Article Text

Abstract
Background Increased time to operative intervention is associated with a greater risk of mortality and complications in adults with a hip fracture. This study sought to determine factors associated with timeliness of operation in elderly patients presenting with an isolated hip fracture and the influence of surgical delay on outcomes.
Methods Trauma quality collaborative data (July 2016 to June 2019) were analyzed. Inclusion criteria were patients ≥65 years with an injury mechanism of fall, Abbreviated Injury Scale (AIS) 2005 diagnosis of hip fracture, and AIS extremity ≤3. Exclusion criteria included AIS in other body regions >1 and non-operative management. We examined the association of demographic, hospital, injury presentation, and comorbidity factors on a surgical delay >48 hours and patient outcomes using multivariable regression analysis.
Results 10 182 patients fit our study criteria out of 212 620 patients. Mean age was 82.7±8.6 years and 68.7% were female. Delay in operation >48 hours occurred in 965 (9.5%) of patients. Factors that significantly increased mortality or discharge to hospice were increased age, male gender, emergency department hypotension, functionally dependent health status (FDHS), advanced directive, liver disease, angina, and congestive heart failure (CHF). Delay >48 hours was associated with increased mortality or discharge to hospice (OR 1.52; 95% CI 1.13 to 2.06; p<0.01). Trauma center verification level, admission service, and hip fracture volume were not associated with mortality or discharge to hospice. Factors associated with operative delay >48 hours were male gender, FDHS, CHF, chronic renal failure, and advanced directive. Admission to the orthopedic surgery service was associated with less incidence of delay >48 hours (OR 0.43; 95% CI 0.29 to 0.64; p<0.001).
Discussion Hospital verification level, admission service, and patient volume did not impact the outcome of mortality/discharge to hospice. Delay to operation >48 hours was associated with increased mortality. The only measured modifiable characteristic that reduced delay to operative intervention was admission to the orthopedic surgery service.
Level of evidence III.
- hip fractures
- quality improvement
- mortality
- outcome assessment
- health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Traumatic injury in the elderly population is commonplace and accounts for 5.6% of all acute hospitalizations among Medicare beneficiaries.1 An acute hip fracture from a fall represents one of the most prevalent forms of traumatic injury treated by surgeons in the elderly.2 For a very small proportion of these acutely injured patients, surgical treatment of their hip fracture may not be desired by the patient or patient’s family because of a significant operative risk or the patient’s ambulatory status. These patients then transition to non-operative palliative care. However, the vast majority of patients undergo urgent operative treatment of their acute hip fracture. For these patients, the facility at which care is provided and the timing of operative intervention are potential factors influencing the optimization of short and long-term outcomes.
In adult patients undergoing hip fracture surgery, increased time to operative repair has been associated with a greater risk of mortality and complications.2 There are conflicting reports as to whether a wait time of 24 hours or less represents a threshold for minimizing adverse outcome risks for patients with hip fracture. A recent randomized controlled trial found no difference in mortality for patients undergoing surgery after a median wait time of 6 hours versus a median wait time of 24 hours.3 In addition to timing as a factor, the type of hospital in which the operation is performed may influence hip fracture outcomes. Hospitals can vary with regard to perioperative processes in place for injury evaluation and patient care. Patients may be treated in hospitals that are American College of Surgeons Committee on Trauma (ACS-COT)-verified trauma centers, or non-trauma center hospitals. The verification level of a trauma center has been found to impact outcomes in the setting of complex injuries such as pelvic ring fractures and blunt liver injury.4 5 Additionally, the admitting service for the patient has been shown to influence the outcomes of patients with hip fracture.6 7
In this context, we examined the perioperative outcomes and processes at 35 hospitals participating in the Michigan Trauma Quality Improvement Program (MTQIP). MTQIP is a Blue Cross Blue Shield of Michigan-funded collaborative quality initiative which uses enhanced trauma registry data collection.8 In addition to standard trauma registry data, MTQIP collects additional information on outcomes and processes of care, and employs a robust data validation program.9 In patients with an isolated hip fracture, this study sought to (1) determine patient and hospital-level factors that are associated with optimal operative outcomes and (2) examine the influence of surgical delay on patient outcomes. Specifically, we explored the impact of verification level of trauma center and admitting service on patient outcomes as well as surgical delay >24 and >48 hours on patient outcomes. In doing so, we aimed to identify which potentially modifiable factors are the most important to prioritize for improved outcomes for patients with hip fracture.
