Article Text

Abstract
Objectives Gallstone disease is a common reason for emergency department (ED) presentation. Surgeons often prefer radiology department ultrasound (RUS) over point of care ultrasound (POCUS) because of perceived of unreliability. Our study was designed to test the hypothesis that POCUS is sufficient to guide the management of surgeons treating select cases of biliary disease as compared to RUS.
Methods This was a prospective cohort study. Patients who presented to the ED with abdominal pain and findings of biliary disease on POCUS were included. The surgeon was then presented the case with POCUS only and recorded their management decision. Patients then proceeded to RUS, were followed through their stay, and analysis was performed to analyze the proportion of patients where the introduction of the RUS changed the management plan.
Results 100 patients were included in this study, and all received both POCUS and RUS. Depending on the surgeons’ POCUS based management decisions, the patients were divided into three groups: (1) surgery, (2) duct clearance, (3) no surgery. Total bilirubin was 34±22 mmol/L in the duct clearance group vs 8.4±6.5 mmol/L and 16±12 mmol/L in the surgery and no surgery groups, respectively (p<0.05). POCUS results showed 68 patients would have been offered surgery, 21 offered duct clearance, and 11 no surgery. In 90% of cases, the introduction of RUS did not change management. The acute care surgeons elected to operate on patients more frequently than other surgical subspecialties (p<0.05).
Conclusions This study showed that fewer than 10% of patients with biliary disease seen on POCUS had a change in surgical decision-making based on the addition of RUS imaging. In uncomplicated cases of biliary disease, relying on POCUS imaging for surgical decision-making has the potential to improve patient flow.
Level of evidence II Prospective Cohort Study.
- patients
- surgeons
- management
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Point of care ultrasound for biliary disease has similar sensitivity and specificity to radiology department ultrasounds; however, medicolegal concerns and concerns about reliability of results are barriers to its adoption for surgical decision-making.
WHAT THIS STUDY ADDS
When biliary point of care ultrasound is performed by trained emergency medicine physicians, the additional step of adding a formal radiology department ultrasound adds minimal additional value to the surgeons making a clinical decision.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This demonstrates that surgical decision-making for uncomplicated biliary disease can safely proceed based on emergency department point of care ultrasound without the use of comprehensive radiology department imaging.
Introduction
Biliary disease is common, affecting more than 20 million Americans annually.1 It frequently results in emergency department (ED) presentation and admission for surgery. Point-of-care ultrasound (POCUS) in the ED has seen growing use in the diagnosis and management of gallbladder disease.2–4 The diagnostic accuracy of biliary POCUS has been previously evaluated in multiple studies. Compared with history, physical examination, and laboratory tests, biliary POCUS is the best performing bedside test for acute biliary disease.5 6 When compared with radiology department ultrasound (RUS), systematic reviews have demonstrated that the sensitivity of POCUS for cholelithiasis was 89.8% and the specificity was 88.0%.7 Implementation of POCUS can improve access to care, and more emergency medicine physicians are being trained in biliary POCUS.8 Patients who have biliary disease diagnosed by POCUS, and are managed without confirmatory imaging, have on average a 2-hour shorter length of stay in the ED.9–11 Despite the literature demonstrating reliability and potential benefits of biliary POCUS, there has been a lack of adoption for the purpose of surgical decision-making.12 A recent Canadian national survey showed that 60% of practicing surgeons had a total lack of confidence in ED POCUS for the diagnosis of biliary disease.13 This lack of confidence leads many surgeons to seek confirmatory radiology department imaging prior to operating on the gallbladder. The unanswered question is whether this additional step of obtaining a RUS adds value for the surgeon over the information available by POCUS. This study attempts to answer this question by prospectively evaluating the surgical decision-making for a cohort of patients who were diagnosed with acute biliary disease on POCUS in the ED. We compared the decisions surgeons would have made in the management of their patients if (i) POCUS had been the only imaging available, to (ii) their final management plan knowing the results of confirmatory radiology department imaging.
