Article Text

Abstract
The following case report and literature review will detail the management of a traumatic amputation of the arm in a 12-year-old boy. Compared with lower limbs, upper limb prosthesis usually results in significant suboptimal function by any measure. While the literature lacks high-quality evidence with regard to functional outcomes following proximal amputations of the upper limb, especially in children, it is known that children generally have superior functional outcomes compared with their adult counterparts. The mechanism of injury, transportation of the amputated part, type of ischemia, timing of surgery, surgical techniques/factors and postoperative rehabilitation will be discussed as factors affecting outcome of reimplantation.
Level of evidence: V
- pediatric trauma
- reimplantation
- arm injuries
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Reimplantation is defined as the reattachment of a completely severed body part. It is considered one of the most difficult operations, particularly in upper limb surgery. Clinical experience, appropriate microsurgical equipment and a well-trained multidisciplinary team are all essential for optimal outcome. The aim of reimplantation is to retain a reattached part which gives a superior functional outcome compared with prosthesis.
The following case presentation in a pediatric patient is utilized to discuss the issues following a major amputation.
Case report
A 12-year-old left hand dominant boy, with no chronic illnesses presented to the University Hospital of the West Indies after being involved in a motor vehicle accident. He had been traveling in a minivan with his right upper limb dangling through the window, when a car, ran into the side of his vehicle resulting in a complete transection midway through his right arm.
He arrived at hospital some 45 min postinjury accompanied by the amputated extremity which had not been cooled in ice. After resuscitation, he was immediately transferred to the operating theatre. The stump and the amputated extremity were not significantly contaminated. There was, however, moderately devitalized tissue.
