Article Text

Abstract
Background Antibiotic prophylaxis is routinely administered for most operative procedures, but their utility for certain bedside procedures remains controversial. We performed a systematic review and meta-analysis and developed evidence-based recommendations on whether trauma patients receiving tube thoracostomy (TT) for traumatic hemothorax or pneumothorax should receive antibiotic prophylaxis.
Methods Published literature was searched through MEDLINE (via PubMed), Embase (via Elsevier), Cochrane Central Register of Controlled Trials (via Wiley), Web of Science and ClinicalTrials.gov databases by a professional librarian. The date ranges for our literature search were January 1900 to March 2020. A systematic review and meta-analysis of currently available evidence were performed using the Grading of Recommendations Assessment, Development and Evaluation methodology.
Results Fourteen relevant studies were identified and analyzed. All but one were prospective, with eight being prospective randomized control studies. Antibiotic prophylaxis protocols ranged from a single dose at insertion to 48 hours post-TT removal. The pooled data showed that patients who received antibiotic prophylaxis were significantly less likely to develop empyema (OR 0.47, 95% CI 0.25 to 0.86, p=0.01). The benefit was greater in patients with penetrating injuries (penetrating OR 0.25, 95% CI 0.10 to 0.59, p=0.002, vs blunt OR 0.25, 95% CI 0.06 to 1.12, p=0.07). Administration of antibiotic prophylaxis did not significantly affect pneumonia incidence or mortality.
Discussion In adult trauma patients who require TT insertion, we conditionally recommend antibiotic prophylaxis be given at the time of insertion to reduce incidence of empyema.
PROSPERO registration number CRD42018088759.
- antibiotics
- empyema
- hemothorax
- pneumothorax
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Thoracic injuries occur in about 60% of all trauma patients.1–5 About one-third of these patients will have a diagnosis of pneumothorax, hemothorax, or hemopneumothorax.1–5 These can be treated with observation with or without serial radiological examinations, tube thoracostomy (TT) placement, or far less commonly, thoracotomy.
Antibiotic prophylaxis is administered for many operative procedures to decrease risk of superficial incisional surgical site infections (SSIs).6 Antibiotic selection is highly procedure-specific and based on the bacteria likely to be the source of the potential infection. The utility of antibiotic prophylaxis for bedside procedures such as TT remains controversial. The greatest concern with TT insertion revolves around the possibility of skin flora introduction into the sterile chest cavity, resulting in empyema thoracis (empyema). In addition, empyema treatment typically includes further invasive procedures, such as additional TT insertion, long-term central venous catheters for prolonged antibiotic therapy, video-assisted thoracoscopy, decortication, and occasionally even thoracotomy. A lesser concern is the development of a superficial incisional SSI at the site of the TT insertion, which may require local incision and drainage with or without therapeutic antibiotics.
In 2000, a practice management guideline from the Eastern Association for the Surgery of Trauma was performed, which found sufficient class I and class II data for a level III recommendation for prophylactic antibiotic use in patients undergoing TT.7 In 2012, an update was performed, which could not recommend for or against antibiotic prophylaxis for TT insertion for traumatic hemothorax or pneumothorax. Of note, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology was not used in the creation of either guideline.8 We performed a systematic review and meta-analysis and developed an evidence-based recommendation on whether patients with traumatic hemothorax or pneumothorax should receive antibiotic prophylaxis using the GRADE methodology.9
Objectives
Our population, intervention, comparator, and outcome (PICO) question was defined as follows.
The population of interest is adult (≥18 years old) trauma patients who require TT for traumatic hemothorax or pneumothorax. Our intervention is antibiotic prophylaxis given at TT insertion. The comparator group is no antibiotics. Our outcomes of interest are empyema, pneumonia, and mortality.
Outcome measures
A wide variety of clinically relevant outcomes related to chest trauma and TT insertion were considered, including hospital length of stay (LOS), duration of TT, and mortality. These were independently voted on by each team member on a scale from 1 to 9 per the GRADE methodology.9 Outcomes with average scores 7 to 9 were considered critical. Those with scores 4 to 6 were considered important, and those with scores ranging from 1 to 3 were considered of limited importance. After rounding to the nearest integer, only critical outcomes (scores seven or greater) were included in our final PICO question. Critical outcomes were empyema, pneumonia, and mortality.
Identification of references
Our project was registered with the PROSPERO registry of systematic reviews and meta-analyses (CRD42018088759). Published literature was searched through MEDLINE (via PubMed), Embase (via Elsevier), Cochrane Central Register of Controlled Trials (via Wiley), Web of Science and ClinicalTrials.gov databases by a professional librarian on March 7, 2020. The following Medical Subject Headings (MeSH) terms were included: chest tube, thoracostomy, trauma, hemothorax, pneumothorax, and antibiotic in various iterations and combinations (see online supplemental file 1 for the full search strategy).
Supplemental material
Language was limited to English. The date ranges for our literature search were January 1900–March 2020. Prospective trials, retrospective cohort, and case–control studies that included trauma patients, chest injuries and antibiotics were eligible for inclusion and retrieved. Case reports, commentaries, abstracts, reviews, editorials and animal studies were excluded. For a study to be included in our final analysis, a clear comparison between patients receiving antibiotic prophylaxis and control patients had to be present, as well as at least one of the critical outcomes reported.
Titles and abstracts were screened independently by two team members for inclusion in our meta-analysis. Conflicts were blindly adjudicated by a third member. Full-text review was performed in a similar fashion. Included articles had their reference lists reviewed by two team members for identification of potential additional articles. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram for our systematic review is depicted in figure 1.
