Article Text

Abstract
Health equity is defined as the sixth domain of healthcare quality. Understanding health disparities in acute care surgery (defined as trauma surgery, emergency general surgery and surgical critical care) is key to identifying targets that will improve outcomes and ensure delivery of high-quality care within healthcare organizations. Implementing a health equity framework within institutions such that local acute care surgeons can ensure equity is a component of quality is imperative. Recognizing this need, the AAST (American Association for the Surgery of Trauma) Diversity, Equity and Inclusion Committee convened an expert panel entitled ‘Quality Care is Equitable Care’ at the 81st annual meeting in September 2022 (Chicago, Illinois). Recommendations for introducing health equity metrics within health systems include: (1) capturing patient outcome data including patient experience data by race, ethnicity, language, sexual orientation, and gender identity; (2) ensuring cultural competency (eg, availability of language services; identifying sources of bias or inequities); (3) prioritizing health literacy; and (4) measuring disease-specific disparities such that targeted interventions are developed and implemented. A stepwise approach is outlined to include health equity as an organizational quality indicator.
- quality
- Healthcare disparities
- general surgery
- Multiple Trauma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
In 2012, a combined summit between the National Institutes of Health (NIH) and the American College of Surgeons examined issues surrounding surgical disparities.1 Experts determined disparities to be ‘differences in the burden of disease, injury, violence, or opportunities to achieve optimal health experienced by socially disadvantaged populations’.1 This includes patient relationships with healthcare providers, hospital systems, the legal system, and societal beliefs to understand modifiable factors that contribute to differences in clinical outcomes. Surgical disparities have been described among acute care surgery patients based on race, socioeconomic status, sexual orientation, disability and insurance status.2–4 Furthermore, geographical differences influence access to healthcare, particularly trauma, which can vary greatly between urban and rural markets.
Recognizing the need to understand and address how health disparities impact outcomes within acute care surgery, a national professional organization for acute care surgeons—the AAST (American Association for the Surgery of Trauma) Diversity, Equity and Inclusion Committee—convened an expert panel entitled ‘Quality Care is Equitable Care’ at the 81st annual meeting in September 2022 (Chicago, Illinois). Experienced surgeons and national health equity leaders engaged in an interactive discussion of the most important considerations of health equity. The aim was to address the impact of health inequity on clinical outcomes for acute care surgery patients, as well as propose a framework for incorporating health equity as a key quality metric (‘the sixth domain of quality’) within trauma centers and healthcare organizations.
Health disparities and health inequities in trauma
Under the Emergency Medical Treatment and Active Labor Act, patients with injuries are expected to receive equal access to emergent care and life-saving trauma services. However, inequities in trauma care are widespread. Black and other under-represented patients have worse trauma mortality rates than white patients, independent of other proxies for socioeconomic status, and worse long-term functional outcomes.3 5 The deleterious effect of being uninsured on outcomes after trauma has also been well studied, with lack of insurance associated with increased mortality, reduced access to postdischarge services, and worse long-term financial outcomes.6–8 Health disparities can even lead to biases impacting care.9 On an institutional or structural level, it is important to consider the demographic data of patients and how systems treat individual patients from under-represented groups. Biases can be explicit or implicit and can add psychological trauma to the patient’s physical injury.10 11 Recent events such as the murders of Tyre Nichols, Ahmaud Arbery, Breonna Taylor, George Floyd and many more have highlighted the severe equity gaps within our healthcare systems and local communities.12 Many of these concepts of health equity and intersectional discrimination are now being explored within the acute care surgery community through work done by the EAST (Eastern Association for the Surgery of Trauma) Equity, Quality and Inclusion in Trauma Surgery Practice Committee.13
Furthermore, trauma itself is its own disparity. We do not have a National Institute of Trauma and only 3.7% of NIH-funded grants in FY2016 were trauma related, a missed opportunity to address disparities in trauma care.14 Trauma prevention programs are needed to target vulnerable populations, expansion of healthcare coverage, relocation of trauma centers to better provide for vulnerable populations, and the restructuring of clinical training to address implicit biases.3 To do this effectively, we need new metrics of equity in trauma and more robust research funding aimed at mitigating trauma disparities.