Methods
Study design
This is a retrospective cohort study of trauma patients who were treated at 35 ACS-COT-verified level I or II trauma centers participating in the MTQIP from July 2016 through June 2019. We investigated time to operative intervention in patients 65 years or older with evidence of an isolated hip fracture from a fall. We then examined the association of demographic, hospital, injury presentation, and comorbidity factors on experiencing a surgical delay of >24 or >48 hours and their impact on patient outcomes. The study outcomes included mortality or discharge to hospice, serious in-hospital complications, total hospital length of stay (LOS), and greater than 48-hour delay to operative intervention.
Data collection
Data collection is performed using the existing trauma registry at participating hospitals with a modular add-on for MTQIP-specific data.10 11 MTQIP publishes a data definitions dictionary based on the National Trauma Data Standard (NTDS), which is available online and updated annually. Trauma registrars and data abstractors from participating centers undergo training in MTQIP and NTDS data definitions. Data are transmitted to the coordinating center at 4-month intervals. Each MTQIP center undergoes an annual data validation audit.8
The inclusion criteria applied to form the analysis cohort are as follows: age ≥65 years; at least one valid trauma International Classification of Diseases-9th Revision or 10th Revision-Clinical Modification (ICD-9-CM, ICD-10-CM) code or Abbreviated Injury Scale (AIS) code consistent with a hip fracture (see online supplemental file); maximum AIS in extremity ≤3; and the mechanism of injury was a fall. Excluded patients included those with no signs of life at initial evaluation (systolic blood pressure=0, pulse=0, Glasgow Coma Scale score=3), those with a maximum AIS score >1 in other body regions, those who did not get a hip fracture surgery, and those missing data to calculate time to operative repair.12
Supplemental material
Statistical analysis
Univariate differences in patient characteristics by group were evaluated using χ2 test or Fisher’s exact test for categorical variables and analysis of variance F tests or Kruskal-Wallis tests for continuous variables. Outcomes of interest included rates of in-hospital mortality or discharge to hospice, serious in-hospital complications, total hospital LOS, and greater than 48-hour delay to operative intervention.
Multivariable logistic regression models were used to account for differences in patient and trauma center characteristics, allowing for risk adjustment at the patient level. Patient characteristics that were non-constantly related to the outcome through all values of the variable were entered into the models as categorical instead of continuous covariates. Adjusted ORs were reported for logistic regression models. A negative binomial regression was used for the outcome variable hospital LOS. Additionally, to account for the possibility that hospitals contributed to differences in outcomes, we adjusted for within-hospital clustering by using robust SEs.
Average values were expressed as the mean±SD. All statistical tests were two sided. Statistical significance was defined as p value <0.05. Statistical analyses were performed using Stata V.15.1 (StataCorp, College Station, Texas).
This study was submitted to the University of Michigan Medical School Institutional Review Board and given a determination of ‘not regulated’ status as secondary use of data from a quality assurance and quality improvement clinical activity.
Results
Out of 212 620 patients in the MTQIP database, 10 182 met our inclusion criteria for patients with an isolated hip fracture (figure 1). Of these, 3731 patients presented to level I trauma centers and 6451 presented to level II trauma centers.

Cohort diagram for inclusion/exclusion criteria. AIS, Abbreviated Injury Scale; ED, emergency department; MTQIP, Michigan Trauma Quality Improvement Program.
Patient characteristics
Table 1 describes the general characteristics of the patient population. The mean age of the patients was 82.7±8.6 years, and 68.7% were female. Approximately 90% of patients in each cohort were of white race. The rates of most comorbid conditions were similar in the level I and level II trauma center cohorts. Significant differences between patients treated at level I versus level II trauma centers were seen for chronic renal failure, congestive heart failure (CHF), dementia, disseminated cancer, drug use disorder, functionally dependent health status, and obesity. Table 2 describes the characteristics of the patient population admitted to the various services (trauma surgery, orthopedic surgery, other). The overall rate of mortality or discharge to hospice was 3.5% for this patient population, and the rate of complications was 5.5% (table 3). The mean LOS was 5.4±3.1 days.
