Article Text

Abstract
Background Effective triage of injured patients is often a balancing act for trauma systems. As healthcare reimbursements continue to decline,1 innovative programs to effectively use hospital resources are essential in maintaining a viable trauma system. The objective of this pilot intervention was to evaluate a new triage model using ‘trauma resource’ (TR) as a new category in our existing Tiered Trauma Team Activation (TA) approach with hopes of decreasing charges without adversely affecting patient outcome.
Methods Patients at one Level II Trauma Center (TC) over seven months were studied. Patients not meeting American College of Surgeons criteria for TA were assigned as TR and transported to a designated TC for expedited emergency department (ED) evaluation. Such patients were immediately assessed by a trauma nurse, ED nurse, and board-certified ED physician. Diagnostic studies were ordered, and the trauma surgeon (TS) was consulted as needed. Demographics, injury mechanism, time to physician evaluation, time to CT scan, time to disposition, hospital length of stay (LOS), and in-hospital mortality were analyzed.
Results Fifty-two of the 318 TR patients were admitted by the TS and were similar to TA patients (N=684) with regard to gender, mean Injury Severity Score, mean LOS and in-hospital mortality, but were older (60.4 vs 47.2 years, p<0.0001) and often involved in a fall injury (52% vs 35%, p=0.0170). TR patients had increased door to physician evaluation times (11.5 vs 0.4 minutes, p<0.0001) and increased door to CT times (76.2 vs 25.9 minutes, p<0.0001). Of the 313 TR patients, 52 incurred charges totaling US$253 708 compared with US$1 041 612 if patients had been classified as TA.
Conclusions Designating patients as TR prehospital with expedited evaluation by an ED physician and early TS consultation resulted in reduced use of resources and lower hospital charges without increase in LOS, time to disposition or in-hospital mortality.
Level of evidence Level II
- triage
- cost-effective management
- ED management
- resource
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Regionalized trauma centers deliver rapid resuscitation, stabilization, and treatment with improved clinical outcomes.2–4 Development, implementation, and evaluation of trauma systems and related protocols have been ongoing in order to assess the safety, effectiveness, and efficiency of patient-centered trauma care.5 6 Incorporation of criteria into trauma center triage standards is necessary to identify high-risk patients who may need urgent operating room use and intensive care unit (ICU) admission.7 Current literature support that a combination of physiologic and anatomic parameters, along with selected mechanism of injuries, comorbidities, and extremes of age may provide the best prehospital and in-hospital triage performance.8
From 1994 to 2014, emergency department (ED) visits have increased from 90.5 million to over 136 million9 with 37 million injury-related ED visits in the USA in 2014.10 Transporting injured patients to the most appropriate medical facility impacts injury-related morbidity and mortality as well as cost of care. Improvements in trauma triage to get the ‘right patient’ to the ‘right hospital’ is a balancing act between overtriage (transporting patients with minor injuries to major trauma centers) and undertriage (transporting seriously injured patients to non-trauma centers) for trauma systems. The goal of a trauma triage system is to maximize sensitivity to prevent undertriage while maximizing specificity to minimize overtriage.11 The American College of Surgeons (ACS) first designed the Field Categorization of Trauma Patients in 1986 based mainly on expert opinion.12 Between 1986 and 1999, the ACS Decision Scheme was revised three times (1990, 1993, and 1999).13–15 With each revision, the scheme was re-evaluated by the ACS-Committee on Trauma (COT) and analyzed in the context of available literature and expert opinion. In 2005, the Centers for Disease Control and Prevention (CDC) in collaboration with the ACS-COT and the National Highway Traffic Safety Administration facilitated revision of these guidelines by the National Expert Panel (the Panel) which included injury care providers, public health professionals, automotive industry representatives, and officials from federal agencies.16 Faul and colleagues reviewed the National Trauma Databank and found a 12% reduction in overtriage using the 2006 compared with the 1999 field triage guidelines.17 The CDC reconvened the Panel in 