Article Text

Abstract
Objective The purpose of this study was to determine if exposure to Prescription for Hope (RxH), a hospital-based violence intervention program (HVIP), is associated with reduced violent reinjury and new convictions for violent crime in the 2-year period after index hospitalization for a violent injury.
Methods This was a retrospective cohort study analyzing patients from two level I trauma centers in Indianapolis, Indiana. RxH participants (n=260) enrolled between January 1, 2015 and December 31, 2018 and who had trauma registry data were included. RxH eligibility criteria: admitted for a violent injury (excluding sexual violence), at least 15 years of age, live in Marion County, Indiana, and stay in the hospital for at least 24 hours. RxH exclusion criteria: heavy active substance use, acute psychosis, dementia, severe traumatic brain injury, intentional self-harm, and incarceration. All patients admitted to IU Health Methodist Hospital, a nearby level I trauma center, for an assault, stabbing, or gunshot wound during the same period and met the RxH eligibility criteria were included as a comparison group (n=732). Doubly adjusted logistic regression with inverse probability of treatment weighting was used to estimate the average treatment effect of RxH participation on violent reinjury and new convictions for violent crime.
Results Data from 992 patients were analyzed. RxH was significantly associated with reduced odds of violent reinjury (OR=0.35, 95% CI 0.20 to 0.59) and increased odds of conviction for a violent crime (OR=2.43, 95% CI 1.64 to 3.61).
Conclusion RxH was associated with decreased odds of violent reinjury but increased odds of new conviction for a violent crime. Our results highlight the importance of robust, routine evaluation of HVIP efficacy and recommend inclusion of other outcomes in addition to violent reinjury when evaluating program success. High-quality randomized controlled trials are needed to further investigate the impact of HVIPs on a variety of outcomes.
Level of evidence IV: retrospective study with more than one negative criterion ((1) limited control of confounding and (2) heterogeneous populations).
- violence
- Community Health Services
- Outcome Assessment, Health Care
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Most studies involving hospital-based violence intervention programs (HVIPs) demonstrate a reduction in violent reinjury, but few have investigated the impact of HVIPs on crime and those that did report mixed results.
WHAT THIS STUDY ADDS
This study suggests that HVIPs may have unmeasured outcomes that should be considered in addition to violent reinjury.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our results highlight the importance of robust, routine evaluation of HVIP efficacy and suggest that it is beneficial to include other outcomes in addition to violent reinjury when evaluating program endpoints and measuring success.
Introduction
Hospital-based violence intervention programs (HVIPs) have been used at trauma centers for over a decade to decrease violent injury and injury recidivism. These programs aim to take advantage of a ‘teachable moment’ after injury, a window of time where patients are particularly receptive to interventions and making positive behavioral changes.1–3 Although HVIP structure varies, the majority include a brief intervention at bedside followed by a period of extended community case management after discharge.3
However, program interventions are variable and few have been rigorously studied to date, leaving questions regarding program efficacy and overall impact.4 Although most studies involving HVIPs show a beneficial effect in reducing violent reinjury, few have investigated the impact of HVIPs on crime and the results have been mixed.5–8 The purpose of this study was to determine if exposure to Prescription for Hope (RxH), an HVIP based out of a level 1 trauma center in Indianapolis, Indiana, USA is related to violent reinjury and new convictions for violent crime in the 2-year period after index hospitalization for a violent injury. We hypothesized that: (1) violently injured patients who participated in RxH would have reduced odds of violent reinjury, and (2) violently injured patients who participated in the RxH program would have reduced odds of conviction for violent crime compared with non-participants.
