Article Text

Statistics from Altmetric.com
A 79-year-old woman presented to the Emergency Department after a ground level fall. On arrival, the patient was hemodynamically normal with an unremarkable primary survey. The secondary survey demonstrated pelvic tenderness to palpation. A pelvic radiograph and subsequent computed tomography (CT) of the abdomen and pelvis demonstrated left inferior and superior rami, sacral wing, and iliac bone fractures with pelvic hematoma and a focus of contrast extravasation. Approximately 1 hour after initial presentation, the patient became hypotensive with a systolic blood pressure (SBP) of 76 mm Hg. The trauma surgery team was consulted. On evaluation, the patient was alert with appropriate mentation. The abdominal examination was notable for tenderness in the lower abdominal quadrants. Radial arterial line confirmed SBP <80 mm Hg, which was transiently responsive to intravenous fluid boluses. The patient carried a legal document and verbally stated that she was a Jehovah’s Witness and declined transfusion of all blood products; however, she would accept autologous transfusion or cell salvage.
What would you do?
Go to interventional radiology (IR) for angiography/embolization.
Go to the operating room (OR) for exploratory laparotomy with preperitoneal packing.
Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA).
Transfuse blood products.
What we did and why
Correct answer C
Given evidence of arterial bleeding, IR was consulted for angioembolization. We planned to proceed to the OR afterward for preperitoneal packing to control venous hemorrhage, and autotransfusion of blood recovered during the operation. Although unavailable in this particular case, a hybrid suite would have allowed for expeditious control of both arterial and venous bleeding.
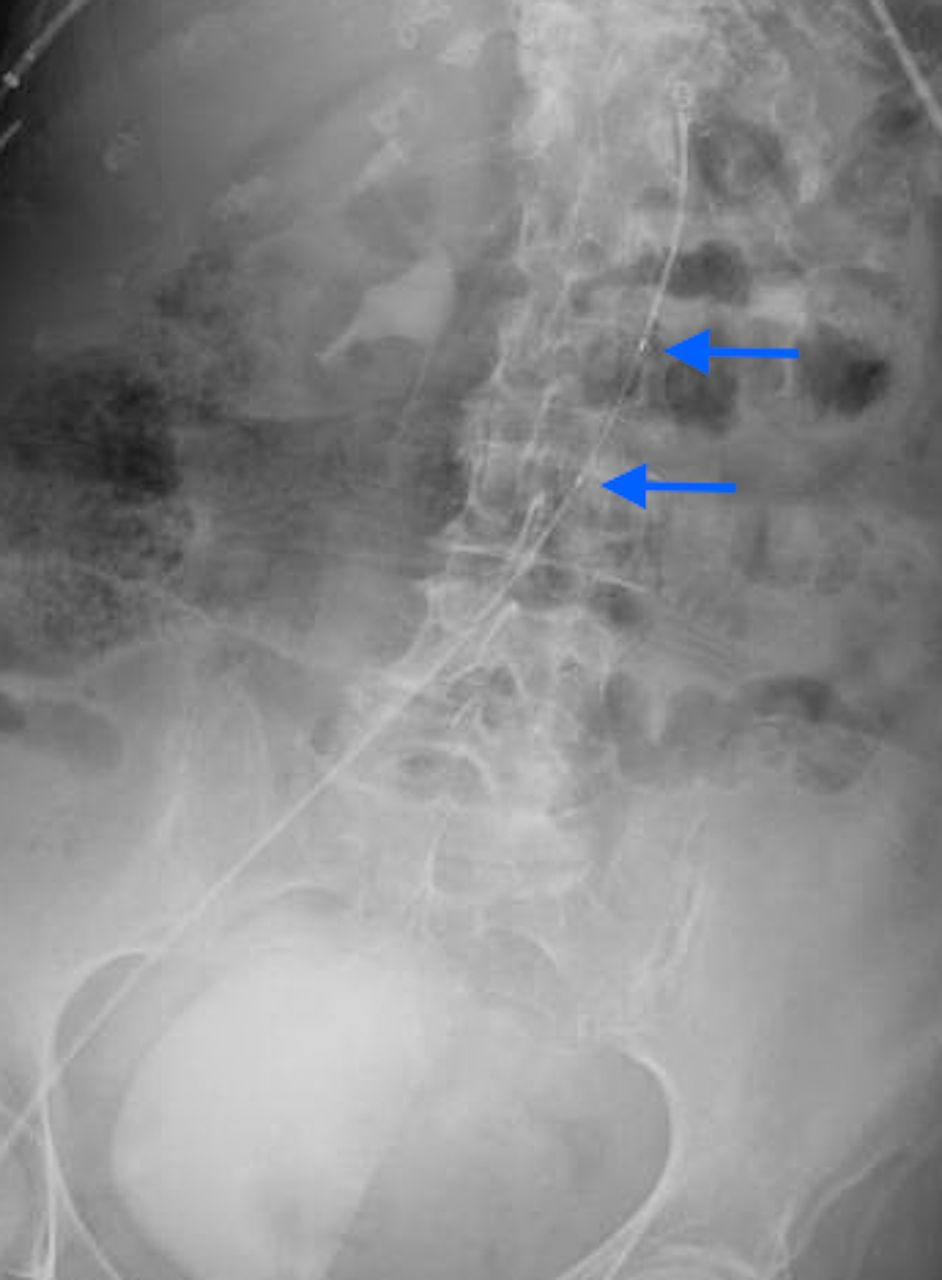
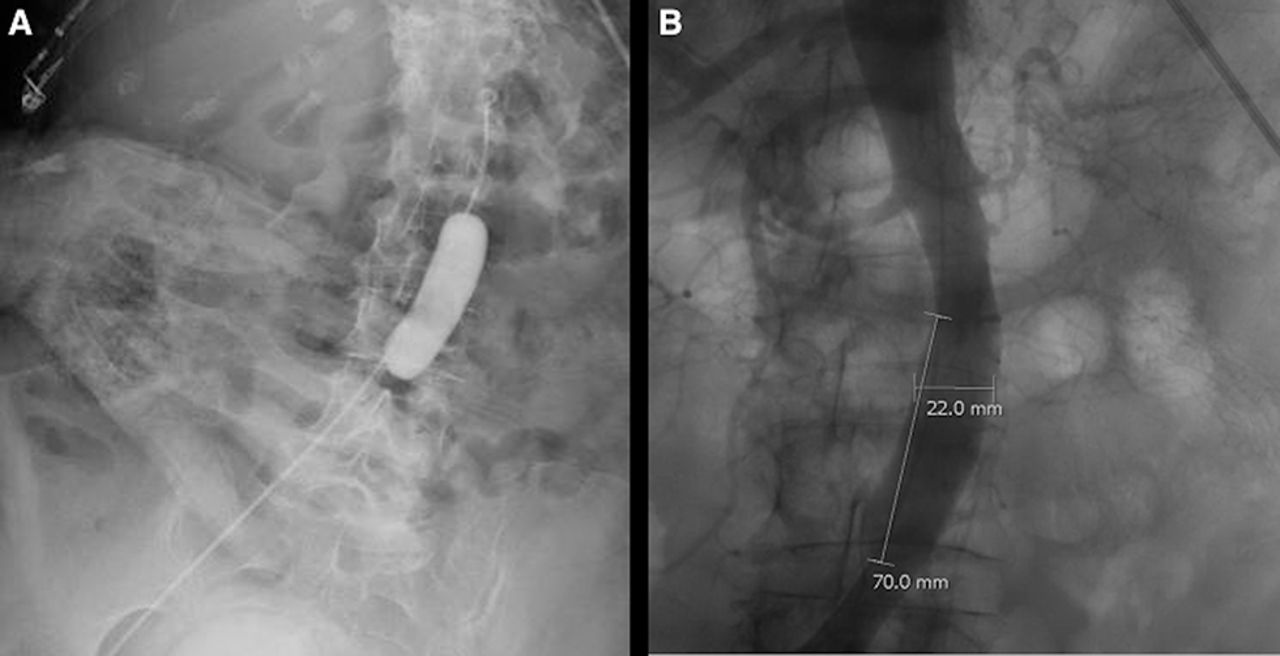