2011 and the guidelines were further modified.18 Field triage guidelines established by the ACS-COT are based on a 5% undertriage rate and 30% to 50% overtriage rate.19 However, such a high overtriage rate may not be sustainable due to the high cost of trauma team activation.20 Although full trauma team activation has been shown to lower ED length of stay (LOS) and in-hospital mortality in injured geriatric patients, high-level trauma activation is a burden on human and physical resource use, along with hospital charges, especially in less severely injured patients.20 21 The challenge of prehospital triage is further confounded by the use of anticoagulants and antiplatelet agents in trauma patients, as well as the increasing elderly population.22
Trauma ranks as the second most expensive condition in terms of healthcare spending in the USA, exceeded only by heart disease.23 As healthcare reimbursements continue to decline,1 innovative programs to effectively use hospital resources are essential for the viability of trauma centers in the future. One key problem is that serious injury is not always known before ED arrival. Current field triage guidelines19 are based on the risk of being seriously injured. Baxt et al suggest that a more cost-effective triage approach for a trauma center is to identify major resuscitations and then subject all other triaged patients to a more limited and cost-effective evaluation.24 Further studies that evaluate two-tiered trauma response systems have demonstrated improved accuracy of predicting immediate treatment need and safety of major trauma patients; thus, allowing more efficient use of trauma personnel.25–28 An analysis of adjusted cost of acute care injury (prehospital Emergency Medical Services (EMS), ED, and hospital admission costs) by hospital type and injury severity in patients transported by EMS to acute care hospitals demonstrated the highest cost in major trauma centers, even among patients with minor injuries.29 A significant portion of acute care costs were attributed to transporting low-risk patients to high-resource hospitals. Strict adherence to field triage guidelines was recommended including the transport of low-risk patients to non-trauma centers. In addition to cost, overtriage may result in crowding of the ED that may adversely impact trauma center functioning. This further supports the refinement of triage guidelines that decrease overtriage and undertriage.
We developed a prototype model system to evaluate a process to decrease overtriage in our trauma system without adversely affecting patient outcome. We implemented this new prehospital triage model as a pilot study that allows for the designation of a subgroup of trauma patients as ‘trauma resource’ (TR). We hypothesize that this new TR group will use significantly less resources without an increase in hospital charges, length of hospital stay, or in-hospital mortality.
Methods
All trauma patients evaluated at one ACS certified Level II Trauma Center from July 2013 through January 2014 were included in this study. Patients meeting strict ACS trauma criteria were designated trauma activations (TAs) by prehospital and base station personnel (see box 1).
Major and minor trauma team activation criteria
Major trauma activation criteria
GCS<13
SBP<90
Respiratory rate <10 or >29
Flail chest
Intubated patients transferred from the scene
Respiratory compromising or in need of emergent airway
Possible airway compromise
Two or more proximal long bone fractures
All penetrating injuries to the head, neck, torso or extremities proximal to the elbow/knee
Combative
Transfer patients receiving blood to maintain vital signs
Minor trauma activation criteria
Ejection from/off a vehicle
Vehicle rollover with unrestrained patient
Death in the same passenger compartment
Auto versus bicyclist/pedestrian thrown, run over, or with significant >20 mph impact
Fall >3 times the patient’s height or >15 feet
Exposure to blast or explosion
Motorcycle crash >20 mph: ED, MD, or MICN judgment
Amputations proximal to wrist/ankle
Suspected pelvic fractures
Limb paralysis
Crush injury, degloved or mangled extremity
Neurologic or vascular deficit or extremities
Combination of trauma with burns
Child abuse: known or suspected with significant injury
Patients not meeting ACS trauma criteria for trauma activation, but were felt to require the resources of a trauma center, were candidates for ‘TR’ designation. These patients were designated based on field information (see box 2) given to the registered nurse at the hospital base station.