Methods
Study design, setting, and participants
All patients (n=268) who enrolled in the RxH violence program at Eskenazi Hospital (EH) after hospitalization for an assault, stabbing, or gunshot wound between January 1, 2015 and December 31, 2018 and had trauma registry data were included. EH is the safety net hospital for Marion County, Indiana, and has a high proportion of penetrating injuries. Patients are considered eligible for the RxH program if they are: admitted for a violent injury (excluding self-harm and sexual violence), at least 15 years of age, live in Marion County, Indiana, and stay in the hospital for at least 24 hours. Exclusion criteria include heavy active substance use, acute psychosis, dementia, severe traumatic brain injury, intentional self-harm, active incarceration or in police custody, and an outstanding warrant or pending criminal charges. Heavy active substance use was determined after a violence intervention specialist had several conversations with patients to determine the extent of their drug use and whether it would disrupt their potential participation in the program. The comparison group was composed of patients admitted to IU Health Methodist Hospital (MH), another level I trauma center less than 2 miles from EH that does not have an HVIP, who also met the same criteria (n=780). MH is a high-volume academic center that receives transfers from all over the state. This comparison group was used to mirror the study population as closely as possible and reduce bias, given that the two centers share the same zip code and are cared for by surgeons in the same division of trauma and acute care surgery.
RxH program description
Details of the RxH program have been previously described by Gomez et al.9 Briefly, RxH provides wraparound case management services including: financial assistance, post-injury recovery care, access to health insurance, secure housing, placement with primary care, legal assistance, and employment or education placement. Primary goals for all participants include obtaining health insurance, a primary care provider, a state ID, and transportation to follow up healthcare appointments. Participants set their own goals at the beginning of the program and program completion is defined as meeting all goals. RxH currently employs four violence intervention specialists, one licensed clinical social worker who is trained in cognitive–behavioral therapy and eye movement desensitization and reprocessing, one program manager with a background in public health, and one program coordinator with a background in social work.
Data sources and variables
Demographics and clinical information, including age, sex, race, mechanism of injury, insurance type, intensive care unit (ICU) use, ventilator use, blood administration within 24 hours of hospitalization, systolic blood pressure at arrival, Abbreviated Injury Scale (AIS) scores, alcohol and drug screen results, hospital length of stay, patient address, previous violent injury, and means of transportation to the hospital, were obtained from the hospital trauma registries. Race was categorized as black, white, or other, and insurance was categorized as commercial, government (Medicare or Medicaid), self-pay, or other. RxH participation data were obtained from program records. Emergency department visit, inpatient visit, and death data for the 2-year period after index hospitalization were obtained through the Regenstrief Institute’s Indiana Network for Patient Care (INPC). The INPC receives data from 95% of all hospitals in Indiana including all three level I trauma centers in Indianapolis. Included in the visit dataset were visit date, care setting, reason for visit, diagnosis code (International Classification of Diseases 9th/10th Clinical Modification (ICD-9-CM/ICD-10-CM)), and diagnosis code text. Physician notes were also acquired for each of the visits when available. The national Area Deprivation Index (ADI) percentile for each patient was obtained using the Neighborhood Atlas, which is available for free at University of Wisconsin School of Medicine and Public Health’s Neighborhood Atlas website (https://www.neighborhoodatlas.medicine.wisc.edu). The ADI is a validated composite measure of neighborhood disadvantage based on domains of income, education, employment, and housing quality at the census block group level.10 Cohort characteristics comparing RxH participants at EH and non-participants at MH are displayed in table 1.
Cohort characteristics at index hospitalization for violent injury
Crime data were manually extracted from Indiana MyCase, a publicly available database that allows the lookup of non-confidential court cases filed within the state. History of violent crime was defined as having at least one conviction for a violent crime anytime before the index hospitalization date. Crimes were considered violent if they involved intentionally harming another person, including the use of or threatening the use of a deadly weapon. Specifically, violent crimes were categorized as: battery, murder, criminal recklessness committed with a deadly weapon, criminal confinement, kidnapping, armed robbery, intimidation where threat is to commit a forcible felony, disorderly conduct with physical altercation, reckless homicide, resisting law enforcement and draws deadly weapon, and strangulation. Table 2 compares characteristics between those who were convicted of a new violent crime during the study period and those who were not.