Both ends were debrided and then irrigated with normal saline. An arterial shunt was placed across the brachial artery. The humerus was shortened 2 cm and then fixed with a dynamic compression plate (see figure 1). Definitive arterial, then venous repair was then performed, followed by epineural repair of the major peripheral nerves. All repairs were done primarily with the aid of magnifying loupes. The muscles of the anterior and posterior compartments were repaired. The repairs were protected in an above elbow dorsal plaster for 6 weeks. Postoperative potassium and other electrolytes were found to be normal. Physical therapy was commenced with passive range of motion exercises of the major joints and splinting in a functional position.

Day two postoperative X-rays of the right arm.
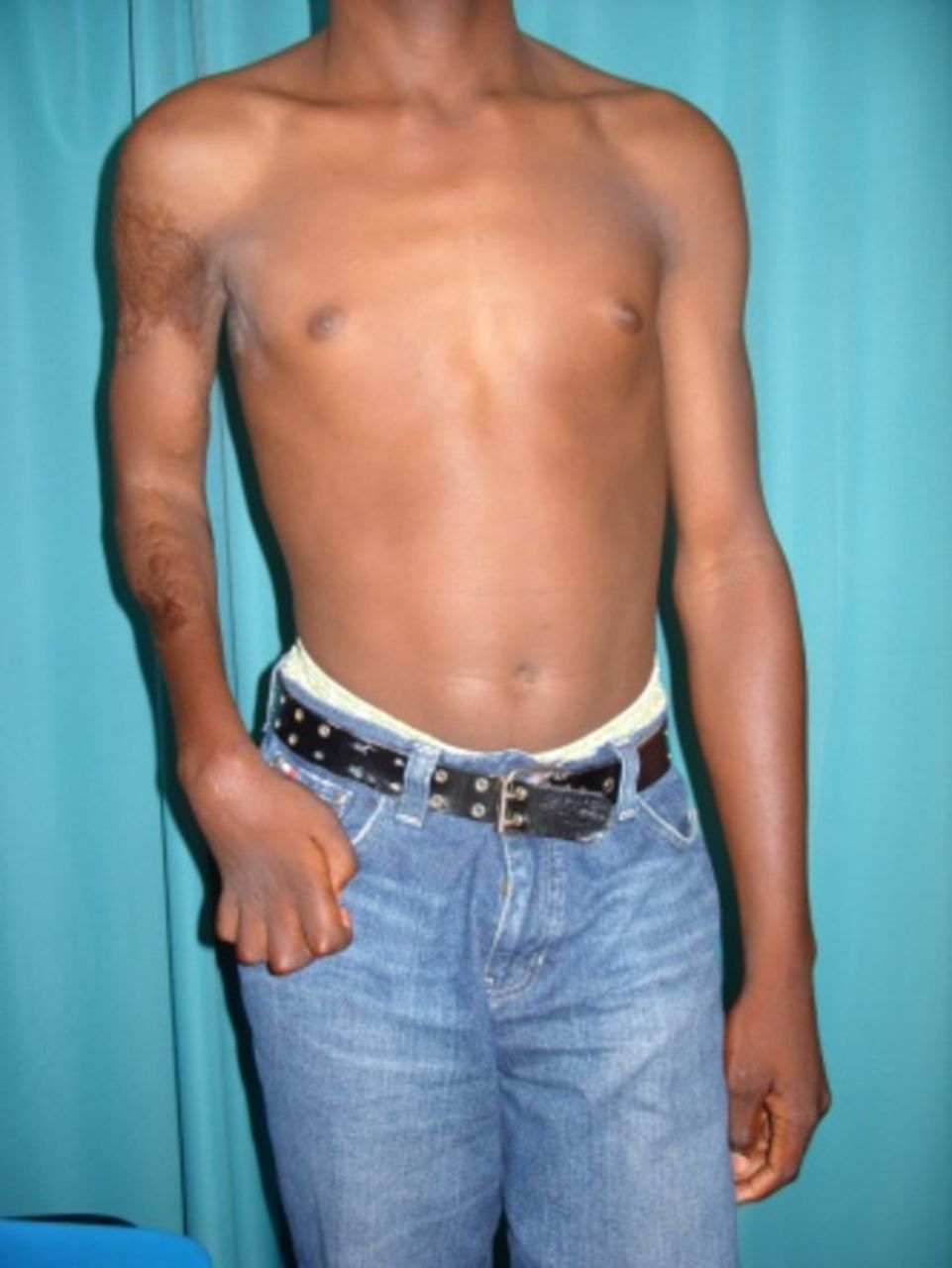
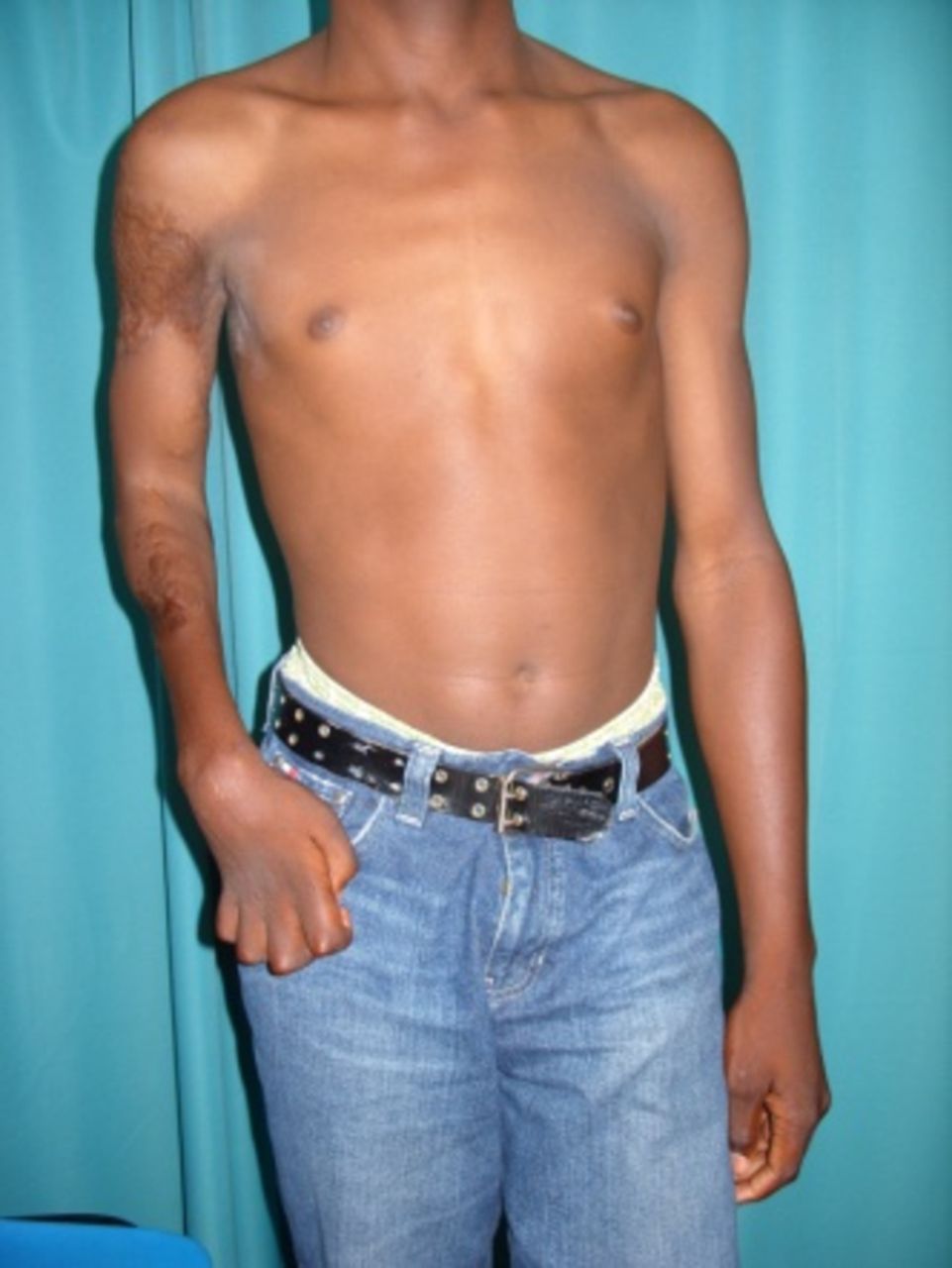
Four years postoperatively, he had 5–80 degrees of active range of motion (AROM) of elbow flexion. He had a 40 degree wrist flexion contracture and AROM was 40–60 degrees of wrist flexion. There was an inability to abduct or adduct all fingers. The fingers were all 40 degrees hyperextended at all of the metacarpophalangeal joints. He had fixed deformities of 90 degrees at the proximal interphalangeal joints and 45 degrees at the distal interphalangeal joints (see figures 2–4). All myotomes in which there was movement had either grade two or three power. He had partial sensation of the median and ulnar nerve autonomous zones. There has been no sensation in the radial nerve autonomous zone. Peripheral pulses were normal.

Lateral view of the patient 4 years postinjury.
Anteroposterior view of the client 4 years postinjury.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Dorsal view of the right hand 4 years postinjury. Demonstrating numerous deformity involving the wrist and digits.
He had to repeat a year (grade) in school, but was currently passing all of his classes at school. He participates in sporting activities in a very limited capacity; however, this was not much different to his preinjury activity level.
Although there was suboptimal function, both patient and parents were satisfied with the overall surgical result as their main concern was preservation of the limb. They had no interest in secondary procedures being performed to improve function. He and his parents were satisfied with the appearance of his pain-free limb. He enjoyed a good relationship with his peers.
Discussion