Methods
A prospective cohort study was performed in a university affiliated tertiary care center (London Health Sciences Centre, in London, Ontario, Canada). This facility has a fellowship training program for emergency medicine physicians in POCUS. The POCUS images and interpretations were performed by emergency medicine attendings within this fellowship program. There are a total of 11 faculty members participating in the ED fellowship POCUS program. Each of these ED faculty members have training and experience specific to biliary POCUS and incorporate it into their clinical practice. Patients presenting with abdominal pain were consecutively evaluated for the possibility of acute biliary disease. When clinically indicated and as part of routine care, abdominal POCUS with gallbladder assessment was performed. Point of care ultrasound images were recorded using a commercially available cloud-based system (Qpath, Telexy Healthcare, Everett, WA). The emergency physician then interpreted the POCUS findings and published them to the electronic medical record for permanent reference and review. Patients were approached for inclusion in the study if the ED physician felt that the ultrasound findings, physical examination, and history were consistent with biliary disease, and their age was equal to or greater than 18. Patients were excluded if they underwent emergency surgery prior to a confirmatory ultrasound or were unable to understand or offer consent to this study. At this institution, surgeons from all subspecialities take emergency general surgery call and are responsible for managing acute biliary pathology. For the purposes of secondary analysis, these surgeons were grouped into five subspeciality categories: acute care/trauma (ACS) surgeons, colorectal surgeons, hepatobiliary (HPB) surgeons, surgical oncologists, and minimally invasive/bariatric (MIS) surgeons. After the patient was approached and informed written consent was obtained, they were then referred to general surgery and a RUS was arranged, as is the usual care. The general surgeon then assessed the patient and was asked to make a clinical decision based on history, physical, available lab work and POCUS. This was entered electronically and was stored on an institutionally maintained research database system (REDCap). After this decision was recorded, the patient then proceeded to the radiology department for an ultrasound performed by an ultrasound technologist and interpreted by a radiologist, the results of which were relayed to the surgeon who then proceeded with management. If for some reason the formal RUS was performed prior to the general surgeon evaluating the patient, the surgeon was blinded to the results of the RUS until their POCUS based management decision was obtained and recorded. Patients were followed through their course in hospital, and the actual final management for each patient served as the comparator to the POCUS based management decision previously recorded in REDCap. The pathway of the patients recruited is shown in figure 1. The primary outcome of this study was the percent change in management decisions after introduction of a RUS. Secondary outcomes included an evaluation of the clinical decisions based on surgeon subspecialty, biochemical markers, vital signs, and patient demographics.

Patient pathway. ED, emergency department; POCUS, point of care ultrasound; US, ultrasound.
Statistical analysis was performed using Matlab r2021a (The Mathworks, Natick, MA). Data are presented as mean±SD. Comparison between the three groups was done using one-way analysis of variance with Tukey Honestly Significant Difference (HSD) correction. Comparison between the proportion of times each subspecialty chose to operate versus not operate was done using a χ² test with Tukey HSD posthoc testing for proportions. P<0.05 was considered statistically significant.
Results
Patient recruitment
We recruited 103 patients to the study, of which 100 were included. Three patients were excluded because the management plan form was filled out incorrectly by the consulting surgeon and the intended management plan could not be analyzed. Demographic information as well as triage vital signs and bloodwork is shown in table 1. All patients underwent both POCUS and RUS studies. The patients were divided into three groups (surgery, duct clearance, and no surgery) based on the POCUS based clinical decision recorded by the surgeons. These three groups were similar in all criteria except for total bilirubin. Total bilirubin was 8.4±6.5 µmol/L in the surgery group, 34±22 µmol/L in the duct clearance group, and 16±12 µmol/L in the no surgery group (p=1.12×10−12). The total bilirubin at admission to hospital for all patients is shown in figure 2.
