Article Text

Abstract
Background Trauma mortality due to exsanguination is the second most common cause of death. The objective of this study is to investigate the predictors for early death from exsanguination.
Methods A prognostic study was done to identify predictors of early mortality due to exsanguination. Data were extracted from our Trauma Surgery Registry database of Sultanah Aminah Hospital, Johor Bahru, Malaysia. All patients who were treated from May 1, 2011 to April 31, 2014 by the trauma team were included. Adult trauma patients included from the Trauma Surgery Registry were divided into two groups for analysis: early death from exsanguination and death from non-exsanguination/survivors. Univariate and multivariate analysis was performed to look for significant predictors of death from exsanguination. Variables analyzed were demography, mechanism of injury, organ injury scale, physiological parameters (systolic blood pressure (SBP), respiratory rate, heart rate, temperature), Glasgow Coma Scale (GCS), Revised Trauma Score (RTS), New Injury Severity Score (NISS), Trauma and Injury Severity Score (TRISS) and cause of death.
Results A total of 2208 patients with an average age of 36 (±16) years were included. Blunt trauma was the majority with 90.5%, followed by penetrating injuries (9.2%). The overall mortality is 239 out of 2208 (10.8%). Seventy-eight patients (32.6%) died due to central nervous system injury, 69 due to sepsis (28.9%) and 58 due to exsanguination (24.3%). After multivariate analysis, age (OR 1.026 (1.009 to 1.044), p=0.002), SBP (OR 0.985 (0.975 to 0.995), p=0.003) and temperature (OR 0.203 (0.076 to 0.543), p=0.001) were found to be the significant physiological parameters. Intra-abdominal injury and NISS were significant anatomic mortality predictors from exsanguination (p<0.001). Patients with intra-abdominal injury had four times higher risk of mortality from exsanguination (OR 3.948 (2.331 to 6.686), p<0.001).
Discussion In a Malaysian trauma center, age, SBP, core body temperature, intra-abdominal injury and NISS were significant predictors of early death from exsanguination.
Level of evidence II.
- mortality predictors
- exsanguination
- adult trauma
- malaysia
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Major trauma accounts for over 5 million deaths worldwide yearly.1 This is a major healthcare burden as it is the fifth leading cause of death among government hospitals.2
Causes of trauma mortality can be due to central nervous system (CNS) injury, multiorgan failure, sepsis or exsanguination. Exsanguination was reported to be the second most common cause of death after CNS injury in high-income countries with a reported mortality rate of 26.6%.3 Cause of reported trauma deaths may be different in other countries with reports from the Philippines that sees multiorgan failure/sepsis as the most common cause followed by exsanguination and CNS injury.4 Without an accurate trauma database, the causes of trauma deaths in Malaysia are still unknown and remain unreported.5
Early death from exsanguination is potentially preventable.6 Therefore, it is important to identify those at risk of mortality from exsanguination. Reported predictors from literatures were mainly from developed countries with an established trauma database.7 Among the reported predictors of death was pH of more than 7.2, body temperature of less than 34°C, blood replacement of more than 4000 mL, total fluid replacement of more than 10 000 mL and blood loss of more than 15 mL/min. Reported predictors for survival from traumatic injuries were presence of a penetrating trauma, spontaneous breathing, avoidance of emergency thoracotomy, Injury Severity Score (ISS) ≤20, packed red blood cell replacement of more than 4000 mL and absence of abdominal vascular injury.8 Using a large cohort from the CRASH 2 trial (Clinical Randomisation of an Antifibrinolytic in Significant Haemorrhage), Perel et al identified the parameters of age, Glasgow Coma Scale (GCS), systolic blood pressure (SBP) and income status of country as the strong predictors of 28 day mortality from exsanguination.9
Hospital Sultanah Aminah is a tertiary hospital located in the southern side of Peninsula Malaysia with a trauma surgery care team established since 2011. Trauma care in this center is managed by trauma surgeons with involvement of general surgeons. All patient data were recorded in the trauma registry and data collection was done prospectively. The objective of this study is to investigate and identify predictors of early mortality due to exsanguination and report the trends of mortality from a Malaysian trauma center.
Methodology
This is an observational prognostic study with a primary objective to describe the local epidemiology and identify predictors of early mortality due to traumatic exsanguination. Data were extracted from the prospective Trauma Surgery Registry database of Hospital Sultanah Aminah. All patients who were treated from May 1, 2011 to April 21, 2014 by the trauma team were included. Patient care was undertaken by the trauma surgery team that composed of trauma surgeons, general surgeons, medical officers and a trauma nurse coordinator. Inclusions of patients were extended to internal referrals by various disciplines within the hospital for potential traumatic bleeding. Pure neurotrauma and orthopedic trauma with no clinical signs of exsanguination were excluded from this registry.