Reimplantation involves reconstitution of all the separated components of an extremity including anastamosis of the arterial inflow and venous return.1 2 Many types of trauma may result in a body part being separated from the body.1 2 In contrast to a lower extremity prosthesis, those available for the upper limb offer limited function. 3. Hand and digit reimplantations are common surgical procedures with well-defined indications and contraindications.4 Above elbow reimplantations are more unusual, with unclear indications.4 5 There are no papers which discuss functional results of large numbers of replants at similar levels except for distal levels.2
Amputations may be classified by the site of injury, type of injury (crush, sharp or avulsion) and degree of contamination and associated local injuries.2 Amputations of the upper limb may be divided into major and minor depending on whether the amputated part has significant muscle bulk.6 Major amputations are those at the level of the wrist or proximal, such as the index case.6 The more proximal the amputation, the greater the muscle load5 6 and muscle does not tolerate ischemia well.5 6 Proximal amputations have poorer prognosis.2 6 7 The major reason for poor outcomes of high-level reimplantation is difficulty in restoring nerve function. This may result in joint stiffness, joint instability, infection, skin and muscle necrosis.7–9 Proximal amputations are also associated with an increase in the number of required secondary procedures.6 The greater the time required for severed nerves to regenerate to the end plates, the worse the chances of recovery.10 This factor also applies to children.11 Saies et al 11 found that age did not affect functional outcome; however, children less than 9 years of age had a significantly higher rate of limb survival.11
Patients suffering from a traumatic amputation often demand reattachment without appreciation of the implications. The patient must be prepared for a long rehabilitation process.4 Factors such as lengthy hospital stays and multiple admissions, loss of productivity, lost wages, prolonged time lost from work, family hardships and psychological stress should be discussed with the patient.5 There is also the potential for a stiff dysfunctional limb.5
The stigma of disfigurement is often real due to cultural and/or environmental factors. For this reason, the patient may choose reimplantation, even in situations where poor function is a strong possibility. In some societies, amputees lose their social position.6 12 In this index case, the time lost from school because of lengthy hospital stays had dissuaded his parents from undertaking secondary procedures.