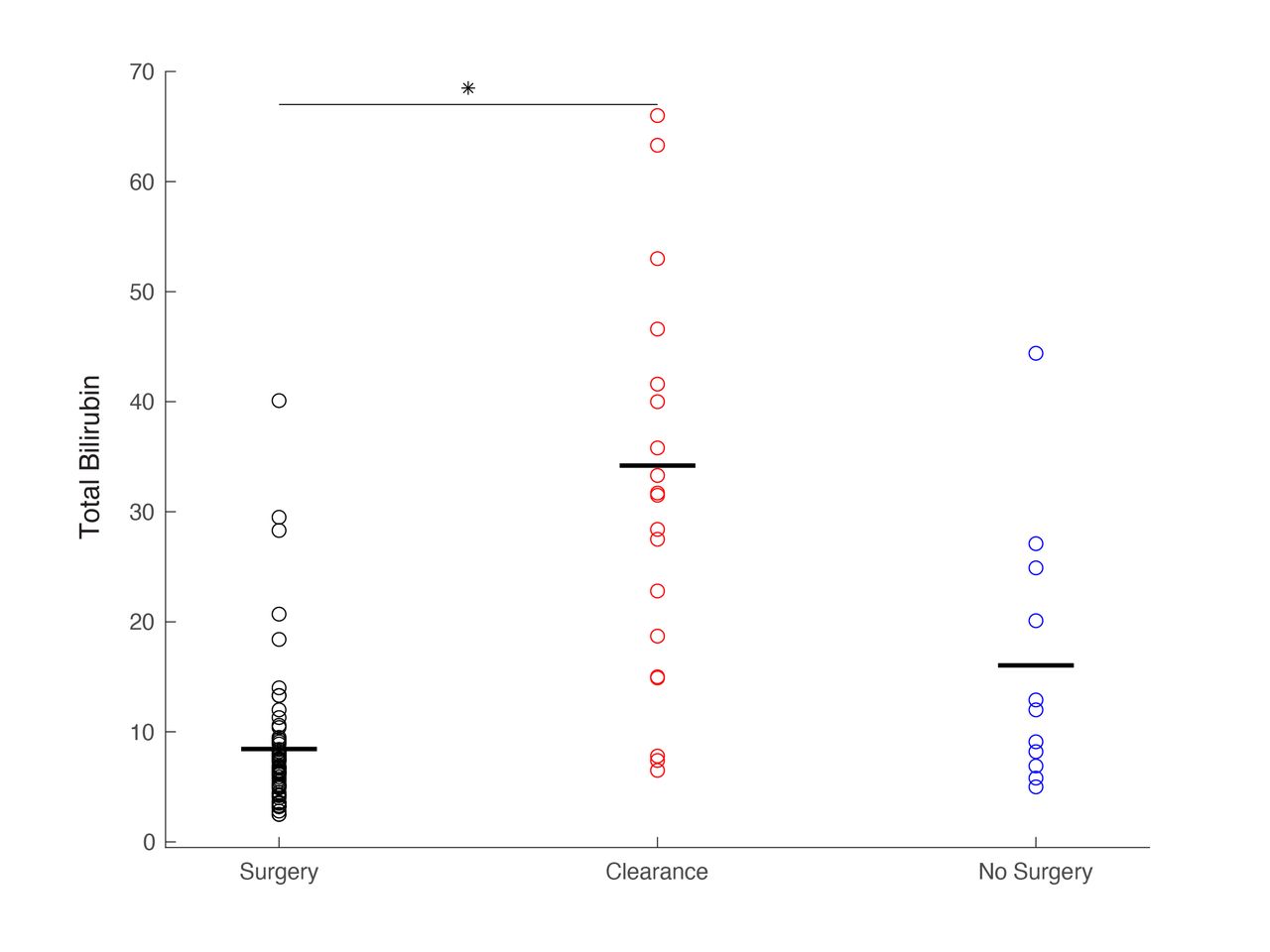
Total bilirubin by group.
Baseline characteristics
Surgeon decisions and response to radiology ultrasound
Twenty surgeons participated in the study. They are composed of a range of subspecialties including acute care surgery (six), colorectal (four), HPB (four), surgical oncology (three), and MIS/bariatric (three). Their POCUS based management plans are shown in table 2. Based on the ED POCUS, 68 patients would have been offered surgery, 21 offered Endoscopic Retrograde Cholangiopancreatography (ERCP) or Magnetic resonance cholangiopancreatography (MRCP) grouped as (duct clearance), and 11 would not have been offered surgery.