Cohort characteristics by new conviction for a violent crime
The primary exposure of interest was enrollment and participation in the RxH program during the study period. The primary outcome of interest was new violent injury, defined as having an emergency department or inpatient visit due to being shot, stabbed, or assaulted within 2 years after index hospitalization. New violent injuries were identified using a prespecified set of ICD-9-CM and ICD-10-CM codes and then confirmed via manual review of physician notes. The 146 patients (28 RxH and 118 non-RxH patients) without any INPC visit data were assumed to not have had a violent injury during the study period. The secondary outcome of interest was violent crime, which was defined as being convicted of a new violent crime within 2 years after index hospitalization. Table 3 shows differences between those who were reinjured during the study period and those who were not.
Cohort characteristics by violent reinjury
Statistical analysis
Descriptive statistics were expressed as means and SDs for normally distributed continuous variables, medians and IQRs for non-normally distributed continuous variables, and frequencies and percentages for categorical variables. Demographic and injury characteristics were compared using Χ2, t-test and Kruskal-Wallis tests. All participants with missing data were excluded from the analysis; this composed of less than 5% of the sample. Inverse probability of treatment weighting (IPTW) was used to estimate effect of the RxH program on violent reinjury and new conviction for a violent crime after initial hospitalization. IPTW is a propensity score-based approach that aims to approximate randomization by creating a pseudopopulation where the distributions of observed covariates are balanced across the treated and untreated populations. Propensity scores and corresponding IPTWs were generated using the following variables11: age, sex, race, mechanism of injury, insurance type, ICU (binary), ventilator use (binary), received blood within the first 24 hours of hospital stay (binary), hypotension at arrival (binary), head AIS score, thorax AIS score, abdomen AIS score, alcohol screen positivity (binary), drug screen positivity (binary), hospital length of stay, zip code group (zip codes were clustered into nine groups based on geographic location), means of transportation to the hospital (ambulance or other), national ADI percentile, history of violent injury (binary), emergency medical service (EMS) provider (if transported to hospital by ambulance), and history of violent crime (binary). Age, sex, race, alcohol screen results, drug screen results, history of violent injury, history of violent crime, national ADI percentile (as a proxy for socioeconomic status) and insurance status (as a proxy for socioeconomic status) were included in the propensity score model because they are associated with risk of violent injury.2 5 6 12 13 EMS provider was included to account for potential bias in which patients are taken to which hospital. The remaining clinical variables were included because they are related to the likelihood of being approached to participate in RxH. The resulting propensity scores were highly predictive of RxH (area under the curve=0.910). Covariate balance in the IPTW sample was evaluated using standardized mean differences (SMDs) and variance ratios. To address any residual imbalance, we fitted doubly adjusted logistic regressions using both IPTW and adjustment for any covariates with weighted SMDs and/or variance ratios outside of the recommended limits (SMD: −0.2 to 0.2; variance ratios: 0.5–2.0) (online supplemental table 1). Two separate doubly adjusted IPTW logistic regression analyses were performed to estimate the effect of RxH participation on violent reinjury and new conviction for a violent crime, respectively (online supplemental table 2). Adjusted ORs and 95% CIs were calculated. All analyses were performed using SAS V.9.4 (SAS Institute) and two-sided p values of <0.05 were considered statistically significant.