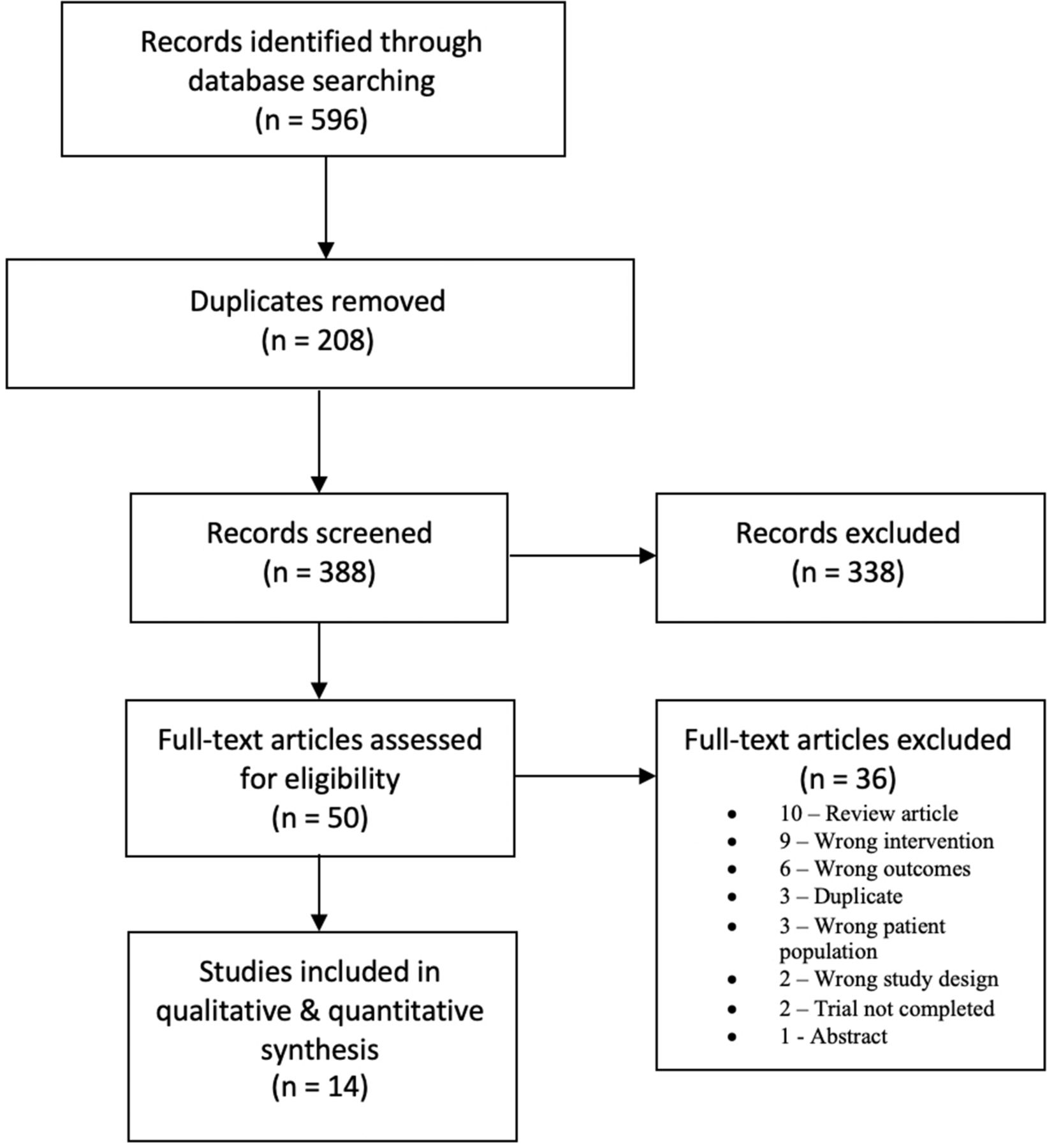
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram for study selection for analysis.
Data extraction and methodology
Data extraction from each included study was performed using a standardized data collection sheet and was performed in duplicate. Data extracted included authors, journal, publication year, study design, number of patients in antibiotic and control arms, bacteria cultured, type of trauma (blunt or penetrating), intervention details, and the critical outcomes previously listed. Skin flora were defined as bacteria commonly found on human skin, such as Staphylococcus spp and Streptococcus spp Respiratory flora were defined as bacteria commonly found in the human upper respiratory tract, such as S. pneumoniae, Haemophilus influenzae, and anaerobes.
Meta-analysis was performed in Review Manager (RevMan Online, The Cochrane Collaboration, 2021, Copenhagen, Denmark) with random-effects modeling to generate forest plots. Treatment effects were calculated with each study weight being proportional to the number of subjects it contributed to each outcome. For our binary outcomes (empyema, pneumonia, and mortality), ORs were calculated for the intervention against the comparator groups. Heterogeneity was calculated and quantified with I 2. High heterogeneity was considered present for I 2 values of >75%, moderate for I 2 values of 50% to 74%, and low if I 2 is <50%.10
Publication bias was evaluated using the Egger test, and the GRADE framework was applied to all quantified outcomes for assessment of bias, publication bias, inconsistency, imprecision, and indirectness. A sensitivity analysis to determine whether mechanism of injury (blunt vs penetrating) was associated with antibiotic effect was also conducted. Evidence profiles were created for each PICO using GRADEpro Guideline Development Tool software (McMaster University and Evidence Prime, 2021, Hamilton, Ontario, Canada).