It is generally accepted that young age is a strong positive predictive factor with regard to performing reimplantation,11 provided that the amputated part is not extensively crushed.13 Severe upper limb injuries differ in prognosis between children and adults.13 The major factor for the difference is the superior neural regeneration in part because of the shorter distances involved in nerve regeneration.6 13
Kleinert and Graham7 found that children less than 9 years old had greater return of sensation. Since children also have better vascularity and bone healing,13 there is almost unanimous agreement that reimplantation should be attempted at any level in the upper limb in children.3
Kleinert and Graham7 and Saies et al 11 found that mechanism of injury was the most important determinant of a replant survival, where a laceration had better survival rates than crush or avulsion. Sharp guillotine amputations have a much narrower zone of injury compared with crush or avulsion injuries. Crush injuries cause greater skin scarring and wider zones of injury in the bone, tendon, muscle, nerve and blood vessels. Traction on the vessels causes internal damage and shearing of their cutaneous branches.2 5 6 Kleinert and Graham’s7 literature review suggested that a return of function of the reimplanted part is most likely in young patients with distal, sharp injuries with short ischemic time. It was also noted that proximal reimplantations may also have good outcome if the mechanism of injury does not involve avulsion or crush injury. Any deviation from the ideal will likely produce less optimal results.7 14
The preoperative poor prognostic factors in the index case were the mechanism of injury being a crush injury and the level of the amputation; however, the degree of contamination and the amount of gross devitalized tissue was not severe. Increased serum potassium is related to extensive crush injury and when persistently elevated is associated with poor outcome.10 The index case had normal potassium level postoperatively.
Ischemic time is another important factor determining functional outcome.5 6 10 The permissible time is increased with cooling the amputated part.5 6 Cooling limits the inflammatory milieu and cellular degradation.5 Cold ischemic times greater than 12 hours and warm ischemic times greater than 6 hours are associated with a poorer prognosis.5 6 Cooling is important in proximal amputations because the permissible ischemia will be shorter due to higher metabolic demands of muscle.2 9 Excessive ischemic time may lead to reperfusion injury.2 10 The shorter the time interval between blood flow interruption and successful reperfusion, the greater the likelihood of restoration of function.2 7 10
Comorbid illness and personal habits, for example, nicotine, alcohol and medication must also be taken into account.12 The patients’ general physical condition has to be able to withstand both a prolonged operation and to compensate postoperatively for the potential systemic influences of the replanted part. Cold ischemic time, extent and type of tissue defect at the amputation site and total trauma load are all criteria used for the prediction of development of systemic disturbances.10 12
Using a two-team approach in theatre reduces ischemic time, where one team prepares the amputated part and the other prepares the amputation stump.12 Ischemic time may also be reduced by early referral and en route stabilization.9 For avulsion injuries, Chew and Tsai6 found that a forearm fasciotomy was required when the ischemic time was greater than 4 hours and also that fasciotomy was unnecessary when the time was less than 4 hours. The index case had 1.5 hours of warm ischemic time.