Trauma resource guidelines
Trauma resource guidelines
Age <5 or >55 years
Pregnancy >20 weeks
Bleeding disorders
Anticoagulant or antiplatelet agent use (ie, Warfarin or Clopidogrel, novel oral anticoagulants) exception: aspirin
Loss of consciousness reported
Severe cardiac and/or respiratory disease
EMS provider judgment
End-stage renal disease requiring dialysis
Extrication time > 20 minutes
Intrusion into occupied passenger space >12 inch frontal
Intrusion into occupied passenger space >8 inch side
Any equivocal patients were discussed with the ED physician and then were designated as either TA, TR or ED patients.
All TR patients underwent expedited evaluation by a board-certified ED physician, dedicated Trauma Nursing Core Course (TNCC) certified trauma nurse and TNCC certified ED nurse, with early involvement by the trauma surgeon (TS) as needed (see table 1). Additionally, the CT technician, respiratory therapist and laboratory technician were notified on patient’s arrival to the ED, and CT scans for TR patients were prioritized. Demographics data, mechanism of injury, time to physician evaluation (MD evaluation), time to CT scan, time to disposition (ie, to Interventional Radiology, operating room, ICU, step-down unit, floor bed or discharge from facility), hospital length of stay (LOS), Injury Severity Score (ISS), and in-hospital mortality were collected and analyzed.
Resource utilization by level of trauma activation
Undertriaged patients were those who did not meet trauma field triage criteria but were later determined to meet such criteria for a higher level of trauma care. Overtriaged patients were those who met trauma field triage criteria but later were determined to have minor injuries not requiring higher level of trauma care. ED activation charges were used as a surrogate for cost. Information on hospital personnel activated and charges for each trauma triage level were derived from established hospital charge levels and are noted in table 1.