Adult trauma patients extracted from the Trauma Surgery Registry were divided into two groups for analysis: early death from exsanguination and death from non-exsanguination/survivors. Early death from exsanguination is defined as subjects who died due to traumatic bleeding within 72 hours from time of injury. A cut-off time of 72 hours was taken as data from a regional center showed more than 80% of death from exsanguination happened within this time frame.4
Data of interest were demography (age, gender, ethnicity), mechanism of injury (blunt, penetrating, blast), Abbreviated Injury Scale (AIS) of each organ injured, physiological parameters on arrival to emergency department (SBP, respiratory rate (RR), heart rate (HR), temperature), GCS, RTS (Revised Trauma Score), NISS (New Injury Severity Score), TRISS (Trauma and Injury Severity Score) and cause of mortality (sepsis, CNS injury, multiorgan failure, exsanguination). These data were chosen to be included in the analysis as they can be accurately obtained and previously reported in literatures as important risk factors for trauma mortality. Collection of these parameters reduced the likelihood of missing data, which might render the analysis inaccurate. The reason we chose NISS instead of the original ISS was because the original ISS uses only the highest AIS in each body region for total scoring. Compared with NISS, it uses the top three scores regardless of body region prior to summation of the squares.
Statistical analysis
Data were analyzed using SPSS V.16. Descriptive data were expressed as mean±SD for continuous variable and percentage for categorical variable. Univariate analysis was done with t-test, χ2 and Fisher’s exact test. Significant and clinically relevant variables were then included in multivariate analysis with binary logistic regression. A value of p<0.05 is considered statistically significant.
The study was conducted in compliance with ethical principles outlined in the Declaration of Helsinki and Malaysian Good Clinical Practice Guideline. As patient data were collected anonymously, declared consent was not required.
Results
A total of 2208 patients with a mean age of 36 (±16) years were included. The majority of patients composed of the Malay race with 46.9%, followed by the Chinese with 24.3% and Indians who were the least with 17.6%. There were 88.6% (1957) males and 11.4% (251) females. Blunt trauma was the majority of reported cases with 90.5% (1998), followed by penetrating injuries with 9.2% (204) and the remaining 0.2% sustained blast injuries.
Mortality trend
The overall mortality rate was 10.8% with 239 deaths. Seventy-eight patients (32.6%) died due to CNS injury, 69 deaths due to sepsis (28.9%), 58 deaths due to exsanguination (24.3%), 7 deaths due to multiorgan failure (2.9%) and 27 deaths were recorded from multifactorial causes (11.3%).
Early traumatic death
Ninety-five (4.2%) patients died within the first 72 hours. From the mortalities, 58 patients died due to exsanguination and 37 patients died from severe head injury. Among those who died early due to exsanguination, 51 patients were male and 7 patients were female with a mean age of 39 (±18). Further analysis found 56 deaths that were due to blunt trauma and 2 more died due to penetrating injuries.
Physiological parameters
Among 2208 patients, we compared 58 patients who died early due to exsanguination with all other trauma patients admitted. Lower SBP, higher RR, higher HR, lower core body temperature and lower GCS were significant physiological parameters associated with early deaths from exsanguination (table 1). Age is not a significant parameter associated with early death from exsanguination shown by the independent t-test.