The wound assessment must include factors such as significant crush injury or significant contamination. These are relative contraindications to reimplantation.6 10 The initial surgical goal via thorough debridement and irrigation is to convert the injury into a clean wound.6 9 15 16 If this cannot be accomplished after the first debridement, the wound is left open and repeat debridement is recommended in 24–48 hours. The cleaner the severed limb is, the better the chance of functional restoration.8 Plastic surgery procedures such as flap coverage are particularly important when vital structures are exposed.6 Only functional muscle is sutured and less important muscle is removed to decompress the wound and the debulking may permit normal skin to provide coverage.8 In addition to debridement, broad spectrum antibiotics are also required to prevent infection.6
Bone shortening of the amputated part is performed to reduce tension on the microvascular repair. This may eliminate the need for nerve or vein grafts and further aid skin closure.2 6 9 16 Bone shortening should be minimized in children.17 Bone growth depends on the integrity of the bone, and in children, one must avoid disturbing the physis8 17 of a major joint.9
For more proximal reimplantation sites, more aggressive techniques of rigid internal fixation are preferable, usually via a standard sized dynamic compression plate as was used in the index case with at least six cortices on either side of the fracture.16 Surgical efficiency and speed are required for the initial process of stabilization, since it is the initial step to a successful operative outcome.16 A stable skeletal fixation acts as a scaffold on which the soft tissue is built6 and allows for early mobilization.1
Whether the artery or vein is then repaired first is based on surgeon’s preference.2 An arterial shunt may be used, such as in the index case, initially to minimize ischemia.6 A venous shunt may be used to wash out metabolites.6 The lack of blood supply in children manifests itself as varying degrees of Volkman’s Syndrome.8
The success of a functional reimplantation is closely related to the quality of reconstruction of peripheral nerves.18 Median and ulnar nerves have an organized fasciculated structure and may be reconstructed with an internal epineural suture,2 16 as was attempted in the index case. Poor nerve regeneration and poor return of sensory and motor function may cause poor patient satisfaction.18 Alignment in mixed nerve grafts are required to avoid excess tension.2 Lack of innervation can result in muscle fibrosis in children due to their muscle fibers being tenuous.8 Primary end to end tension free repair is performed whenever possible, as was done in the index case. Secondary repairs usually require nerve grafting.9 Grafts must be harvested from areas not suffering from crush injury.1
Postoperatively, physiotherapy plays a key role in terms of regaining function.6 9 19 The functional capacity afforded by reimplantation may only be realized if physiotherapy is done consistently, adequately and for extended periods.19 Rehabilitation usually includes intrinsic splints with outrigger supports and protected passive and AROM of fingers.6 Early motion of joints is encouraged to prevent contractures and facilitate strengthening of musculotendinous units.9 The index case was not compliant with supervised or home physiotherapy which likely contributed to his limited hand function. He also lacked motivation because he used his dominant left hand to perform all activities of daily living once it was feasible to do so.
For optimal results, proper cooperation and coordination is required between the referral centre, the operating theatre, postoperative monitoring, hand therapy and the dedication of the patient in participating in their rehabilitation.2 The therapy team is all encompassing and comprises surgeons, anesthetists, nurses, physiotherapists, social services, family and the patient.12
Any functional evaluation system must be simple, yet comprehensive.20 Zhong-Wei et al 20 developed a system intended to express functional recovery in terms which are realistic to everyday life. The system analyses the following categories:
ability to work
range of joint motion
recovery of sensibility
muscular power.
Using the above categories, the four grades described were Grade one—excellent, Grade two—good, Grade three—fair and Grade four—poor. The first two grades are deemed worthwhile.20 Using return to work statistically as a measure of success has a few problems: performing white collar jobs may not indicate functional return.20 For children, return to school does not reflect functional return.6 20 It should also be noted that except in very young children, sensory recovery is never normal.6 The ability to gain independence in activities of daily living is considered an acceptable achievement in patients.7
Interestingly, patients may have suboptimal function but may still be satisfied with the result14 16 18 because of the esthetical aspect of the reconstruction and the extremity.19 The index case was satisfied with the surgical result despite having poor hand function, mainly because he was happy with the cosmetic result and psychologically preferred having ‘a natural limb’ as opposed to a prosthesis.