Continuous variables such as age were compared between groups using an unpaired t-test. Categorical variables were compared using Fisher’s χ2 test of independence using Yates correction for continuity for small numbers. Differences in proportions were evaluated using the z test of equality of two proportions for one sided hypotheses. For two-sided hypotheses, the χ2 test of independence was applied. We chose p<0.05 as statistically significant.
Analyses included comparisons between the TA versus TR groups. For evaluation of hospital charges only, a subgroup of TR patients who were admitted to the trauma service were reviewed to analyze the difference in charges if this pilot TR process had not been in place and those same patients had incurred TA ED fees.
Results
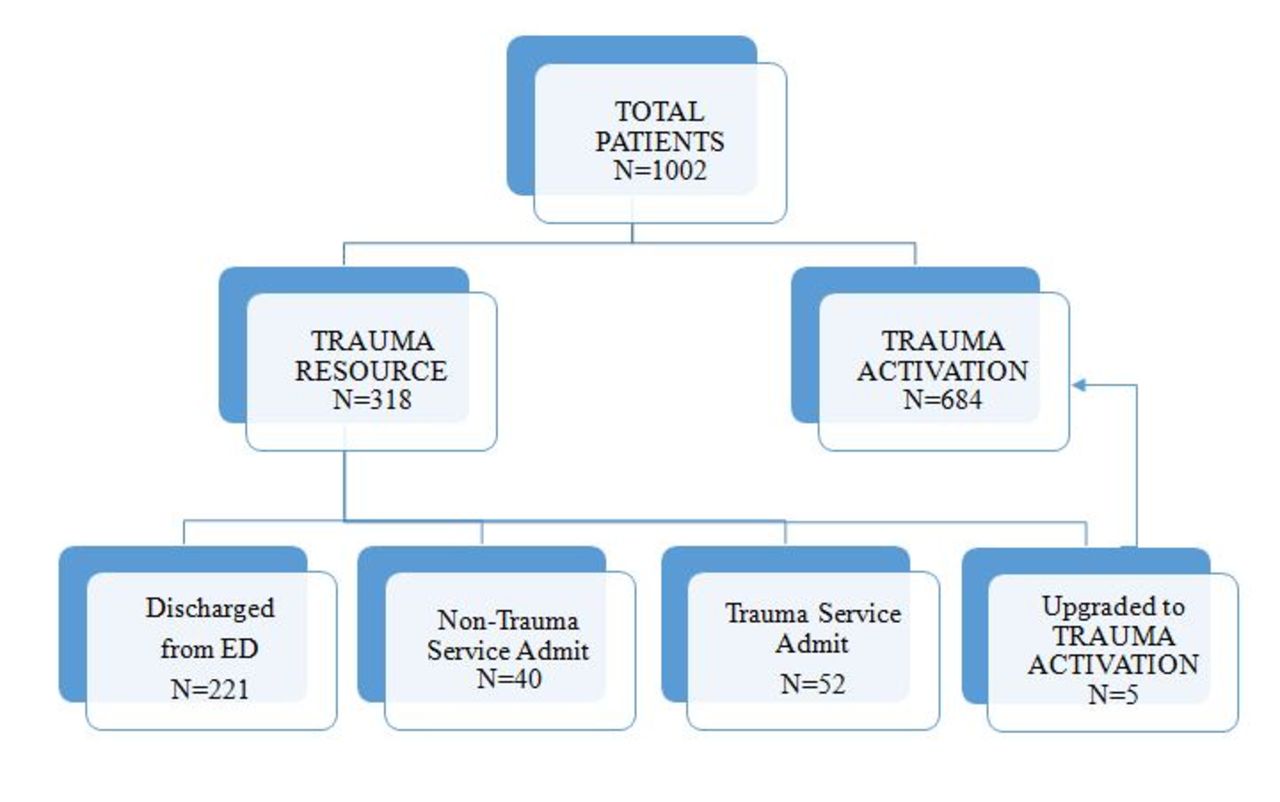
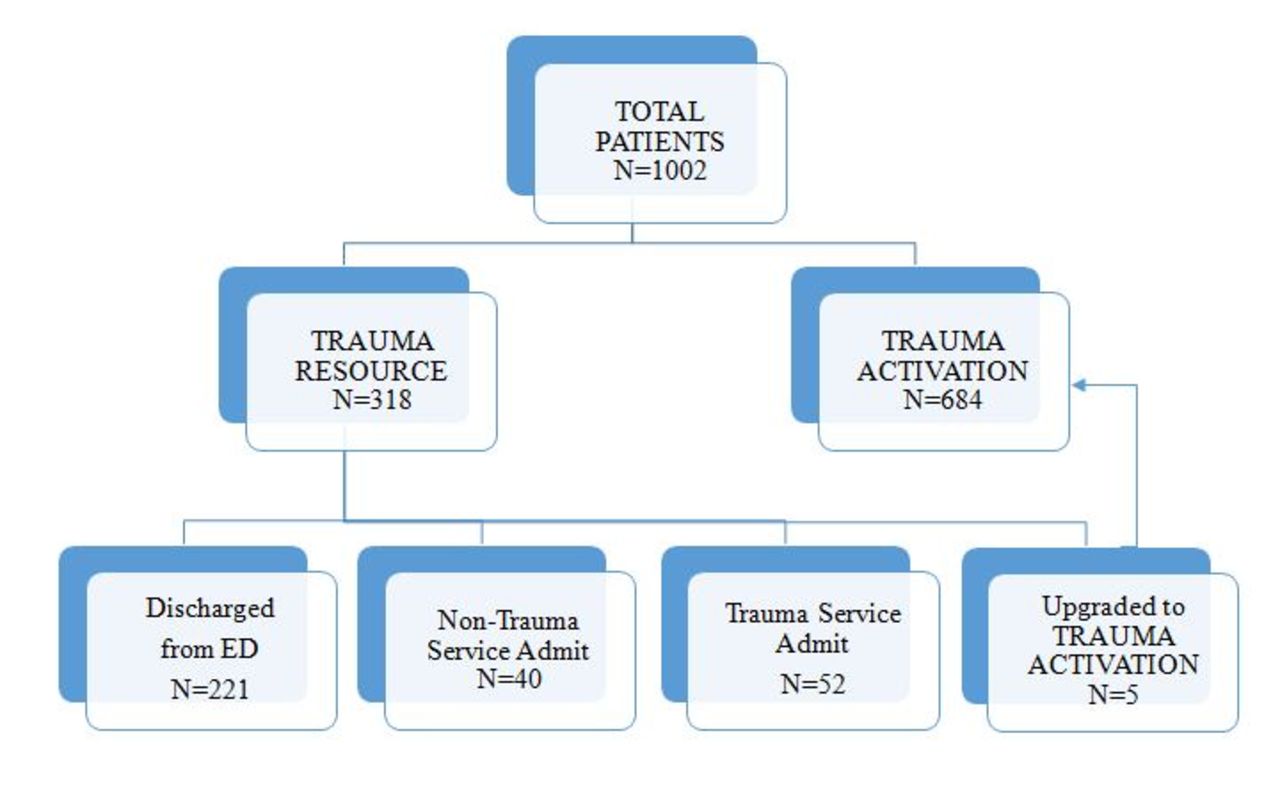
There were 684 patients in the TA group and 318 patients in the TR group evaluated during the study period (see figure 1). Five patients in the TR group (1.6%) were immediately upgraded to TA status by the ED physician. Two hundred and twenty-one (69.5%) patients in the TR group were discharged from the ED and 92 patients in the TR group were admitted to the hospital. Fifty-two (16.4%) patients in the TR group required TS consultation with trauma service admission. These 52 TR patients were similar to the TA patients with regard to gender, mean ISS, LOS, and in-hospital mortality (see table 2).
Data for trauma patients by triage group
{kind=link}
Distribution of patients.
The patients in the TR group that were admitted by the TS (n=52) were significantly different from the TA patients with regard to age (60.4 vs 47.2 years, p<0.0001), falls as mechanism of injury (52% vs 35%, p=0.0166), increased door to MD evaluation times (11.5 vs 0.4 minutes, p<0.0001), increased door to CT times (76.2 vs 25.9 minutes, p<0.0001), and decreased time to disposition (79 vs 132 minutes, p<0.0001).