All committee members voted initially independently taking into consideration the quality of evidence, relationship of benefits and harms, perceived patient values and preferences, and resource use. Although there was a majority, consensus was unable to be reached after several conference calls and rounds of voting. Our PICO question and analysis results (forest plots, GradePRO table, risk of bias assessment, and summary of study types) were submitted to two external GRADE experts for blind review. Results were discussed with the group, and majority (13 of 16) with dissent was able to be reached.
Results
Qualitative synthesis
Fourteen studies were included in the meta-analysis with publication dates ranging from 1977 to 2019.5 11–23 Available microbiology data are summarized in table 1.
Microbial data by study
The oldest study by Grover et al 11 was a double-blind, randomized control trial (RCT) of adult patients who underwent TT insertion after penetrating trauma. The antibiotic prophylaxis group received clindamycin from admission until either 1 day after TT removal or for 5 days, whichever came first. The remainder received no antibiotics. The antibiotic prophylaxis group had a lower incidence of pneumonia, positive pleural and wound cultures, and empyema. Pneumonia was diagnosed based on radiologic findings. Pleural cultures in the antibiotic prophylaxis group grew common skin flora. In the control group, pleural cultures grew common skin flora in two-thirds of the positive cultures. Wound cultures were also consistent with skin flora. Sputum cultures in the antibiotic prophylaxis group demonstrated 62% respiratory flora and 15% skin flora, in contrast to the control group, where sputum cultures were 29% respiratory flora and 36% skin flora. They concluded that antibiotic prophylaxis may confer an infectious benefit when used for penetrating trauma.
Stone and colleagues12 evaluated patients undergoing TT insertion in an RCT of penetrating wound victims conducted during 22 months.12 Patients received either a second-generation cephalosporin (cefamandole) or placebo, which continued from the time of insertion until 2 days after TT removal. All infections were due to bacteria susceptible to cefamandole. They did not separate bacteria responsible for pneumonias as opposed to empyemas. More importantly, the bacterial species responsible for the single case of empyema in the antibiotic prophylaxis group was also not reported. Skin flora, however, were responsible for the majority of infections. Patients who received placebo were eight times more likely to develop empyema or pneumonia, making the authors conclude that in patients with penetrating chest injury, antibiotic prophylaxis confers a benefit.
In a randomized study of patients from LeBlanc et al 13 blunt and penetrating trauma patients who required TT received either a first-generation cephalosporin (cephapirin) or no antibiotics from insertion to 24 hours post-removal.13 The antibiotic prophylaxis group had one patient with pneumonia, whereas the control group had one patient with pneumonia, one patient with empyema, and two patients with superficial incisional SSI. The difference in infectious complications did not reach statistical significance. The group pointed out in their discussion that this is a relatively small series (52 patients, with 26 in each group) and concluded that there was no obvious benefit to receiving antibiotic prophylaxis for TT insertion.
LoCurto and colleagues14 studied the use of prophylactic antibiotics for TT insertion in blunt and penetrating trauma.14 Patients were randomized to receive either a second-generation cephalosporin (cefoxitin) at insertion and continued until 12 hours post removal, or placebo. Pneumonia and empyema were significantly more common in the placebo group. No microbiology data were provided. The authors concluded that antibiotic prophylaxis did confer a benefit in patients undergoing TT insertion after either blunt or penetrating thoracic trauma.
Brunner et al 15 studied chest trauma patients who were prospectively randomized into two groups (antibiotic prophylaxis for skin flora (cefazolin) vs placebo) based on the date of their admission (even vs odd date).15 Cefazolin was continued for the entire duration of TT drainage. A total of six empyemas were identified. All were in the placebo group, and all were in patients with penetrating trauma. Of those, 83% grew skin flora. One blunt injury victim that did receive antibiotic prophylaxis developed pneumonia. The placebo group had three pneumonias, again all seen in penetrating trauma patients. They concluded antibiotic prophylaxis during the period of chest drainage may result in decreased infectious complications, particularly empyema.
Cant and associates16 studied isolated chest stab wound patients who required TT insertion within 24 hours of their injury in an RCT.16 Patients were randomized to receive either antibiotic prophylaxis for skin flora (cefazolin) or placebo during 24 hours. Pleural fluid was sent for culture at insertion. The most common pathogens cultured from the pleural fluid were skin flora; however, it is unclear whether routinely obtained cultures were of clinical importance. The placebo group had a higher incidence of both empyema and pneumonia. Antibiotic prophylaxis was also associated with a lower thoracotomy rate and consequent cost savings. Therefore, they recommended antibiotic prophylaxis for TT insertion for chest stab wounds.
In the RCT by Nichols et al,17 adult patients who sustained blunt or penetrating trauma and required a TT were given cefonicid or placebo at insertion and then daily until 24 hours post removal. Antibiotic prophylaxis was associated with significantly fewer episodes of pneumonia and empyema. All empyema and pneumonia cases were associated with penetrating trauma; however, there were only 6 patients (out of 116 included) who sustained blunt trauma. The empyema cultures from the placebo group were due to skin flora, whereas the pneumonia cases were due to respiratory flora. The authors therefore concluded that limited dosing of antibiotic prophylaxis was valuable in the prevention of pneumonia and empyema after TT insertion for thoracic trauma.
Gonzalez and Holevar18 prospectively studied patients with isolated blunt or penetrating thoracic trauma requiring TT insertion.18 Patients were randomized to receive cefazolin versus placebo using double-blind methodology for the entire duration of the TT. In patients who did not receive antibiotic prophylaxis, there were two patients with empyema from skin flora and two patients with pneumonias from a combination of respiratory and skin flora. There were no patients with empyema nor pneumonia in the antibiotic prophylaxis group. They concluded that isolated patients with chest injury would benefit from antibiotic prophylaxis during TT insertion.