Supplemental material
Results
Demographics and clinical characteristics
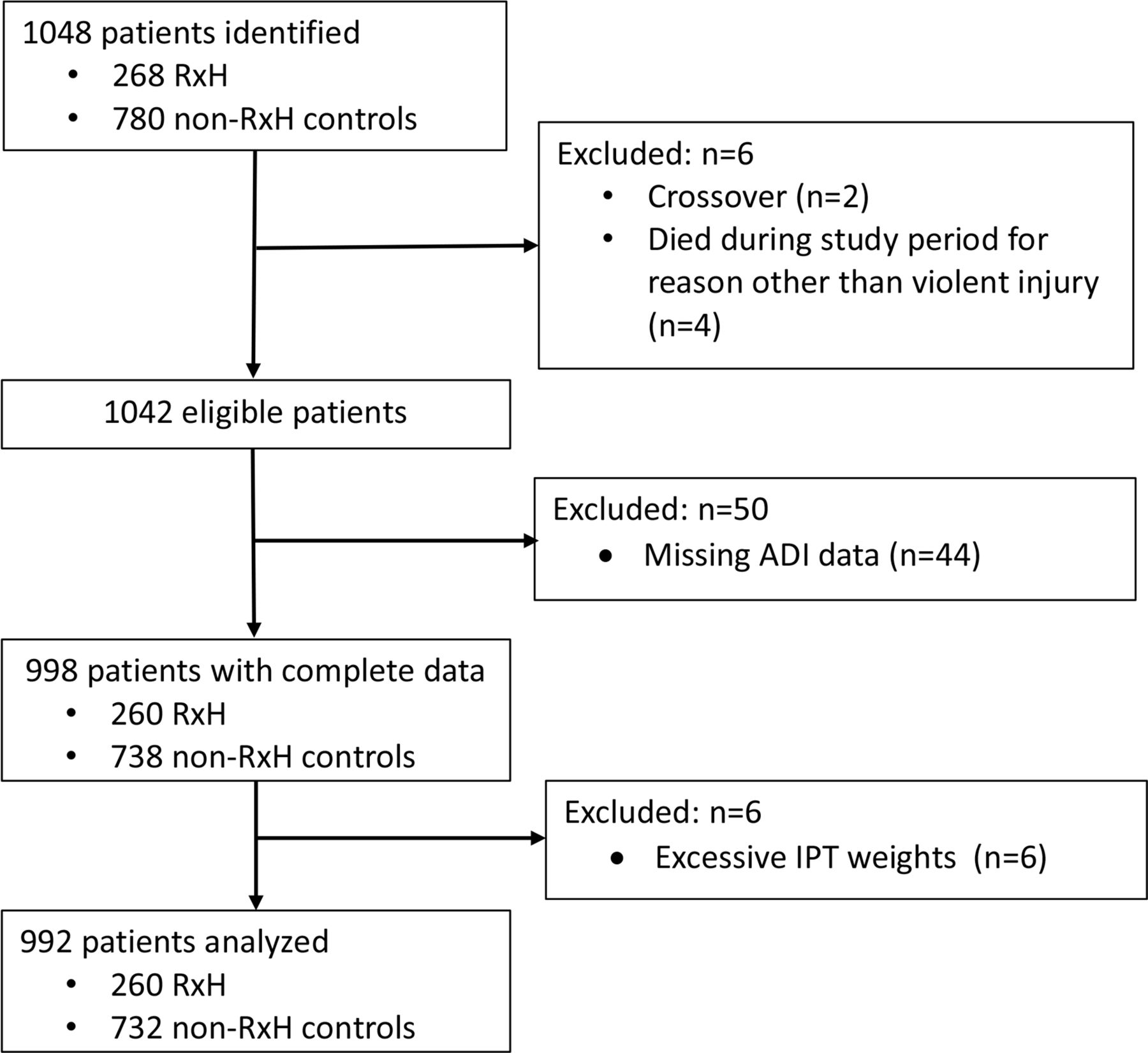
Of 1048 eligible patients, 2 were excluded for having crossover (participated in RxH and were also admitted to MH for violent injury during the study period) and 6 were excluded due to death from non-violent injury. The two patients who died of violent reinjury within the study period were included. Forty-four patients (4.2%) had missing ADI information (either due to homelessness or incomplete data entry) and were excluded from the regression analysis. In total, the final sample included 998 patients (RxH=260, non-RxH=738) (figure 1). The median patient age was 28 years (IQR 23–38). Patients were predominantly male (83%), black (67%), and insured through the government (Medicare or Medicaid, 45%). The most common mechanism of injury at index hospitalization was gunshot wound (55%) followed by assault (29%). Approximately one-quarter of patients screened positive for alcohol at admission (26%) and half screened positive for illicit drugs (50%). The median national ADI percentile (continuous) was 90 (IQR 75–96). Higher ADI percentile signifies increasing neighborhood adversity ranging from 0 to 100. Of the 260 RxH participants, 61 (23.6%) completed the program.