Comparison of physiological parameters between early death from exsanguination and death from non-exsanguination/survivors
Anatomic parameters
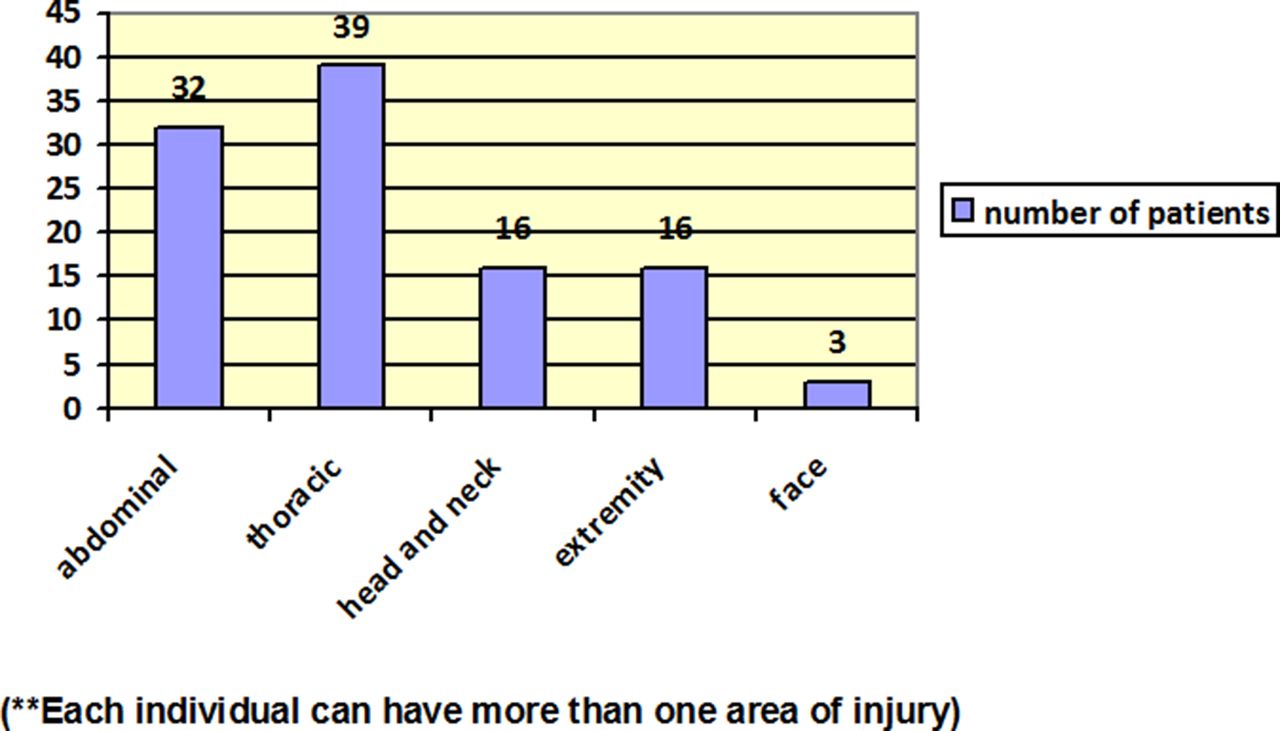
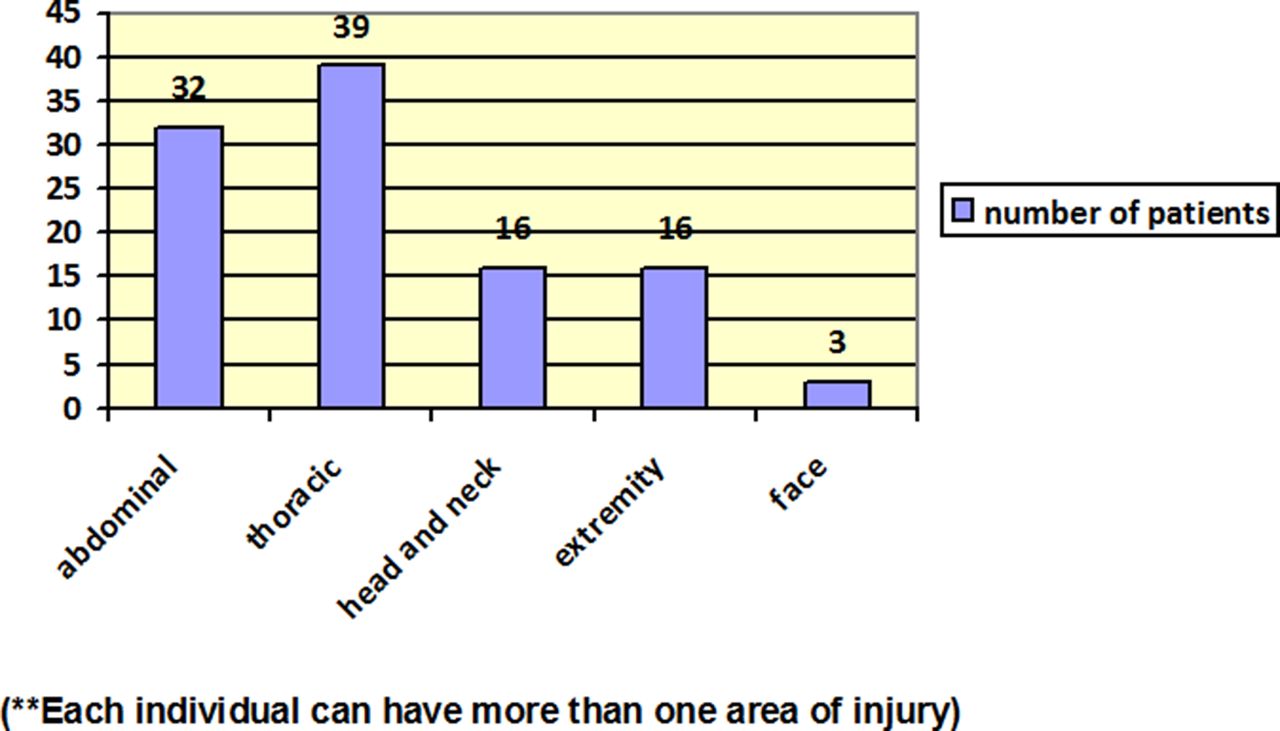
Analysis of the trauma database revealed that the majority of trauma patients sustained injuries to the thorax, followed by the extremities and the least were facial injuries (figure 1). Early death within 72 hours shared similar patterns with the results of the anatomic analysis revealing that the highest number of injuries from the thoracic region, followed by abdominal injuries and the least were facial injuries (figure 2). Interestingly, results of univariate analysis comparing risk of death against the reported anatomic injuries showed that the cohort of Malaysian patients had a four times higher odds at death when presented with an abdominal injury (p<0.001)(table 2).

Injuries according to anatomic location.
{kind=link}
{kind=link}
Death within 72 hours by anatomic location.
OR for death according to body regions
NISS, RTS and TRISS
Mean NISS for the trauma registry’s population was 19.39 (14.01), mean RTS is 7.3835 (0.9938) and mean TRISS is 0.9168 (0.1311). Compared with survivors and deaths from non-exsanguination, mean scores from the cohort of patients with early death from exsanguination were significantly higher. This is consistent with the finding that the higher the severity of injuries, the higher the risks of mortality in trauma patients (table 3).
OR for death comparing early death from exsanguination and death from non-exsanguination/survivors with NISS, RTS and TRISS
Identifying the predictors of early death due to exsanguination
Multivariate analysis was performed on all identified significant physiological and anatomic parameters using binary logistic regression with enter method. The analysis included age as a variable as it is widely reported in various studies as a significant predictor of early exsanguinating death.
Physiological parameters such as age, SBP and temperature were the significant predictors of early death from exsanguination. Significant anatomic predictors of early mortality were the presence of intra-abdominal injury and high NISS (table 4).
Multivariate analysis for the predictors of early death from exsanguination
Discussion
Age