Social determinants of health and outcomes within acute care surgery
Achieving health equity—the ‘absence of systemic disparities in health between and within social groups that have different levels of underlying social advantages or disadvantages’—entails nuanced understanding of how the social determinants of health (SDOH)—the ‘economic and social conditions that influence individual and group differences in health status’—interact with biological factors, the physical environment, and clinical care to produce a range of important health outcomes.15
Research on SDOH in surgery has relied on composite neighborhood measures to approximate the social, economic, and environmental conditions of a patient’s lived experience. The Social Vulnerability Index was developed by the Centers for Disease Control and Prevention to identify and map communities most likely to need support due to hazardous events. The index evaluates four themes: socioeconomic status, household characteristics, racial and ethnic minority status, and housing type/transportation. Census tracts are assigned an overall ranking as well as a score for each theme. Other common indices include the Area Deprivation Index (increased geographic granularity), the Distressed Communities Index and the Child Opportunity Index.
Multiple studies have shown an association between neighborhood social vulnerability and increased risk of urgent/emergent presentation of common surgical procedures including cholecystectomy, colon resection, and hernia repair.16–18 Zhang et al introduced the concept of ‘access-sensitive’ surgical conditions that under optimal conditions (ie, primary care screening, insurance coverage, surgeon availability) should be treated electively, but without, have a natural course that progresses toward emergent presentation. Neighborhoods with high social vulnerability are more likely to undergo unplanned surgery, with farther travel and to lower rated hospitals, highlighting structural barriers to accessing care that contribute to delays and worse outcomes.18
Neighborhood socioeconomic vulnerability is associated with worse outcomes for trauma patients as well. Neiman et al found an association of social vulnerability with increasing inpatient mortality related to severity of injury at the time of arrival to the hospital.19 Long-term outcomes are also affected, with residence in a high-vulnerability community associated with increased risk of functional limitations, incidence of post-traumatic stress disorder and inability to return to work up to 14 months after injury.20
Further work is required to better understand the upstream social, economic, political, and structural mechanisms driving neighborhood influences on surgical outcomes, and to design effective interventions. Surgeons and health systems can start this process by engaging in relatively simple interventions. First, it is necessary to screen patients for social needs, including unmet housing, transportation, food, or financial needs. Screening tools are available through the American Academy of Family Physicians EveryONE project and the Centers for Medicare & Medicaid Services (CMS).21 22 Increasing geographic accessibility of surgical services in high-vulnerability communities may improve access to elective care for access-sensitive conditions. Finally, clinical registries such as the Trauma Quality Improvement Program (TQIP) can include geographic information at the census tract level to accurately measure neighborhood effects and target meaningful interventions. Understanding a patient’s community is central to designing high-quality surgical systems capable of meeting their needs.
Defining and measuring health equity metrics in acute care surgery
Appropriate capture of health equity metrics involves mixed-methods techniques. Quantitative outcomes pertaining to performance, for example, board certification, the presence of clinical guidelines, hospital characteristics such as volume, safety variation, use of electronic health records, and regionality, are all relatively straightforward to capture and frequently collect. It is also important to elicit additional quantitative SDOH, such as food insecurity, housing instability, a lack of access to transportation, an inability to afford bills, and exposure to interpersonal violence.23 Equally important and even more challenging are qualitative outcomes, such as patient-centered care metrics of satisfaction, bias, perceived quality, and decision-making. If combined, these data will help us better understand patient preferences and expectations across a broad range of sociodemographic and economic backgrounds. Developing health equity quality and safety performance improvement programs (QSPIP) will also enhance the doctor–patient relationship concerning shared decision-making, cultural preferences, priorities, and establishing of expectations. It is equally important to ensure ongoing research in health equity, so as to identify the unique disparities and barriers within one’s community.