Flow diagram of derivation of analysis cohort. Out of 1048 patients identified, 992 were analyzed. ADI, Area Deprivation Index; IPT, inverse probability of treatment; RxH, Prescription for Hope.
Violent reinjury and criminal recidivism
In total, 77 patients (8%) had a new violent injury during the 2-year period after index hospitalization. Of those, 12 were RxH participants and 65 were non-participants. Most patients (86%) did not have a history of violent crime convictions prior to their injury. RxH participants had slightly more prior convictions for violent crimes. Sixty-five patients (7%) were convicted of a new violent crime within the 2-year study period, including 28 RxH participants and 37 non-participants.
Regression analyses
After generating propensity scores and performing the IPTW procedure, six observations with excessively large weights (defined as IPTW greater than 10 times the expected value) were excluded; in total, 992 patients were analyzed (figure 1). Drug use, alcohol use, and ICU admission had SMDs greater than the recommended limit 0.2, so they were included in the IPTW logistic regressions to eliminate any residual differences. RxH participation was significantly associated with reduced odds of violent reinjury (OR=0.35, 95% CI 0.20 to 0.59). RxH participation was also associated with increased odds of a new conviction for violent crime (OR=2.43, 95% CI 1.64 to 3.61) (figure 2).

{kind=link}
{kind=link}
Prescription for Hope (RxH) participation: ORs and 95% CIs for violent reinjury and violent crime. Figure 2 is a graphic depiction of RxH participation association with violent reinjury and violent crime. RxH participation was significantly associated with reduced odds of violent reinjury (OR=0.35, 95% CI 0.20 to 0.59) and was also associated with increased odds of a new conviction for violent crime (OR=2.43, 95% CI 1.64 to 3.61).
Sensitivity analysis
Limiting the cohort to only patients who completed RxH and non-RxH controls resulted in a sample of 799 patients (RxH=61, non-RxH=738). None of the observations had excessively large weights so all 799 patients were analyzed. After completing the weighting procedure, race, insurance, ICU admission, mechanism of injury, hospital length of stay, and drug use had SMDs greater than the recommended value of 0.2 and were included in the logistic regressions to account for any residual differences. In the sensitivity analysis, RxH completion was significantly associated with decreased odds of violent reinjury (OR=0.33, 95% CI 0.14 to 0.76) and increased odds of conviction for a new violent crime (OR=8.73, 95% CI 4.70 to 16.24).
Discussion
Participation in the HVIP RxH was associated with approximately half the rate of violent reinjury. Surprisingly, it was also associated with over twice the odds of being convicted for a new violent crime during the 2-year period after the index hospitalization. These findings support our first hypothesis but refute the second. Additionally, the results of the exploratory sensitivity analysis of patients who completed the RxH program were consistent with our main analysis.
This study represents the third evaluation of RxH and was the first attempt to investigate the efficacy of the program by comparing RxH participants with controls. The previous studies reported an association between RxH and reduction of violent reinjury; in the first year after establishing the RxH program, Gomez et al reported a 1-year violent reinjury rate of 2.9% for 516 program participants using institutional data.9 This was compared with a historical institutional 5-year violent reinjury rate of 31%. Bell et al later reported an 8-year recidivism rate of 4.4% using statewide INPC data, suggesting sustained positive effects of the program over time.14 The present study, which also used INPC data, similarly found that RxH participants had a 2-year violent reinjury rate of 4.5%.
