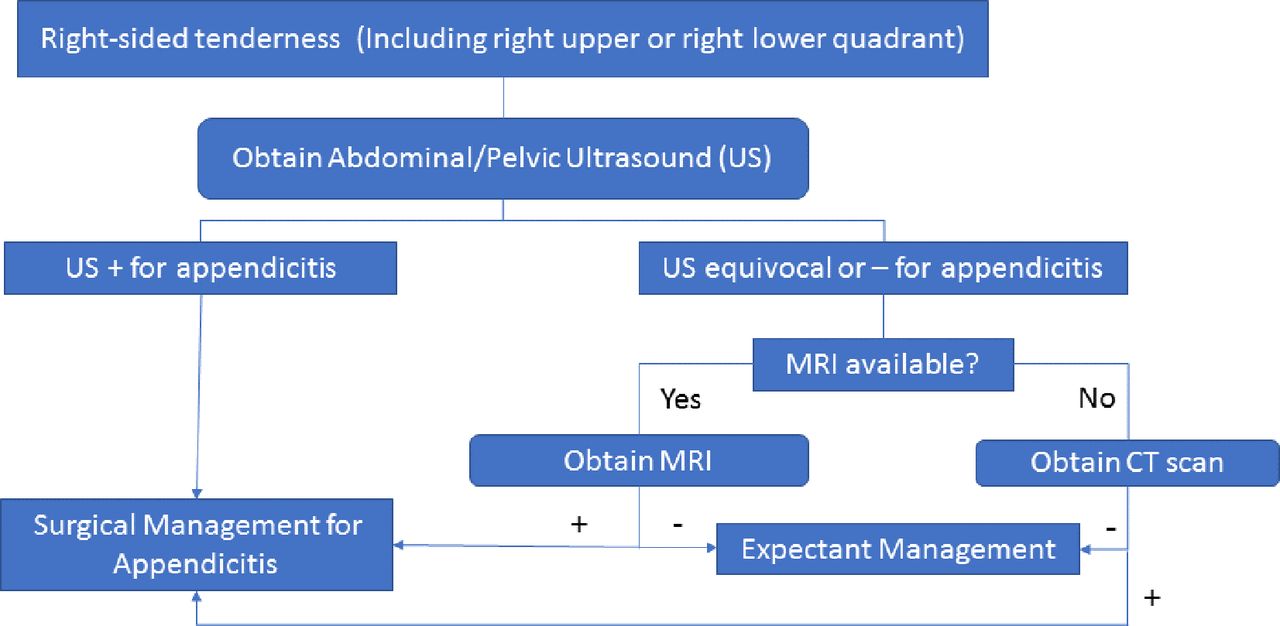
A case of acute appendicitis during pregnancy was first reported in the literature by Hancock in 1848.32 It is the most common non-obstetric surgical emergency during pregnancy.1 It occurs in about 1 in 1000–2000 pregnancies and may occur at any time during the pregnancy.33–35 The diagnosis is more frequently missed in pregnant than in non-pregnant patients, because signs and symptoms of appendicitis, such as leukocytosis, nausea and vomiting, are also commonly seen during pregnancy. There is a question of reliability of the abdominal examination in pregnant patients suspected of having appendicitis. The classical teaching is that the location of pain from appendicitis moves progressively upward as the pregnancy progresses based on Baer’s 1932 study of barium images of 78 pregnant patients.36 More recent retrospective studies have failed to corroborate this hypothesis showing roughly 90% of patients having pain in the right lower quadrant regardless of trimester.37 38 Maternal morbidity is usually the result of a delay in diagnosis. Fetal loss occurs in 3%–5% of pregnant patients without perforation but can be as high as 36% with perforation.35 This high risk of fetal loss with perforation along with the difficulty of diagnosing appendicitis in the pregnant patient explains the high rate (50% in many series) of normal appendices found at operation.39 Traditionally, this high rate of negative operation had not been found to increase maternal or fetal morbidity; however, recent data suggest that negative appendectomy may be associated with an increase in fetal loss.40 41 Therefore, it is important to confirm the diagnosis before heading to the operating room. Ultrasound, CT, MRI or diagnostic laparoscopy can confirm the diagnosis. Ultrasound should be the first-line study for abdominal pain in the pregnant female; however, the sensitivity ranges from only 20% to 36%. If ultrasound is indeterminate, the next study that should be ordered if available is an MRI. A review of imaging strategies for right lower quadrant pain in pregnant females performed a meta-analysis of six studies examining the role of MRI in diagnosing appendicitis in pregnant females. They found a pooled sensitivity of 0.91 and a specificity of 0.98.42 If MRI is unavailable, a CT may be ordered. While the diagnostic accuracy of CT for appendicitis in the non-obstetric population has been well demonstrated,43 there is a paucity of data for pregnant females. Two small studies looking specifically at pregnant patients demonstrated successful diagnoses of appendicitis in 5/7 patients and 12/13 patients.44 45 Protocols involving abdominal ultrasound followed by CT scan, if inconclusive, have been associated with a reduction of negative appendectomy rates.39 Our diagnostic algorithm for appendicitis is shown in figure 1. Appendectomy can be performed open or laparoscopically20 depending on the surgeon’s comfort level with the patient’s body habitus and degree of pregnancy. The laparoscopic approach has advanced to become the standard of care at many centers; this is the authors’ preference as well.