Maxwell et al 19 conducted a multicenter RCT which studied the use of antibiotic prophylaxis during TT insertion for blunt and penetrating thoracic trauma during 34 months.19 For empyemas, skin flora were the predominant pathogens. For pneumonias in the antibiotic prophylaxis group, the cultures were polymicrobial. The pneumonias in the placebo group were both consistent with pansensitive respiratory flora. They found that pneumonia was more likely to occur after blunt trauma, whereas empyema tended to occur after penetrating injuries.
Villegas-Carlos et al 20 conducted an RCT in blunt chest trauma patients requiring TT.20 One group received antibiotic prophylaxis (cephalothin for 7 days), and the other placebo. No information regarding the microbiology of the infections were provided. There was no statistically significant difference in the incidence of empyema between the two groups.
More recently, the American Association for the Surgery of Trauma (AAST) sponsored a multicenter, prospective, observational study at 20 trauma centers from 2009 to 2011 of patients with retained hemothorax on imaging within 14 days of the initial TT insertion.22 The most common antibiotic prophylaxis used was cefazolin (84.1%) for skin flora. This group found no association between either the use of periprocedural antibiotics or antibiotic choice and subsequent development of empyema.
Grigorescu and Maghiar21 retrospectively studied 939 patients with both blunt and penetrating thoracic trauma that underwent TT insertion for hemothorax or pneumothorax.21 They stratified patients into those who received antibiotic prophylaxis (<24 hours), curative antibiotics (multiple antibiotics or one for >24 hours), and no antibiotics. The actual antibiotics used were not described. Logistic regression analysis showed that neither prophylactic nor curative antibiotics lowered risk for pneumonia and empyema. Of the six deaths reported, only one was due to infection.