The current literature on HVIP efficacy is limited and difficult to compare due to heterogeneity of interventions. Published randomized controlled trials (RCTs) regarding adult HVIP exist, but most have significant flaws in study design, significant loss to follow-up, and/or insufficient description of methodology.5 7 8 The most rigorous is likely Cooper et al, which evaluated the HVIP at the R Adam Cowley Shock Trauma Center in Baltimore, Maryland with an RCT comparing program participants with non-participants. They found a similar reduction in violent reinjury to our program results: the intervention group had a 5% recidivism rate compared with 36% in the control group.6 However, a similar RCT by Snider et al on their HVIP for youth did not find a statistically significant difference in violent reinjury between participants and non-participants.7
The majority of HVIPs, including RxH, use reduction in violent reinjury as the main measure of program success.5–8 This is also often a grant funding requirement for HVIP. As such, most studies evaluating HVIP have used violent reinjury as the outcome of interest. Using this metric, RxH is a successful HVIP. However, other factors should be considered when evaluating an HVIP. For example, this is the first time new violent crime has been considered as an outcome when evaluating RxH. The association between RxH participation and violent crime was surprising, and we were unable to find any similar results in the literature. This finding could be potentially explained by unmeasured confounders, including differences in social environment and non-normative social involvement, such as gang activity, between the Methodist and Eskenazi patient samples. Patients injured by a penetrating mechanism who were taken to EH, which is a safety net hospital, may have been injured under different circumstances than patients taken to MH. Eskenazi patients may experience more pressure to retaliate from their communities, resulting in the observed differences in violent crime convictions. The literature suggests that youths living in high-crime, high-poverty areas may think that responding to provocation with violence is necessary to protect their reputation and prevent future conflict.15 Furthermore, youths exposed to violence are twice as likely to perpetrate violence within 2 years.2 Property and violent crimes have also been shown to rise in populations where individuals do not have strong social bonds, specifically, engagement in schooling, employment, or community organizations.16 We did not include these factors in our analysis. Alternatively, violently injured patients who present to Eskenazi may already be on a trajectory toward a life of violent crime. The Age–Crime Curve (ACC) phenomenon observes crime rates that rise during adolescence, peak in the mid to late 20s and then decline with age.17 There has been more recent study on the variability of this curve based on individual factors.16 18 19 Based on available data, many violent crimes appear to follow the classic ACC.17 The median age in our study was 28 years overall, 24.5 years for program participants, and 30 years for non-participants. The age for program participants corresponds with the peak years of violent criminal activity whereas non-participants may already be on the natural gradual decline and therefore already less likely to commit a violent crime in the subsequent 2 years.
The few RCTs that did evaluate the impact of HVIP on crime report either no difference or reduced violent crime convictions among program participants.5 6 8 Cooper et al found that patients in the control group were 2.2 times more likely to be convicted of any crime and 4.4 times more likely to be convicted of a violent crime compared with HVIP participants.6 It is worth noting that the program had substantial resources dedicated to crime prevention and RxH does not. Until now, RxH’s program scope has focused on individual social determinants of health and assistance with injury recovery. Other studies have not supported crime reduction associated with HVIP participation. Aboutanos et al reported that 5% of HVIP participants were convicted of a crime 6 months after injury compared with 11% of controls, but statistical significance was not addressed.5 Zun et al found no significant differences in the number of arrests and convictions between HVIP participants and non-participants.8
The low RxH program completion rate was a limitation in determining if program completion would affect our primary outcomes. The lack of power due to small sample size made the analysis vulnerable to type II error or not detecting a significant difference. However, our sensitivity analysis using only the group that completed the program supported our initial results. It is more likely that an unobserved difference between groups explains the increased violent crime convictions rather than it being an unintended consequence of the HVIP itself. Factors such as juvenile criminal history, attitude changes after injury, and stressors from injury, including hospital expenses, were also not examined.20 21