Prior to transport to IR, however, the patient became hemodynamically unstable and a REBOA catheter was placed. Under ultrasound guidance, a 7Fr sheath was inserted via the right common femoral artery, followed by the ER-REBOA catheter (Prytime Medical Devices, Boerne, TX). Per protocol for control of pelvic hemorrhage and placement in Zone III of the aorta (figure 1), the catheter was measured externally to the umbilicus and advanced without resistance. Balloon position was confirmed by a bedside radiograph (figure 2), and then it was inflated with a 50:50 saline to contrast solution. There was no increase in SBP despite confirmation of balloon inflation on X-ray (figure 3A). The balloon was further inflated to 12 mL with appropriate loss of bilateral femoral pulses; however, the SBP remained unchanged on both the device and radial arterial lines. The patient was transported to IR. Angiogram revealed active extravasation from a branch of the left internal iliac, which was embolized successfully. Aortogram revealed dilation of the infrarenal aorta from 1.5 cm to 2.2 cm. The area of dilation was noted to be the width and length of the balloon (2.2 cm×7 cm) (figure 3B). At the conclusion of the procedure, the patient required vasopressor support. We proceeded to the OR for preperitoneal pelvic packing, and autotransfused 250 mL of cell salvage. Postoperatively the patient progressed to require maximal vasopressor support. The patient's family elected to proceed with comfort care, and she passed away later that evening.

Aortic zones related to Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA). Zone I extends from the origin of the left subclavian artery to the celiac artery and is a potential zone of occlusion. Zone II extends from the celiac artery to the lowest renal artery and is a no-occlusion zone. Zone III exists from the lowest renal artery to the aortic bifurcation. REBOA in this zone may provide particular utility for instances of pelvic and junctional femoral (contralateral) hemorrhage. (Source: Stannard A, Eliason J, Rasmussen T. J Trauma Injury Infect Crit Care 71(6):1869-72).

Radiograph demonstrating REBOA catheter positioning. Arrows indicating the balloon. REBOA, Resuscitative Endovascular Balloon Occlusion of the Aorta.