In 2014, Heydari et al performed an RCT of blunt trauma patients needing TT. Patients were randomized into two groups, one group received antibiotic prophylaxis for skin flora (cefazolin) for 24 hours after TT insertion; the other did not.23 They demonstrated no difference in rates of empyema or pneumonia between the two groups.
In its most recent publication on this topic, the AAST sponsored a multicenter, prospective, observational study at 23 level I and II trauma centers from December 1, 2013, to November 16, 2016.5 A total of 1887 patients were included in the primary analysis (272 received antibiotic prophylaxis; 1615 did not). Although 14 different antibiotics were used, cefazolin was the most common. The nearest neighbor-matching method was used to match the 272 antibiotic patients with individual controls at a 1:1 ratio. There were no significant differences in empyema nor pneumonia rates.
Quantitative synthesis (meta-analysis)
Empyema
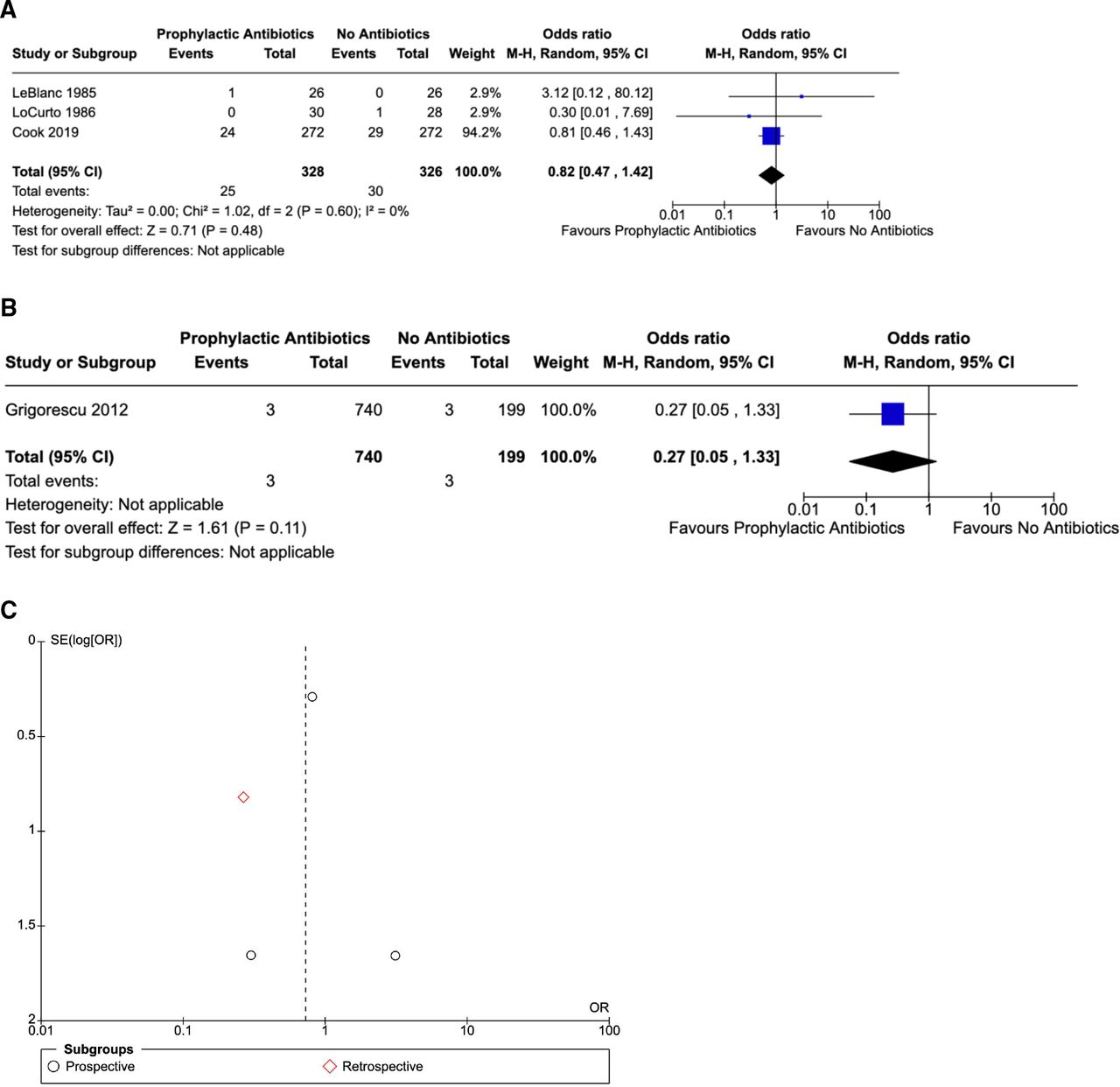
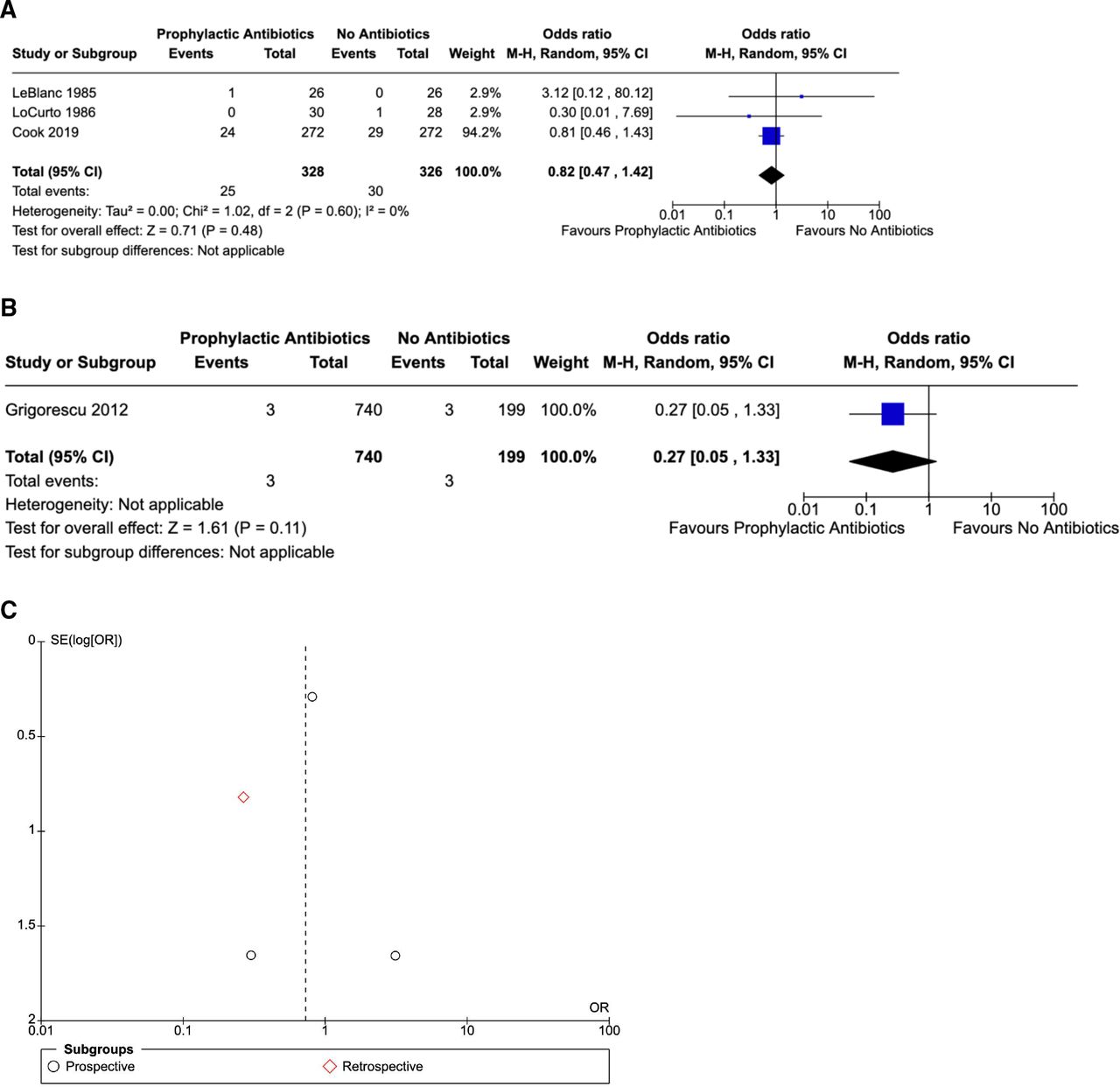
Fourteen studies compared empyema incidence in all trauma patients who were given antibiotic prophylaxis for TT insertion versus no antibiotics (figure 2A–C).5 11–23 In the prospective data, a total of 1057 patients received antibiotic prophylaxis, whereas 1018 patients did not (figure 2A). There were 44 patients with empyema who received antibiotic prophylaxis and 96 who did not. Heterogeneity was low. The pooled data showed that patients who received antibiotic prophylaxis were significantly less likely to develop empyema. In the retrospective data, 19 of 740 patients with empyema received antibiotic prophylaxis and 2 of 199 patients who did not (figure 2B).

(A) Empyema: all trauma (prospective). (B) Empyema: all trauma (retrospective). (C) Funnel plot: empyema all trauma (prospective). (D) Risk of bias assessment.