Grouping of survey responses
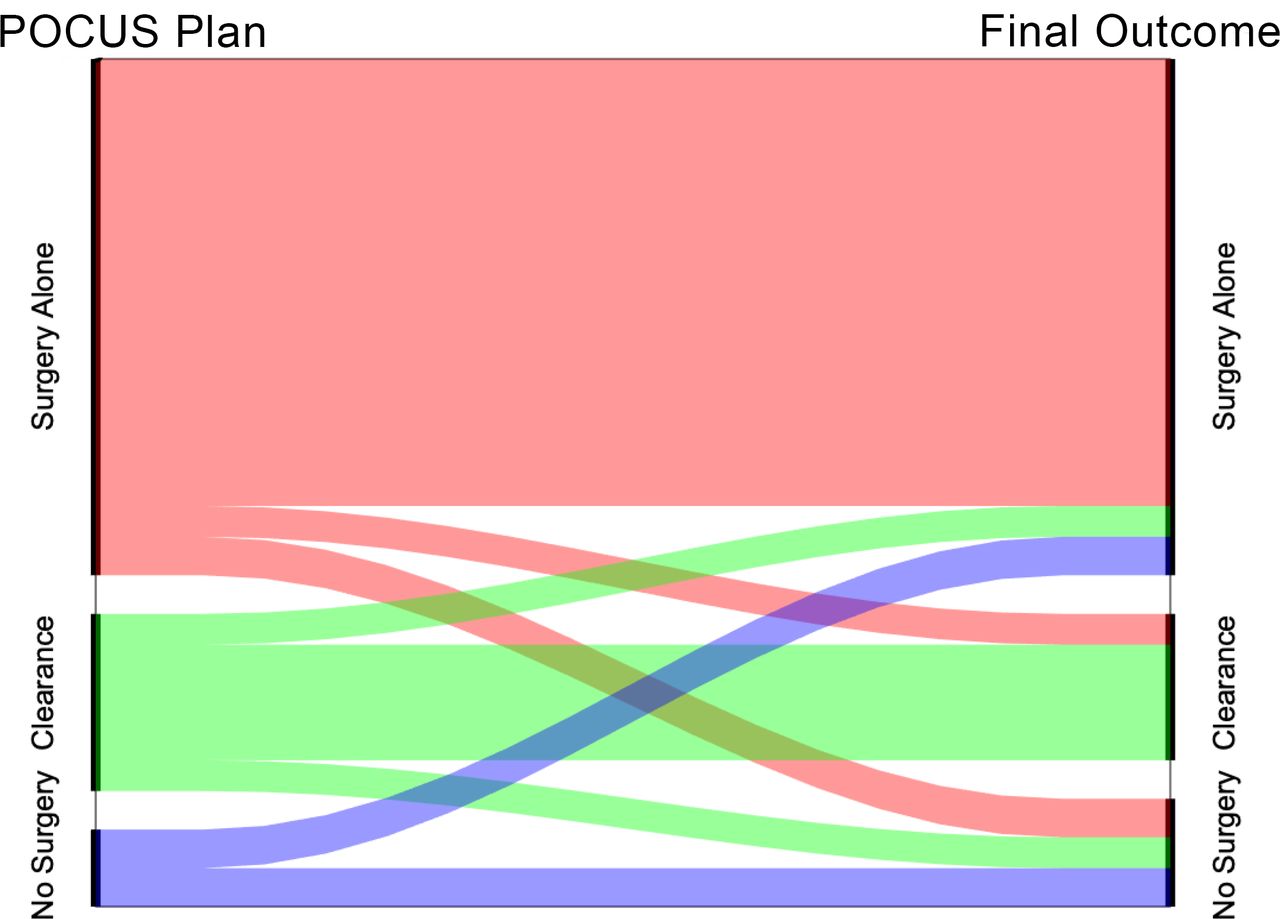
Of the 100 patients included in the study, the initial plan based on the ED POCUS was changed after the radiology ultrasound results a total of 10 times. The pathway of patients between the POCUS based clinical decision to their eventual outcome after RUS is shown in the alluvial diagram in figure 3. The left-hand side of the figure shows the POCUS based clinical decision, and the right-hand side shows the eventual outcome for each patient. The pink bars represent patients who would have been offered surgery, and the thickness of the bars represents the number of patients. Green bars represent those patients who would have undergone ERCP or MRCP. Blue bars represent patients who would not have been offered surgery. The figure reflects that 90% of the patients in the study did not have a change to their plan after the RUS was added.

Decision-making alluvial diagram.
The patients whose plan was changed during their clinical course in hospital are shown in table 3. One of these patients required an ERCP prior to surgery because of presence of a common bile duct (CBD) stone identified on RUS. Two patients would have been sent for ERCP based on POCUS alone, but this plan was changed to surgery because the RUS demonstrated a normal diameter bile duct. In these cases, the common bile duct was not visualized on the POCUS. Two patients would have been offered surgery, but their bilirubin increased after imaging was completed, necessitating duct clearance prior to surgery. Neither of these patients had choledocholithiasis after final duct clearance imaging. One patient had a change of diagnosis from cholelithiasis to gastroesophageal reflux (RUS did demonstrate gallstones in agreement with the POCUS results). One patient was offered surgery but chose not to proceed because their symptoms resolved. One patient was discharged home after a normal hepatobiliary iminodiacetic acid (HIDA) scan. One patient required an ERCP after the RUS identified a dilatated common bile duct that had not been visualized on POCUS. Finally, one patient had a plan for non-operative management but proceeded to surgery after their bilirubin normalized during the admission.