Patient characteristics by trauma center verification level
Patient characteristics by admitting service (trauma, orthopedic surgery, other)
Unadjusted outcomes by trauma center verification level
Factors associated with outcomes
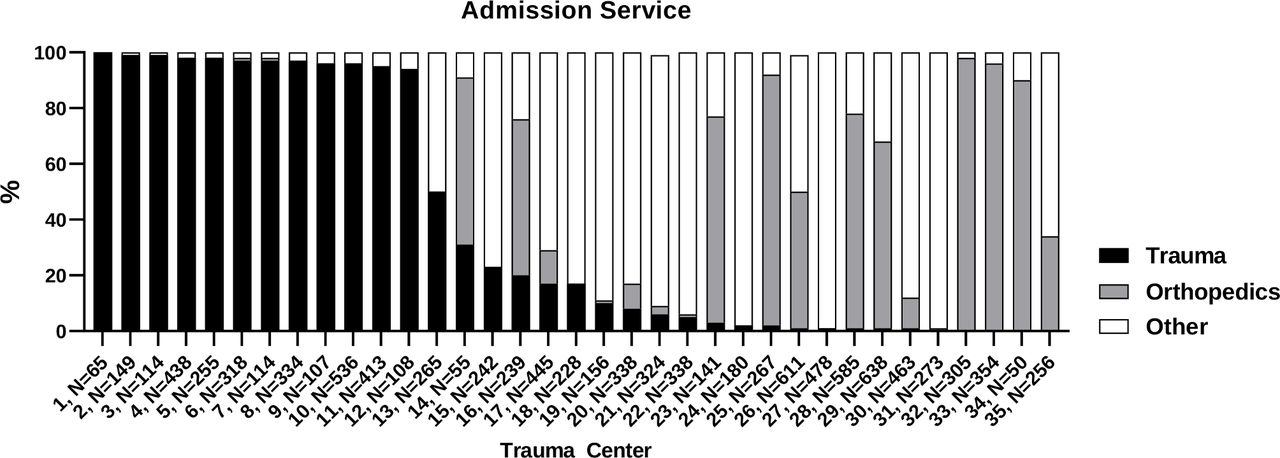
There was substantial variation in the hospital volume of patients treated for isolated hip fractures across trauma centers, ranging from 50 to 638 patients (figure 2). The service to which patients with isolated hip fracture were admitted also demonstrated wide variation among trauma centers. Overall, 33% of patients were admitted to the trauma service, 27% to the orthopedic surgery service, and 40% to ‘Other’ which is most commonly the internal medicine or hospitalist service. Table 4 illustrates patient, hospital, clinical, and comorbid factors associated with mortality or discharge to hospice, complications, or hospital LOS. There were no significant differences in the outcomes of mortality or hospice, complications, or hospital LOS for admission to a level I versus a level II trauma center. Admission to the orthopedic surgery service was associated with significantly decreased complications (OR 0.61, 95% CI 0.40 to 0.94, p=0.02) and hospital LOS (regression coefficient −0.12, 95% CI −0.22 to 0.02, p=0.019) when compared with the trauma service as the reference. The volume of patients with isolated hip fracture treated at a trauma center was not associated with differences in mortality or discharge to hospice, complications, or hospital LOS.
Patient outcomes (mortality or hospice, complications, and hospital length of stay) by hospital and patient characteristics

{kind=link}
{kind=link}
Admission service.
Operative delay
Delay in operation >24 hours occurred in 4643 (45.6%) of patients and delay in operation >48 hours occurred in 965 (9.5%) of patients. Delay in operation >24 hours trended towards increased mortality or discharge to hospice, but was not statistically significant (online supplemental file). Delay in operation >48 hours was associated with a risk-adjusted increase in mortality or discharge to hospice (OR 1.52, 95% CI 1.13 to 2.06, p=0.006). Patients operated on >48 hours after admission also experienced significantly more complications and had a longer hospital LOS. There were multiple patient characteristics found to be associated with increasing the incidence of operative delay to >48 hours (table 5). These included male gender, functionally dependent health status, CHF, chronic renal failure, and the presence of an advanced directive limiting care. Admission to the orthopedic surgery service was associated with a reduced incidence of delay >48 hours (OR 0.43, 95% CI 0.29 to 0.64, p<0.001). The only factor associated with operative delay >48 hours that was also associated with higher rate of admission to ‘Other’ services was the presence of an advanced directive limiting care. However, the presence of an advanced directive did not lead to a significant reduction in the rate of admission to orthopedic surgery (online supplemental file).