Patients were then divided based on mechanism of injury. Eight RCTs compared empyema incidence in penetrating trauma patients who were given antibiotic prophylaxis at TT insertion versus patients who received no antibiotics (figure 3A).11 13 15–20 There were only 5 patients with empyema in the antibiotic prophylaxis group (358 patients) and 29 in the control group (326 patients). Heterogeneity was low in the pooled data. Empyema incidence was significantly decreased in penetrating trauma patients who received antibiotic prophylaxis at TT insertion (p=0.002). Four RCTs studied antibiotic prophylaxis usage for TT insertion in blunt trauma patients (figure 3B).18–20 23 Heterogeneity was low. No statistically significant difference between the two groups was found (p=0.07).

(A) Empyema: penetrating trauma (prospective). (B) Empyema: blunt trauma (prospective).
Pneumonia
In the prospective data, there were 66 patients with pneumonia in the antibiotic prophylaxis group (845 patients) versus 74 in the no-antibiotics group (749 patients, figure 4A).5 11–19 23 Heterogeneity was moderate in the pooled data, and it should be mentioned that two articles diagnosed pneumonia based only on radiographic findings.11 23 A funnel plot is shown in figure 4C. The retrospective data showed no difference between the groups (figure 4B).

(A) Pneumonia: all trauma (prospective). (B) Pneumonia: all trauma (retrospective). (C) Funnel plot: pneumonia all trauma.
Mortality
Four publications that reported mortality rates with antibiotic prophylaxis usage for TT insertion in trauma patients (figure 5A–C).5 13 14 21 There was a low degree of heterogeneity in the pooled data. There was no statistical difference between the two groups.
(A) Mortality: all trauma (prospective). (B) Mortality: all trauma (retrospective). (C) Funnel plot: mortality all trauma.
Grading the evidence
Of the 14 studies included in the meta-analysis, 13 were prospective in nature.5 11–20 22 23
Eight were RCTs.11 12 16–20 23 One was a prospective observational study with 1:1 patient matching.5 The most common antibiotic used in the studies was cefazolin.5 15 16 18 19 22 23 In one study, the antibiotic used and the dose regimen were not mentioned.21 Antibiotic protocols in the other studies ranged from a single preprocedure dose to 48 hours post TT removal.
Eight studies recommended the use of antibiotic prophylaxis, three of which only studied penetrating trauma patients.11 12 16 Seven of these were published before 2000.11 12 14–18 Interestingly, the group of six studies that did not recommend antibiotic prophylaxis usage included three of the four largest studies.5 20 22
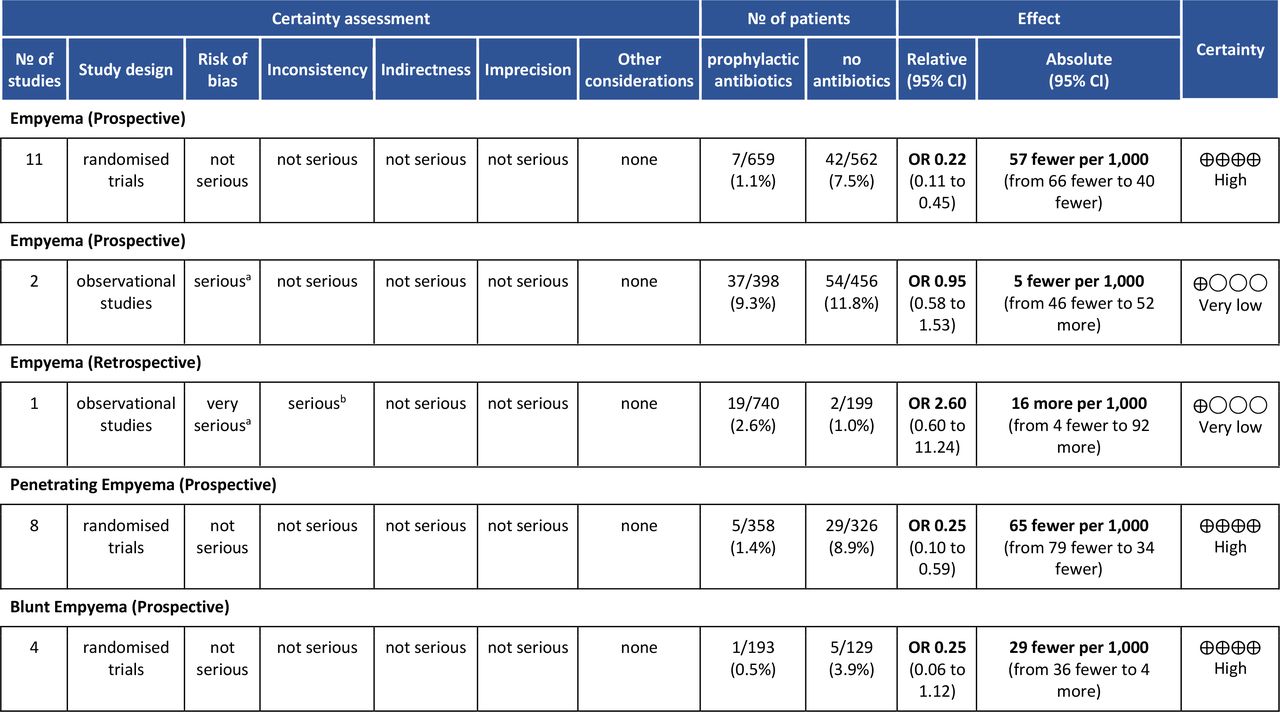
For patients with empyema and pneumonia, different antibiotics and different antibiotic protocols were used across studies. Some studies focused on only penetrating trauma patients, whereas others either focused on only blunt injuries or combined the blunt and penetrating trauma patients. In addition, there was variability in injury severity and blinding of treatment limbs. The overall quality of evidence for the RCT data is considered high, whereas the quality for the observational and retrospective data is considered very low (figures 6 and 7). Risk of bias assessment is shown in figure 2D.