Patient factors that influence outcomes include preoperative comorbidities and pre-existing biases, preferences and varying levels of health literacy, many of which are influenced by structural drivers and community determinants (eg, economic environments) which can impact their treatment course. Acute care surgeons can evaluate these metrics in the perioperative setting. Patient perceptions and engagement with the healthcare system can also be both measured and improved with respect to comprehension, perceptions, and willingness to engage in risk. These data would help surgeons tailor recommendations and improve outcomes.
Other important metrics measure availability and access to care. For trauma and Emergency General Surgery (EGS) patients, the availability and quality of rehabilitative (physician and occupational therapy) and postoperative services (mental health services, prescription services, palliative care) are essential components of access. In addition to availability of these resources, an assessment of patients’ postoperative and postdischarge expectations, as well as their individual ability to access this care (including identifying potential barriers such as lack of insurance, prohibitive travel distance), is essential. Regionalization of care can also influence trauma outcomes and must also be captured. Patients in rural settings may have further distances to travel to access high-level trauma care. Similarly, in urban settings, disenfranchised patients may be limited in access when compared with patients who do not rely on safety net hospitals. Measuring these multilevel indicators and examining each in exclusion as well as in parallel will help design a system that may improve outcomes in all patients.
Health equity as a quality metric: the sixth domain of quality
Although equity is one of the six domains of health quality, it is often considered the ‘forgotten aim’. Equity as a domain of quality is defined as ‘provision of care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status’. Currently, equity metrics are not widely used for hospital benchmarking, such as by the American College of Surgeons (ACS) National Surgical Quality Improvement Program or TQIP. Equity is only weighted at 5% of the composite benchmarking score in Vizient, a member-owned health services company that focuses on improving patient outcomes at reduced costs. Nonetheless, equity metrics may carry more weight in the future given recent announcements by the Joint Commission and CMS around their prioritization of and commitment to health equity.24
The ACS has a long-standing history of promoting healthcare quality through its verification programs. The ACS has described their four key pillars of continuous quality improvement: (1) setting standards to guide practice, (2) building infrastructure, (3) collecting data to measure performance, and (4) verifying performance through external peer review.25 For trauma centers, the standards of care outlined in the ‘Resources for the Optimal Care of the Injured Patient’ serve as the basis for the Verification, Review, and Consultation (VRC) program.24 In reviewing the existing VRC standards, the only standard that explicitly addresses equity is 5.13 which states: ‘In all trauma centers, the decision to transfer an injured patient must be based solely on the needs of the patient, without consideration of their health plan or payor status.’24 Thus, there is an opportunity to integrate equity considerations across all of the VRC standards.
With regard to infrastructure to promote equity, the VRC does not currently provide guidance to trauma centers. However, as part of the ACS Quality Verification Program, a non-subspecialty-specific program, infrastructure guidance focuses on institutional administrative and leadership commitment and on program scope and governance, creating a culture of patient safety and high reliability.26 Leadership commitment is essential to ensure equitable care and promoting a safe culture. With regard to program scope and governance, the Quality Verification Program calls for a surgical quality officer and for a surgical quality and safety committee. Institutions should build a similar infrastructure around equity, and in fact, many institutions are already doing so, such as by designating a leader in diversity, equity, and inclusion.
Other organizations committed to quality and equity have released guidelines around infrastructure that can be used by hospitals. For example, the Institute for Healthcare Improvement published a white paper describing a health equity framework which has five components: (1) make health equity a strategic priority; (2) develop structure and processes to support health equity work; (3) deploy specific strategies to address the multiple determinants of health on which healthcare organizations can have a direct impact; (4) decrease institutional racism within the organization; and (5) develop partnerships with community organizations.27
While trauma centers can address one or more of these components, they are not currently formally required to do so. TQIP does not report equity metrics and does not collect data on SDOH. While there are pros and cons of adjusting for SDOH, such information should be collected and used in reporting and evaluating hospital quality.