Well-known predictors of death reported in various studies show that with an increase in age, there is a higher risk of death. Analysis of 507 trauma patients in a European emergency department revealed that an increase in every 1 year of age resulted in a 2% increased risk of death.10 Consistent with our findings, age was a significant predictor of death (table 1). The mean age in the trauma patients who died were 3 years older than the survivor group (table 1). Age was also a strong predictor of death as demonstrated from the large cohort study by Perel et al.9
Glasgow Coma Scale
Risk of early trauma mortality increases in the presence of neurological injuries.11 GCS is well acknowledged to predict multiple causes of trauma mortality.12 This is seen in trauma patients with no head injury where GCS was also shown to predict mortality.13 14 After multivariate analysis, our data report that GCS was not a significant predictor of early mortality, which is distinct from other reported literatures. Reduced conscious level or poor GCS that were not associated with head injuries may not be a significant predictor of mortality.
Systolic blood pressure
A report from Macleod et al revealed that presentation of SBP was a significant prognostic predictor of death from traumatic injuries.11 Analysis of SBP in a cohort of patients with traumatic bleeding performed by Perel et al also had similar findings, which further substantiates that SBP does predict traumatic deaths.15 Our analysis also reproduced results alike to the two aforementioned studies.
Core body temperature
Body temperature is the least reported parameter in the literature to predict trauma mortality. The reason it was reported less could be due to a difficulty in obtaining the core body temperature during rapid trauma resuscitation.15 With the development of infrared thermometers, core body temperature can be easily obtained even during rapid trauma resuscitation. Krishna et al published on core body temperature as a strong predictor of death in exsanguinating trauma patients.16 Physiologic deficits of hypothermia have a deleterious effect on the body, and it is an important predictor of early and late traumatic deaths.17 Multivariate analysis from our surgical trauma database revealed similar results conclusive that core body temperature predicts early trauma mortality (table 4).