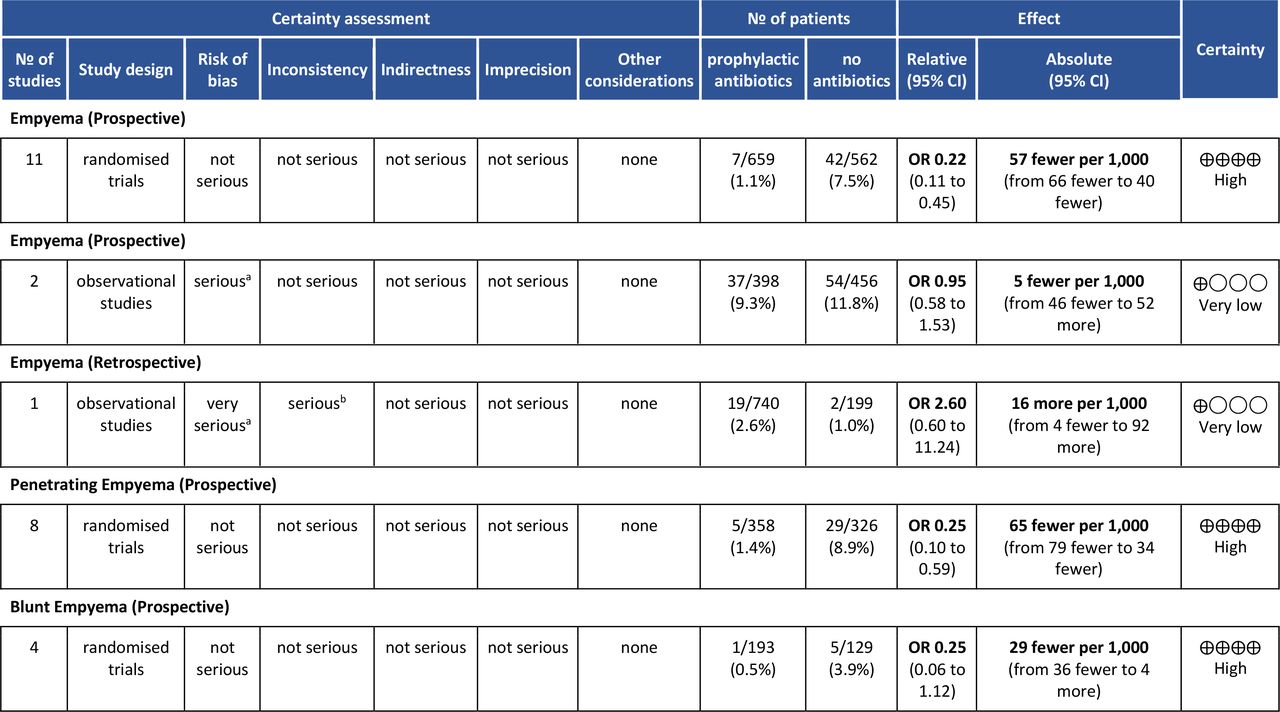
GradePro table: empyema. *See Risk of Bias assessment. †Different antibiotics and different protocols used.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
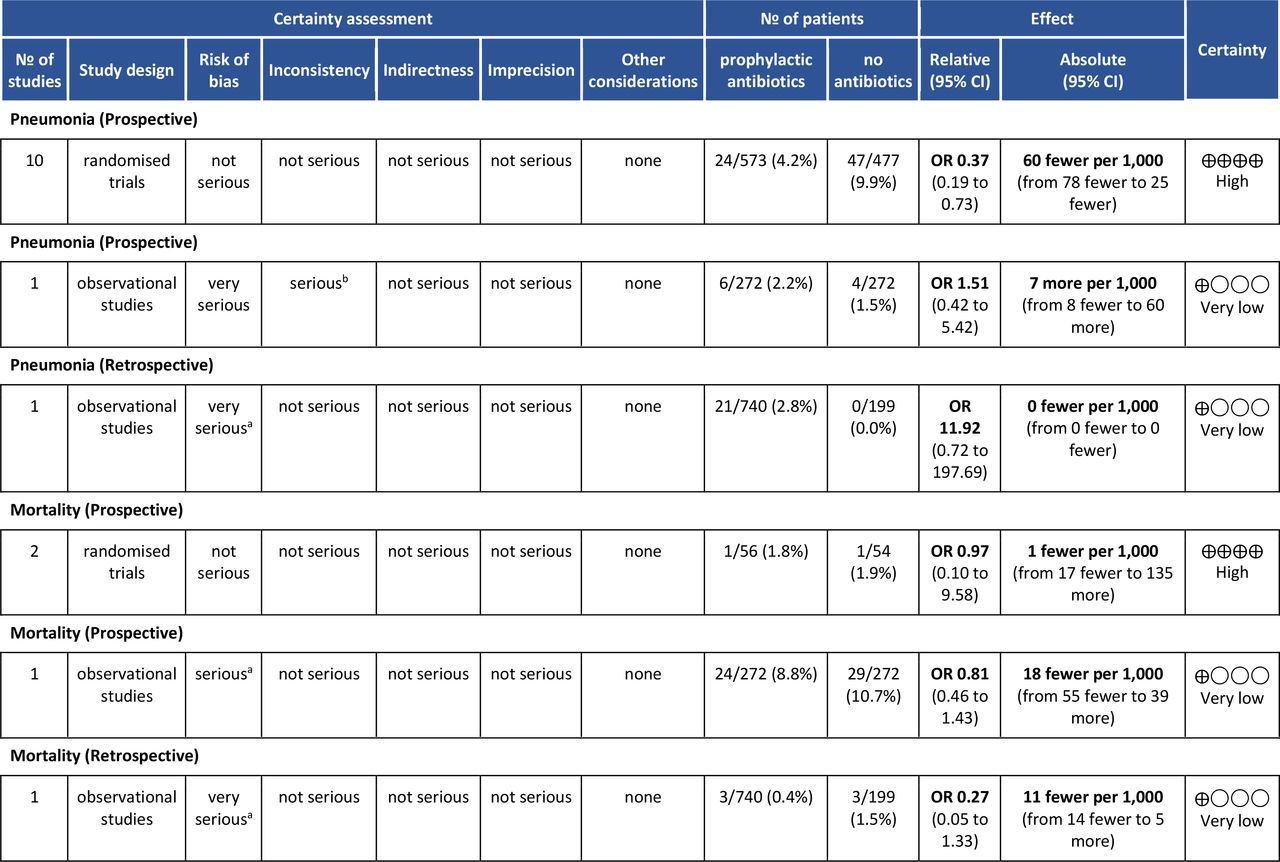
GradePro table: pneumonia and mortality. *See risk of bias assessment. †Different conclusions.