Evaluating equity as a domain of quality should be included in the trauma verification process. As the number of trauma center-affiliated, community-facing hospital-based violence intervention programs (HVIPs) grows, so do hospital–community partnerships.28 Strengthening HVIPs through the creation of medical–legal partnerships in trauma centers will fuse injury prevention and SDOH work with civil rights law.29–31 Thus, there are multiple opportunities for making equity an integral component of quality across trauma centers.
Ultimately, as with adjustment for SDOH, accrediting bodies need to monitor for unintended consequences—that is, for exacerbation of healthcare disparities through exclusion of high-risk patients. Thus, metrics might include representativeness of the center’s patient population as compared with the population in the communities being served and proportion of high-risk patients being transferred to other centers. To promote a meaningful change, centers will need to be evaluated for leadership commitment to, processes around, and infrastructure for equity, not just outcomes. There are multiple opportunities for making equity an integral component of quality across trauma centers which aligns with the Joint Commission’s new requirements to reduce healthcare disparities within ambulatory healthcare, behavioral healthcare and human services, critical access hospitals, and hospital accreditation programs effective January 1, 2023.32 This mandate will require dedicated leadership to implement strategies for reducing health disparities; screening patients for SDOH; and developing an action plan that describes how it will address identified health disparities in its patient population. Finally, for CMS, payment determination will be tied to mandatory reporting of SDOH.
Integrating health equity as a key quality metric in your institution
Despite its importance in trauma and across all aspects of healthcare delivery, few institutions have formally integrated health equity metrics in their curricula. In 2021, the New York University Langone Health (NYULH) created the Institute for Excellence in Health Equity (IEHE) in partnership with the Dean’s Office, the Office of Diversity Affairs, and Human Resources to focus on two fundamental goals: (a) achieving excellence in health equity research, clinical care, and medical education; and (b) fostering a culture of inclusive excellence across our health system.27 33 IEHE is built on four core pillars: clinical systems, medical education, research and community engagement. The clinical systems pillar focuses on adapting delivery systems to identify and mitigate health inequities and achieve excellence in health outcomes. The goals and deliverables for the clinical systems pillar are listed in box 1.
Institutional clinical pillars and objectives related to health equity
Develop heath equity quality and safety performance improvement program goals focused on addressing health inequities.
Develop dashboard metrics to capture health equity outcomes across clinical departments.
Collect and analyze data on health equity outcomes across the care continuum.
Modify electronic health records (Epic) to capture metrics for social determinants of health.