Factors contributing to operative delay >48 h
Discussion
In this study, we determined that the hospital characteristics of trauma verification level, admission service, and volume of patients treated for isolated hip fractures did not impact our primary outcome of mortality or discharge to hospice for patients treated at level I and level II trauma centers. However, we found that a delay of operative intervention >48 hours was associated with increased mortality or discharge to hospice. The only measured modifiable hospital characteristic associated with significantly decreased incidence of delay >48 hours was admission to the orthopedic surgery service (table 4). Patient factors associated with delay >48 hours included non-modifiable factors such as gender, or comorbid conditions such as CHF and chronic renal failure, which are generally not modifiable in the acute setting without creating a delay in care. However, there may be benefit to optimizing those conditions within 24–48 hours of presentation prior to operation.
Trauma center designation (ie, level I vs. level II) has been shown to be associated with a reduced risk of mortality after trauma. In a retrospective observational study of more than 200 000 patients, trauma patients admitted to a level I center had a 15% lower odds of mortality compared with those admitted to a level II center.13 Additionally, for patients with a complex pelvic ring injury, treatment at a level I trauma center was associated with decreased mortality.5 In contrast, our study found no difference between level I and level II centers with regard to the outcome of mortality or discharge to hospice. This variation is potentially explained by the fact that operative management of hip fractures is considered a standard procedure for nearly all orthopedic surgeons whereas complex pelvic ring fixation is most often addressed by orthopedic trauma subspecialists. Thus, patients with hip fracture are more likely to have access to orthopedic surgeons qualified to perform the necessary procedure in a timely manner at level I and level II trauma centers.
Our study found that admission to the orthopedic surgery service was associated with a significantly lower incidence of operative delay >48 hours. Though these results are risk adjusted, our data are not granular enough to determine if these services were comanaged with hospitalists or geriatricians. Comanagement would be unsurprising given the literature demonstrating improved outcomes when patients with hip fracture are treated with a multidisciplinary ‘ortho-geriatric’ combined service. In a systematic review and meta-analysis of 18 studies, an ortho-geriatric comanaged service improved mortality and LOS after hip fracture.14 Additionally, a systematic review including 33 studies found improvements in outcomes and LOS for patients with hip fracture comanaged by hospitalists.15 Similarly, a pathway, or process management guideline, has been shown to decrease the time to surgery and mortality.10 The reason for these improvements in outcomes is likely multifactorial and would require a more rigorous qualitative understanding of the service structures and processes of individual hospitals.
There is a large body of evidence which supports the conclusion that increasing comorbidity burden is independently associated with increased risk of mortality. For example, in a prospective study of 2692 patients, those with dementia, chronic obstructive pulmonary disease (COPD), CHF, and/or cancer had a significantly lower odds of survival.11 Similarly, other studies have shown that liver disease, COPD, heart failure, Charlson index >2, and renal failure are associated with an increase in mortality after geriatric hip fracture.16 17 Our data, consistent with these studies, demonstrated that patient-specific factors such as CHF, liver disease, functionally dependent health status, and angina were associated with significantly increased risk of mortality.
Some studies, however, suggest that the increase in mortality seen in patients with hip fracture is not due to preoperative comorbidity burden, but rather, the hip fracture event itself. In a matched cohort study of 169 145 Danish patients, adjusting the fracture cohort for preoperative comorbidity burden resulted in no significant change in mortality. The study instead revealed ‘post-fracture conditions related to the trauma’ to be significant predictors of mortality. Thus, the authors concluded that the major factor driving the increased rates of mortality seen in patients with hip fracture is the hip fracture event.18 Notably, however, the postfracture conditions that the authors found to be significant predictors of mortality included pulmonary disorders such as asthma and COPD as well as dementia and psychiatric disease. It is likely that these same disorders were existing comorbidities even prior to the study, potentially limiting the conclusion that postfracture factors are more pertinent to mortality than prefracture comorbidity burden.