In recent years, there has been an improvement in prosthetic designs in terms of their form and function.21 Carlsen et al 21 presented a 50-year-old patient with a similar injury to the index case who was initially treated with an above elbow myoelectric prosthesis. The myoelectric prosthesis for this injury allows for intuitive control of elbow flexion and extension; however, activating a cumbersome switch is required for forearm rotation and hand control.21 The patient’s frustration with the prosthesis despite improved function resulted in a revision using an allograft humerus to increase the lever arm and provide rotational stability for her new prosthetic device. The patient was far more satisfied postrevision surgery.21
The decision with regard to performing reimplantation versus amputation is partly based on the expected functional result postoperatively.5 Reimplantation criteria will try to predict the functional and esthetic result of reimplantation. It is defined for the amputated part separately from the amputation stump.12 Worthiness of the stump is based on lack of deep contamination and lack of extensive soft tissue damage. Prognostic indicators for poor outcome post-reimplantation include crush or avulsion injury, warm ischemia greater than 6 hours, cold ischemia greater than 12 hours, multilevel disruption, advanced age, psychosocial disturbance and rehabilitation compliance concerns.2 5 12 The index case had a crush injury; however, he is young, had a warm ischemic time well within 6 hours and he did not have multilevel disruption; thus, he had overall favorable prognostic indicators.
Patients unwilling or unable to cooperate with intensive postoperative rehabilitation will not have good functional outcome.6 8 The surgeon must assess the prognosis of the injured limb adequately and accurately.8 If reimplantation is done before patient stabilization, their life may be endangered or poor functional outcomes may occur. Nowadays, viability alone is not sufficient to fulfill the criteria for successful reimplantation.12
Other considerations include:
lack of systemic disturbances secondary to the reimplantation
functional extremity according to Chen’s criteria
little or no pain of the reimplanted part
acceptable aesthetic result
acceptable rehabilitation time
social reintegration
return to normal life.19
After achieving a viable limb, the goal is to achieve a stable shoulder, active elbow flexion, hand sensation and an extremity that can hold and carry objects.4 Based on these aims, the goal was partially achieved in the shoulder and elbow, but not in the hand. The index case was happy with the appearance of his pain-free limb and enjoyed a good relationship with his peers. Successful reimplantations of the upper extremity at different levels have been reported with increasing frequency and consistent success.6 Magnification and the utilization of microsurgical loupes and the operating microscope are especially important in young children to achieve optimal results.13 Notwithstanding the smaller structures, the principles for reimplantation in children are identical to adults.8
Success of an operation may be defined by several parameters. Surgeons and patients often view success from different perspectives.5 Unfortunately, the resultant outcome is not always the expected outcome. This is a reflection of additive variables which dictate the final functional outcome.5
Mattiassich et al 22 analysed 16 patients from three trauma centers who underwent reimplantation using the disabilities of the arm, shoulder and hand scores, functional independence measurements and Chen’s criteria. After a mean follow-up period of 13.5 years, six patients were found to have very good function, eight had good function, one had fair function and one had bad function according to the Chen criteria. Despite this, all patients were satisfied with their function despite not having full function of the replanted appendage.22 In addition to reduced function of the replanted part, the literature has also recognized the potential for a new onset of anxiety and depressive symptoms.23 The Hospital Anxiety and Depression scale when utilized by Wendy et al demonstrated at least mild anxiety and depressive symptoms in 17 patients undergoing major upper extremity reimplantations with a mean follow-up period of 4 years. Of note, one patient committed suicide 3 years post-reimplantation and had no history of a psychiatric illness.23
Otto et al 24 performed the first extensive systematic review of the literature comparing the wearing of a prosthesis and reimplantation following traumatic arm amputations. There were 301 reimplantation cases and 172 cases managed with prosthesis. The authors acknowledged that the literature on upper limb prosthesis is somewhat lacking with regard to measurement of their functional capacity and outcomes. Despite this, the authors concluded that an arm reimplantation is more desirable compared with wearing a prosthesis because of an overall higher patient satisfaction in the former.24
At the time of injury, the patient and his parents were doubtful as to whether or not the limb would survive. They initially feared being told that a formal amputation would be required, which might have had major effects on them socially as well as psychologically. Once the limb demonstrated viability in the acute period, their major concern was the development of tingling, burning or shocking pains based on their general knowledge of recovery from a traumatic amputation. The achievement of a painless viable limb resulted in patient and parent satisfaction despite suboptimal function clinically.
Conclusion
The functional outcome following reimplantation of severe upper limb injuries in children are generally good. Despite higher cost, longer postoperative care and increased potential for secondary operations, reimplantation is considered functionally superior to prosthetic management. The generally improved quality of life therefore makes reimplantation a worthwhile procedure.
References
Footnotes
Contributors CF is the sole contributor to this article.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Provenance and peer review Not commissioned; externally peer reviewed.