{kind=link}
{kind=link}
{kind=link}
(A) Radiograph demonstrating the inflated aortic occlusion balloon. (B) Aortogram demonstrating the dilation of the infrarenal aorta.
REBOA is a minimally invasive intervention that can arrest hemorrhage and maintain cerebral and cardiac perfusion in the setting of bleeding from the abdomen or pelvis. In patients with pelvic bleeding, the balloon is deployed in Zone III, the infrarenal aorta above the bifurcation. Improvement in SBP with REBOA is well described, however, despite inflation of the balloon in the appropriate location, we did not see augmentation of the SBP. This has not been reported in the literature and was likely due to severe hemorrhagic shock in a patient who could not be resuscitated with blood products.
Morrison et al 1 reported REBOA-related morbidity rates at 3.7%, with rates of arterial injury, amputation, and non-fatal embolic event rates at 2.9%, 0.8% and 0.5%, respectively. Reports of dilation or aortic injury, however, are extremely rare. There are isolated reports of aortic injury in patients with diseased aortas, and with overinflation of the balloon in a diminutive aorta—neither of which was apparent in our patient. In summary, this is a unique case of a Jehovah’s Witness patient who did not demonstrate the expected hemodynamic response to REBOA, and additionally had a complication of aortic dilation with unknown clinical significance. This case hallmarks the importance of additional findings besides blood pressure response, namely absence of bilateral femoral pulses and radiographic findings such as CT diameter measurements, to confirm appropriate deployment of REBOA in a patient in severe hemorrhagic shock.
Footnotes
Contributors JN, N-KK, and ASQ provided care for the patient in question. ASQ and JLP performed the literature review and drafted the manuscript. JN and N-KK provided critical review.
Competing interests None declared.
Patient consent Not obtained.
Provenance and peer review Not commissioned; externally peer reviewed.