Anatomic parameters
With univariate and multivariate analysis, the abdomen is the only body region that was significantly associated with early death from traumatic bleeding. The odds of dying from an abdominal injury increased fourfold when compared with other parts of the body being injured (tables 2 and 4). Presence of abdominal injuries was not a significant risk to exsanguinating trauma deaths. Instead, head injury is the most significant anatomic region reported that resulted in early mortality from traumatic injuries.10 11 Patients with pure head injury were excluded from our Trauma Surgery Registry as they were managed solely by the neurosurgical department. However, there was a subset of patients from our registry that had severe traumatic injuries with concurrent head injuries. Hence, the results of the multivariate analysis that showed head injury was not a significant predictor of death may be affected by our exclusion criteria of patients with pure head injury. Similarly, thoracic injuries were also a significant predictor of deaths found in many literatures.18 Recent updates in trauma clinical practice advocate the use of injury severity scoring as a guide by anatomic region injury severity.19 Therefore, by identifying the anatomic region being injured that comes with a higher risk of death may facilitate a more precise triaging of patients in accordance to individual severity.
Limitation
The hospital’s Trauma Surgery Registry is from a single-center experience, and results from other tertiary centers may affect our results. However, we think that our results may be the most accurate representation of Malaysian trauma surgery data as our hospital is the pioneering and only center with a subspecialized trauma surgery team. In addition, there are no comparative trauma surgery data in the country and our results are the first to be reported. Shortcomings of the trauma patient’s data accuracy and data loss in a non-computerized hospital system were kept to a minimum with a trauma surgery nurse dedicated to collect and maintain the prospective trauma registry. Any discrepancies in patient data were discussed among the trauma surgeon’s prior data entry into the trauma registry. The authors would like to highlight that the data included in the registry falls within the inclusion criteria of ‘multiorgan or multisystem trauma’, which affects two or more organ systems and excludes isolated neurosurgical or orthopedic injury.
Data on advanced imaging reports, specialized laboratory results, parameters of invasive hemodynamic measures, an estimated blood loss intraoperatively and blood product transfusion were excluded due to constraints of a non-computerized documentation system. The manpower needed to accurately register the aforementioned parameters would be enormous and daunting for a single trauma nurse to handle in addition to the clinical task of trauma patient’s nursing care.
Furthermore, the Trauma Surgery Registry was initially set up with intentions for a local center performance audit and later on modified into the current registry database. Due to a lack of technical support, certain key parameters were not entered into the SPSS spreadsheet where patient data were stored, which led to our limitation of collection of the clinical parameters.
Lastly, our hospital relies heavily on the manual documentation system and the initial resuscitation of trauma patients frequently involves multiple disciplines. The various teams respond quickly, which makes clinical documentation scattered or missing and difficult to trace.
Clinical application
The results from our analysis revealed that trauma patients who were more than 38 years old, lower SBP of less than 110 mm Hg, lower body temperature of less than 36.8°C and presence of an abdominal injury had a significantly higher risk of early exsanguinating deaths.
These identified predictors of trauma deaths are an important tool for prehospital and in-hospital triaging of patients. This may also instill a higher level of alertness for the primary emergency teams in activating the local general surgical/trauma team members.
Recommendation for future study
The current study composed of a low number of patients with early mortality from exsanguination. A larger cohort of trauma patients involving multicenters in Malaysia is needed to further develop a superior risk profile and scoring system to cater to our local population.
Conclusion
Age, SBP, core body temperature, abdominal injury and NISS were strong predictors of early death from exsanguination. The risk it carries in trauma mortality can be used as a tool to triage exsanguinating trauma patients in accordance to the severity of injury.
Acknowledgments
The authors would like to thank the Clinical Research Centre of Malaysia for the assistance provided throughout this research project. We also thank the Director General of Health Malaysia, Dr Noor Hisham Abdullah for his approval to publish this data. The authors would like to acknowledge the former Director of the Department of General Surgery, Sultanah Aminah Hospital, Mr Andrew Gunn, trauma surgery fellow Mr Azzudin and the rest of the trauma team members for their contribution to the trauma registry data collection.
References
Footnotes
Contributors TJH was involved in planning, conducting and reporting of the work described in the article. YM, RIA and HTCL were involved in the drafting of this manuscript. NMN was involved in conducting of the research with data cleaning.
Competing interests None declared.
Ethics approval Study was conducted in concordance with the Declaration of Helsinki. As it was done retrospective and anonymously, informed consent was exempted by the Malaysian Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.