The timing of hip fracture surgery, particularly regarding what constitutes an ‘unacceptable delay’, has been vigorously debated in the literature. A systematic review and meta-analysis which included 16 observational studies demonstrated that, irrespective of whether the cut-off was defined as 24, 48, or 72 hours, patients who received earlier surgery had a significant reduction in mortality.19 An additional meta-analysis comprised 35 studies and 191 873 patients confirmed the findings that surgery within 48 hours is associated with lower mortality.20 These findings align with our data which demonstrate increased risk of mortality after a delay >48 hours. Additionally, while our results for delay >24 hours do not meet our criteria for statistical significance, they suggest a trend that aligns with findings from previous studies demonstrating mortality benefit if surgery is performed within 24 hours.21 22 In contrast to our findings, there are several smaller studies which found no correlation between surgical delay >24 hours and mortality.23 24 The reason for this difference in findings is unclear but may be attributable to our choice of excluding polytrauma patients.
There are limitations to this study that merit discussion. As with all database studies, there is potential for data capture errors to occur; however, the rigorous data collection processes described above coupled with routine auditing minimize the frequency of error. Second, our database comprised sites only within the state of Michigan, and we only included patients treated at level I and level II-verified trauma centers, potentially limiting the generalizability of our findings. However, our patient demographics closely mirror the demographics of other database studies which use the National (Nationwide) Inpatient Sample (NIS) as well as prior literature describing the epidemiology of hip fractures.25 26 Third, this study did not examine specialty-specific outcomes such as non-union or malunion, both of which would be useful information for clinicians. Lastly, though our data are prospectively collected, this is a retrospective review and is subject to inherent biases and confounding. To mitigate this, we used multivariable models as well as robust SEs to account for clustering of patients within hospitals. Nonetheless, unidentified confounding factors always remain a possibility.
The results of this study provide clinicians with information regarding which patient-level and hospital-level factors are associated with mortality after hip fracture. These factors are important for surgeons to recognize and attempt to mitigate. Unlike several other emergency surgery procedures, our study suggests that for hip fracture surgery, trauma center-level designation and surgical volume are not associated with adverse outcomes. This information could be useful when designing triage guidelines—with patients with isolated hip fracture being treated more frequently at level II centers while prioritizing level I for complex polytrauma patients. Additionally, our study adds to the body of evidence documenting that operating within 48 hours is associated with lower mortality and fewer complications, though the impact of wait time <24 hours on mortality was less clear. Given the potential ethical implications of randomization between surgery before and after 48 hours, a large-scale retrospective study with a high degree of data fidelity such as ours may provide the highest level of evidence ethically attainable.
Acknowledgments
We would like to recognize the trauma registrars, MTQIP clinical reviewers, trauma program managers, and trauma program directors at the trauma centers for their dedication towards collection of the data and participation in MTQIP.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LG and MRH had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study conception and design: AJdM, BWO, MRH, LG, NS. Acquisition, analysis, or interpretation of data: LG, PCJ, MRH, NS. Drafting of the article: AJdM, MRH, LG, NS. Critical revision of the article for important intellectual content: AJdM, BWO, MRH, PCJ, LG, NS. Statistical analysis: LG, AHCN, MRH, BWO. Administrative, technical, or material support: MRH, LG, AHCN. Study supervision: NS, MRH, BWO.
Funding This study was supported by a Blue Cross Blue Shield of Michigan and Blue Care Network Collaborative Quality Initiatives grant and a Michigan Department of Health and Human Services grant to MRH for administration of the Michigan Trauma Quality Improvement Program. AHCN receives salary support from Blue Cross Blue Shield of Michigan/Blue Care Network (a non-profit mutual company) and the Michigan Department of Health and Human Services through grant funding of the Michigan Trauma Quality Improvement Program. PCJ is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number UL1TR002529.
Disclaimer The funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Michigan Trauma Quality Improvement Program (MTQIP) is exempt from IRB approval as a quality improvement activity. Secondary use of MTQIP data has been approved by the Michigan Medicine IRB under application HUM00041947.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement Data are available upon reasonable request. Data are generally only made available to the participants in the quality improvement collaborative.