{kind=link}
This algorithm is our suggested diagnostic workup for a pregnant patient with a suspected diagnosis of appendicitis.
Gallbladder disease
Biliary tract disease is the second most common non-obstetric surgical problem.1 Weight gain and hormonal changes predispose pregnant women to biliary sludge and gallstone formation. Weakened contractions and decreased emptying lead to increased gallbladder volume during fasting and postprandially. Biliary stasis contributes to cholesterol crystal sequestration, theoretically leading to formation of sludge and stones. Estrogen increases bile lithogenicity, whereas progesterone impairs gallbladder emptying.46 Lower gallbladder ejection fractions and increasing parity appear to increase the risk of sludge formation.47 The reported incidence of biliary sludge formation is as high as 31%, while gallstone formation ranges from 3% to 12%.48 49 A total of 1 in 1000 pregnancies will develop symptoms related to biliary colic.50 51 About one-third of patients with biliary colic will experience no additional bouts during the following 2 years. Unfortunately, approximately 80% of pregnant women presenting with symptoms will have recurrence of symptoms with 20%–40% recurring prior to delivery.52 53 This recurrence is often more severe than the initial presentation. Surgical intervention is indicated for obstructive jaundice, acute cholecystitis and gallstone pancreatitis. Where once the non-operative management with delayed cholecystectomy of symptomatic cholelithiasis was encouraged,54–58 there are data now suggesting that pregnant patients with symptomatic cholelithiasis should undergo cholecystectomy early due to the increase in the rate of recurrent hospitalizations, preterm deliveries, spontaneous abortions and fetal morbidity associated with non-operative management.21 59 In addition, non-operative management of symptomatic cholelithiasis increases the risk of gallstone pancreatitis up to 15%.53 Whereas once it was thought that the second trimester was the optimal time for cholecystectomy due to decreased spontaneous abortions and preterm labor, there is a growing body of evidence that suggests laparoscopy can be performed in all trimesters with equal safety.20 21
Cholangitis
Choledocholithiasis in pregnancy is infrequent and is estimated to be around 1 in 1200 deliveries60; however, therapeutic intervention is almost always required.61 The diagnosis of choledocholithiasis is similar in both pregnant and non-pregnant patients; fever, leukocytosis, abdominal pain, hyperbilirubinemia and elevated alkaline phosphatase, with or without shock suggests the diagnosis of cholangitis.62 While Charcot’s original triad has been shown to be 95% specific for cholangitis, it is only 26% sensitive for the disease. The Tokyo guidelines for diagnosing cholangitis first published in 2007 and revised in 2012 have much higher sensitivities (83% and 92%, respectively).63 64 Intravenous resuscitation and broad-spectrum antibiotics should be started immediately on suspicion of the diagnosis. Ultrasonography can detect common bile duct stones but only at a 30% sensitivity.65 66 If there is uncertainty in the diagnosis, MRCP seems to be an excellent diagnostic modality in pregnancy.67 It is not associated with any known adverse fetal effects and can be used in all stages of pregnancy.68
Endoscopic treatment of choledocholithiasis is presently the treatment of choice in pregnant patients, especially in the presence of cholangitis. Therapeutic ERCP in pregnancy was first reported in 1990 by Baillie et al.69 Since then, there have been multiple studies that have demonstrated the safety and success of ERCP followed by sphincterotomy during pregnancy with minimal risk of radiation to the fetus.14 15 60 70–72 In cases where endoscopic retrieval of the choledocholithiasis is not possible, biliary stents may be placed; however, they do carry the risk of stent occlusion with subsequent cholangitis and also necessitate an additional procedure for stent removal.73–75