TR patients (n=52) admitted by the TS were similar to trauma consult patients (n=187) from the ED with regard to age, gender, fall mechanism, ISS, LOS, in-hospital mortality and time to disposition compared with trauma consults from the ED. TR patients upgraded to TA status by the ED physician had similar times to CT compared with patients initially triaged as a TA.
Personnel resource use was significantly less in the TR group compared with the TA group (see table 1). Of the 313 patients in the TR group, 52 patients were upgraded to the trauma service and incurred ED charges totaling US$253 708 compared with US$1 041 612, if these patients had not received the TR assessment, but triaged as minor TAs. If all 313 TR patients were classified minor TAs, there would have had a 26% overtriage rate. With the TR designation, 1.6% (5/318) were undertriaged, but were immediately upgraded to TA status without increase in hospital LOS or in-hospital mortality. There were no ED deaths. The one death in the TR group was a non-agenarian who was designated comfort care the day following admission and then expired.
Discussion
Triage is a key to identifying patients with severe injuries who will benefit from the resources available at designated ACS Trauma Centers.18 By adding a TR category to our trauma triage system, we were able to significantly decrease overtriage. Only 18% of the patients designated as TR group required TS consultation and trauma admission. The TR group of patients used fewer hospital resources with no increase in in-hospital mortality. Prompt evaluation by a board certified ED physician was key, with only five patients (1.6%) requiring immediate upgrade to TA status. With our established triage process protocol, these five patients had similar door to MD evaluation times and door to CT scan times as compared with TA patient times.