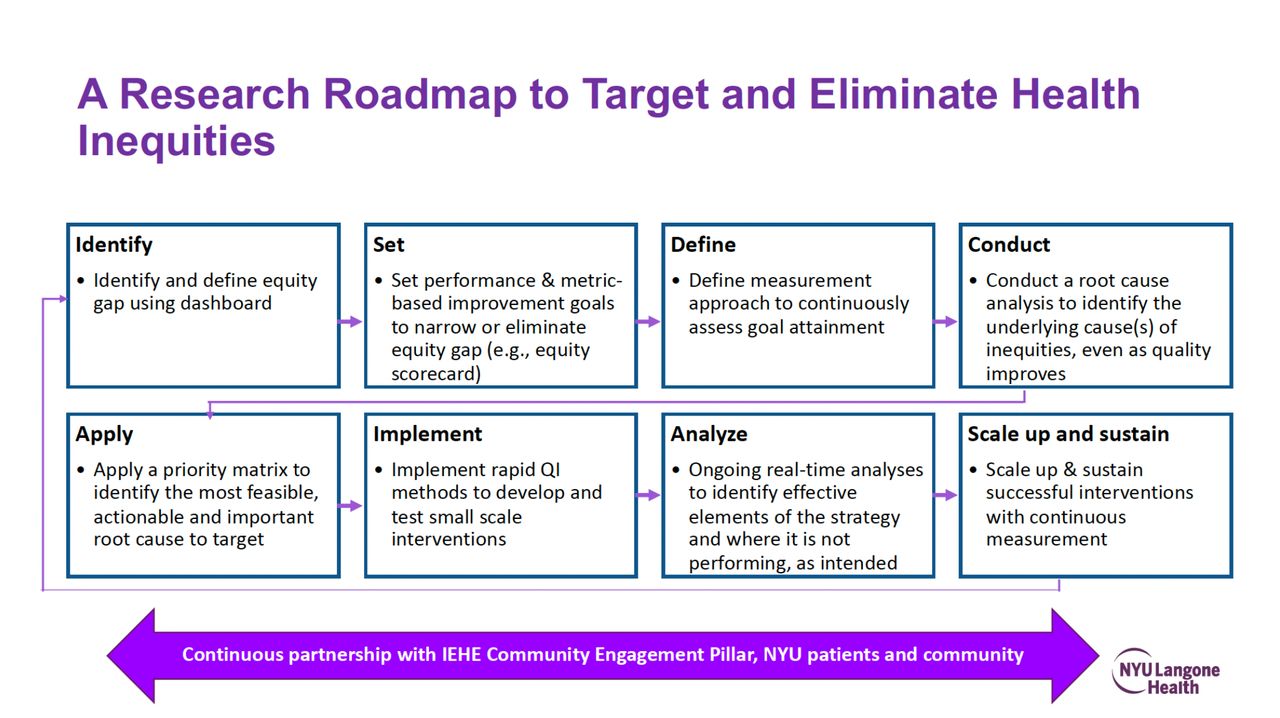
Health equity was adopted into a system-wide quality improvement framework, namely the NYULH QSPIP. Each clinical department was required to develop two health equity goals and implement projects according to a research roadmap in collaboration with IEHE (figure 1).

{kind=link}
Research roadmap to target and eliminate health inequities. IEHE, Institute for Excellence in Health Equity; NYU, New York University; QI, quality improvement.
By tying health equity to quality at a system-wide level, the focus shifts from documenting inequities in care to implementing changes to reducing gaps in care. Like all QSPIP goals, accountability is placed on the department chairs’ scorecards and reviewed midyear and at the end of the year with the Dean. The clinical systems pillar lead of IEHE collaborates and educates hospital leadership, department chairs and diversity and health equity department vice chairs regarding the process for health equity goals (table 1).
Processes for developing institutional health equity goals
Finally, a health equity dashboard assists departments and the healthcare system in further addressing health inequities. The dashboard created by IEHE in collaboration with the Office of the Chief Quality Officer, Chief of Hospital Operations, the medical center information technology department, and other stakeholders was designed to examine on a more granular level existing quality metrics which can be stratified by race, ethnicity, and language; sexual orientation and gender identity; insurance; and other demographic information. By developing this dashboard, the goal is to foster awareness that while departments may meet their metrics, quality improvement may not benefit all populations equally. The dashboard data can be used to apply an intersectional lens to our patient population and allow departments to start with small projects, which can be an educational and research opportunity for students and trainees to learn additional approaches to health equity and quality. By making interventions to address these inequities, departments will then track their performance. Further, data tracking will enhance an institution’s ability to plan and prioritize equitable outcomes by identifying system gaps and implementing strategies aimed at mitigation of inequities and eventually primary prevention.
Conclusion
Inequities are pervasive among acute care surgery patients. To identify ways to mitigate these disparities, health equity metrics must be accurately captured among our patients and used to drive change. This requires an organized and collective effort towards driving change which begins at the individual clinician level, but extends more broadly to trauma centers, health systems as well as professional organizations.
Ethics statements
Patient consent for publication
References
Footnotes
Presented at This article was presented as a lunch panel session from the AAST Diversity, Equity and Inclusion Committee at the 81st Annual Meeting of the American Association for the Surgery of Trauma on September 23, 2022, in Chicago, Illinois.
Contributors All authors contributed to the conceptualization, writing and review of this article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.