ERCP has been described using both conscious sedation and general anesthesia with equal safety.76–79 Maternal fetal monitoring should be used during the procedure under the supervision of the obstetrician. In the rare situation when ERCP is unavailable or unsuccessful, percutaneous transhepatic cholangiography with drainage can be used.80 81 Another alternative is surgical intervention. Laparoscopic common bile duct exploration has been described in the second trimester and early third trimester in case reports, but no large studies have been published to date.82–86 Open cholecystectomy with choledocotomy and T-tube placement has also been described in older series, although with associated higher rates of fetal loss.55 59 Whatever the method used to clear the duct, cholecystectomy is offered during the same hospitalization due to the high rate of recurrent symptoms associated with outpatient management.87
Acute pancreatitis
Acute pancreatitis complicates approximately 1 in 1000–5000 pregnancies, usually occurring late in the third trimester or in the early postpartum period.87–91 Cholelithiasis is the most common cause and accounts for 67%–100% of cases, followed by ethanol use and hyperlipidemia.91 92 The medical management is the same as in pancreatitis in non-pregnant women and consists of bowel rest, fluid and electrolyte resuscitation and the use of analgesics.93 These patients are best managed in an intensive care unit. As mentioned previously for choledocholithiasis, because of the high recurrence of gallstone-related symptoms, a prompt cholecystectomy should be performed when the patient improves during the same hospitalization if the determined etiology was biliary.87
Intestinal obstruction
Acute intestinal obstruction is the third most common non-obstetric abdominal emergency with an incidence of 1 in 1500 pregnancies.94 Adhesions cause 60%–70% of cases. Other causes include volvulus, intussusception, hernia, neoplasm and appendicitis. Of note, volvulus can be the cause of obstruction in up to 25% of cases of gestational obstruction, while in non-pregnant patients, it is only 5%.1 Gestational bowel obstruction should never be confused with hyperemesis gravidarum, which can lead to a delay in diagnosis, the former of which will have abdominal examination findings.6 The approach to intestinal obstruction is the same in pregnancy as in the general population. Medical management involving hydration, bowel rest and nasogastric decompression will lead to resolution in the majority of cases.1 Both laparoscopic as well as open approaches for surgery are acceptable.95 96 Mortality for gestational intestinal obstruction is higher than for non-pregnant patients and increases as gestational age increases.1 96 Excessive manipulation of the uterus should be avoided. Fetal monitoring should be used in all viable cases of 24 weeks and older.27 28
Conclusion
Pregnant patients are a specific population, where worry about the risk of harm to the fetus often overshadows clinical decision making when presented with a possible surgical diagnosis. While it is important to limit duration of exposure to radiation and unnecessary surgery in this population, delays in diagnosis and treatment can also harm both fetus and mother. Obtaining the correct diagnosis in the pregnant patient can be challenging because of the normal physiologic and anatomic changes that occur with pregnancy. While reduced radiation imaging such as MRI or radiation-free ERCP may allow limiting of radiation exposure to the fetus, availability and time involved may hinder use depending on one’s practice setting. Minimally invasive surgery may be performed safely depending on the surgeon’s comfort level with the duration of pregnancy. In cases of general surgical emergencies during pregnancy, a diagnosis should be rapidly sought and treatment offered, lest we should ever penalize a patient for being pregnant.
Acknowledgments
The authors would like to acknowledge Katherine Armstrong for her assistance with reviewing the manuscript.
References
Footnotes
Contributors JJS and AS wrote and reviewed the manuscript.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.