CT scans were expedited for the TR group, but time from arrival to CT was still longer for the TR group as compared with TA group. However, no deleterious effect was noted from delayed CT scanning. CT scan delay in the TR group may in part be due to our institution’s CT scanning triage protocol, where priority is given to the TA patients, stroke code patients, and ED patients with acute neurological deterioration. TR patients upgraded to TA status demonstrated no change in time to CT when compared with TA patients. The time to disposition from the trauma room/ED (ie, to Interventional Radiology, operating room, ICU, step-down unit, in-patient hospital bed) was less in the TR group than in the TA group. This may be a result of the bed flow process in our ED and trauma room.
The TR group admitted to the trauma service had a similar ISS to the TA group. Intuitively, patients that do not meet TA criteria are at low risk for sustaining significant traumatic injuries. Hence, you would expect the TR group to have a lower ISS than the TA group. However, the TR group was significantly older in comparison and ground level falls was the most common mechanism of injury. Low energy trauma mechanism, such as falls from standing, can deceivingly cause more significant injuries in the elderly population30 which often leads to undertriage in the field.31Undertriage of these patients to non-trauma center or low-performing trauma centers can lead to increased mortality when compared with high performing trauma centers.32 Other researchers have reported a 15% to 50% undertriage rate in those over 64 years of age.33 Additionally, Nakamura and colleagues stated that undertriage increases with age and specifically found that those aged 45–54 years were associated with undertriage.34 Clearly, older people with low energy mechanism of injury do not meet the current national trauma field triage criteria19 as being at high risk for significant injury. However, if we designate TAs for all middle-aged and elderly patients who sustain a ground level fall, it may strain the trauma system. Predictive factors for undertriage in the elderly needs to be studied more closely.35 This will be an ongoing problem as the elderly population continues to increase in USA.30 Our study demonstrates one way to manage the undertriage problem in elderly patients, as well as patients on anticoagulants with minor trauma mechanisms.
Our data demonstrated no difference in the TR group compared with the TA group with regard to hospital LOS and in-hospital mortality. As measured by ED hospital charges and the number of hospital personnel required, physical resource and charges were significantly less in the TR group compared with the TA group.
The current study has several limitations. This was a 7-month pilot program with relatively small number of patients and was implemented in only one of the six designated trauma centers in our county. Additionally, we used patient charges as a surrogate for hospital resources used which may not directly translate to cost. Finally, our overtriage rate was an underestimate, since we did not delineate the number of TA patients who were discharged from the ED or within 24 hours of evaluation.
Further refinements of our triage categories should include a more efficient process to decrease times to CT scanning. A larger study including all six trauma centers in our county following our guidelines might confirm whether this program can be safely and effectively implemented in a regional trauma system. This model may create savings for the entire county if it is uniformly applied. Additionally, future analysis of hospital resource utilization and trauma staffing as it relates to patient volume and acuity may lead to more efficient trauma care.36
Conclusions
Designating patients as TR patients prehospital with expedited evaluation by a board certified ED physician with early TS consultation resulted the utilization of fewer resources and lower hospital charges without increasing hospital LOS or in-hospital mortality. TR is now part of the standard of care in our trauma triage process. Modifications to this piloted TR triage algorithm are currently being developed to further improve our triage process.
Supplementary Material
Acknowledgments
The authors thank Marc Sedwitz, J Gary Schwendig, and Christine Wells for their help in implementing this study. We also acknowledge Jiayan Wang for her assistance with manuscript preparation.
References
Footnotes
Contributors GTT and ISD were responsible for study design, analysis and interpretation. KBS and FN were responsible for data management and acquisition, analysis and interpretation. MGRN was responsible for study design and data interpretation. JFK was responsible for data analysis and interpretation. All authors were involved in the drafting and critical revision of the manuscript and provided final approval of the version to be published.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.