The unexpected finding of our HVIP association with increased violent crime convictions, as well as other recent work, leads us to conclude that leveraging other secondary outcomes to measure the success of HVIP is critical to fully evaluate a program’s efficacy. To this end, Monopoli et al used a two-stage Delphi method with service delivery practitioners to identify core HVIP outcomes. Post-traumatic stress, beliefs about violence and aggression, coping strategies and emotional regulation were the outcomes prioritized by respondents.21 A 2013 RCT used the Attitudes Towards Guns and Violence Questionnaire as the primary outcome and demonstrated a 50% reduction in aggressive response to shame, a 29% reduction in comfort with aggression, and a 19% reduction in overall inclination toward violence among HVIP participants.22 These results are important because they suggest that HVIPs can positively influence social factors associated with repeated violence. Despite their importance in the Social–Ecological Model for violence prevention, these socioemotional and behavioral health outcomes are not consistently or rigorously studied in HVIP literature.23 24 Although reducing violent reinjury and violent crime is an important endpoint for HVIPs, it does not give a complete picture of the program’s potential effects. In addition to considering other outcomes, it will be important to identify the effective ‘dose’ of HVIP interventions as well as the specific program services that provide the most benefit to optimize use of resources.25
Strengths and limitations
To our knowledge, this is the largest study investigating HVIP efficacy. We were able to use data from a statewide health information exchange, which allows for the capture of nearly all instances of violent reinjury regardless of where a patient chose to seek care. In addition to capturing violent crime convictions, we were able to look up history of violent crime for each patient and include it as a variable when generating propensity scores. This analysis also used double adjustment for baseline covariates to reduce residual confounding and ensure observed covariate balance between the treated (RxH) and non-treated (non-RxH controls) groups.
This study has important limitations. RxH data collection and storage have been inconsistent over the years, so we were unable to determine which or how many patients were approached for enrollment in the program. Due to this challenge, we elected to use similar patients from a nearby level I trauma center as controls. We attempted to mitigate differences between RxH participants and controls by balancing the analysis sample across a large set of clinical and sociodemographic variables using both IPTW and covariate adjustment. It is important to note that propensity score-based methods only balance groups across known confounders; although we included important sociodemographic variables, there is still the possibility that unmeasured confounding exists. This would be best addressed by performing an RCT. Because RxH did not collect information related to social or emotional recovery, we were unable to assess the impact of RxH on those factors in this study. We are including metrics to capture that information in the update of the program so they can be assessed in future studies. Also, the Indiana MyCase Database only has information on non-confidential court cases; cases relating to juvenile delinquency (children under the age of 18 years) are not available. Due to this, it is possible that violent crimes were underestimated. Because the study was limited to a single HVIP serving patients in Marion County, Indiana, the results may not generalize to all HVIPs. Finally, the present study was not designed to determine which components of RxH are most important for reducing violent reinjury.
Future directions
Future directions for our program will include improving data management strategies, incorporating validated assessments for socioemotional and behavioral health outcomes, qualitative data gathering, and design of an RCT to evaluate the updated HVIP.
Conclusions
Participation in the RxH HVIP was associated with decreased odds of violent reinjury but increased odds of conviction for a violent crime in the 2 years after hospitalization. Our results highlight the importance of robust, routine evaluation of HVIP efficacy and suggest that it is beneficial to include other outcomes in addition to violent reinjury when evaluating program endpoints and measuring success. High-quality RCTs are needed to further investigate the impact of HVIPs on a variety of outcomes. Finally, our results suggest that violent injury prevention does not equate to violent crime prevention.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This retrospective cohort study was approved by the Institutional Review Board of Indiana University and a waiver of consent was obtained (protocol #2003937741).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DO, EH, and CJS conceived and designed the study. EH, BLZ, and DO analyzed and interpreted the data. EH and DO drafted the initial manuscript and all authors critically revised and approved the final version. EH and BLZ had full access to all the data in the study, accept full responsibility for the work and conduct of the study, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.