Discussion
This study found a decline in empyema incidence with antibiotic prophylaxis usage for TT placement. Subgroup analysis showed antibiotic prophylaxis was more impactful in penetrating chest trauma. There were no statistical differences in pneumonia and mortality rates. The previous guideline from 2012 could not make a recommendation regarding antibiotic prophylaxis usage due to insufficient evidence.8
There are several limitations to this study. Included studies varied in types of antibiotics given, treatment dosages and duration protocols. The two multi-institutional studies did not control the antibiotic protocol used, so the results are muddled with broad-spectrum and narrow-spectrum antibiotics as well as varying regimen durations.5 19 Two studies diagnosed pneumonia based on radiographical findings alone, creating a concern for overdiagnosis.11 23 However, when the funnel plot was analyzed, these two studies were consistent with the others included. In addition, there was no significant change in the OR with removal of these data. As a result, the working group chose to include these data to prevent the introduction of any selection bias.
In addition, how much temporal improvements in sterile technique at TT insertion, TT size, pain management and pulmonary toilet, and overall critical care management during the course of the last few decades affected infectious outcomes remains unclear. None of the studies provided information on skin preparation, draping, or insertion protocols. Changes in the management of retained hemothorax and use of early video-assisted thoracoscopic surgery or percutaneous empyema drainage were not discussed.
Routine antibiotic usage is not without consequences. Clostridioides difficile causes more than 450 000 infections and 29 000 deaths in the USA annually.24 Antibiotic exposure is the most common trigger, as it disrupts the normal bowel flora.25 Though most of the older studies do not mention C. difficile, Grover et al terminated their study early due to concerns from recent publications linking clindamycin usage to C. difficile infections.11 Most recently, Cook et al reported no difference in C. difficile colitis between the antibiotic prophylaxis and control groups, which is consistent with reported increases in community-acquired cases.5 24 In addition, Maxwell et al reported increased antibiotic resistance in cultures for patients who received both single and continuous dosing of antibiotics when compared with patients who did not receive any antibiotics.19
When the data are stratified by injury mechanism, there seems to be a greater benefit of prophylactic antibiotic usage for TT insertion in penetrating trauma patients, compared with blunt injuries. The majority of empyemas in these patients were caused by skin flora. It is unclear whether this is due to the procedure itself, the contaminated nature of the wound, or, more likely, a combination of the two. We suspect there is a combination of factors as there is a decrease in empyema incidence seen in blunt trauma patients (who would presumably have a sterile pleural cavity until TT insertion) receiving antibiotic prophylaxis, although it did not reach significance.
Infection prevention must be balanced with cost and resource management. Most of the studies did not show a difference in hospital LOS; however, LoCurto et al found an average 4-day shorter LOS with antibiotic prophylaxis.14 Cant et al showed fewer thoracotomies with prophylactic antibiotics, leading to lower hospital charges.16
Of note, there was no unanimity in the evaluation of the data or in the recommendation. Three dissenting members of the work group pointed out that during the temporal trend of the studies (figure 2A), there has been a decline in the significance of antibiotic prophylaxis during the more than 30 years of data, such that more recent studies did not demonstrate a benefit of antibiotic usage. It is possible that the visualized trend may be attributable to improvements in sterile technique, care bundles, smaller chest tubes, or other advances in protocolized trauma care.
Recommendation
We conditionally recommend that antibiotic prophylaxis be given at the time of insertion to reduce empyema in adult patients who require TT for traumatic hemothorax or pneumothorax.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Sarah Cantrell at Duke University Medical Center Library for her assistance with the literature search. Without her expertise and guidance, this project would not have been possible.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at Presented at Eastern Association for the Surgery of Trauma meeting on January 18, 2019 in Austin, Texas, USA.
Contributors CJV and BKY conceived and designed the study. CJV, BKY, KLH, GK, SHA, and JJC graded the outcomes. JJF, CJV and BKY reviewed the literature. JBB, CJV, BKY, GK, and JJF performed the abstract and text screens. CJV, BKY, GK, and JJF performed the data extraction. JJF, SHA, CJV, BKY, KLH, JBB, DK, EAL, AJK, AM, SA, NF, ERH, MLC, JJC, and GK graded and reviewed the evidence. JJF and SHA analyzed the data and drafted the article. GK and JJC oversaw the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.