Changes in management
Surgeon subspecialty
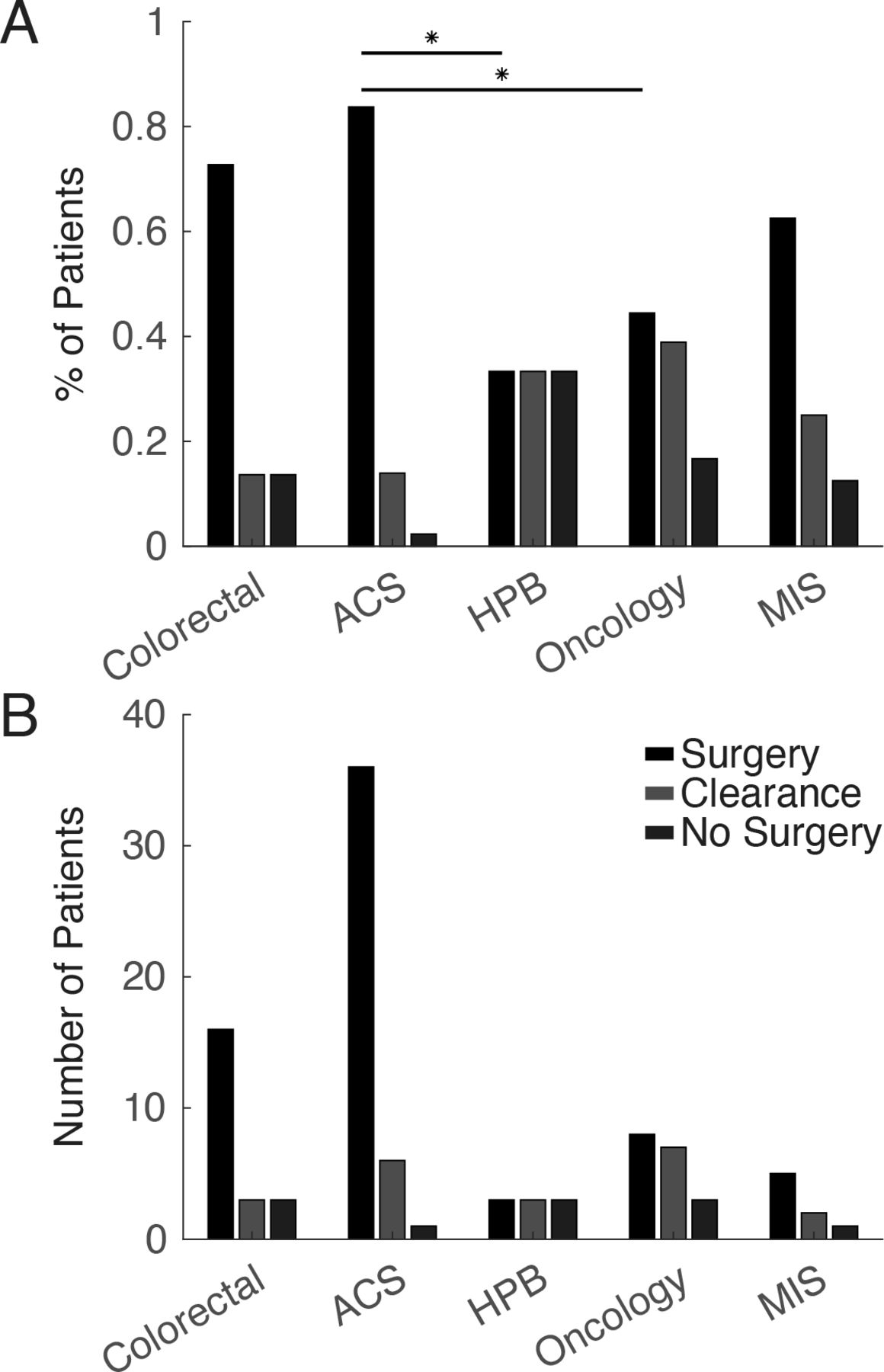
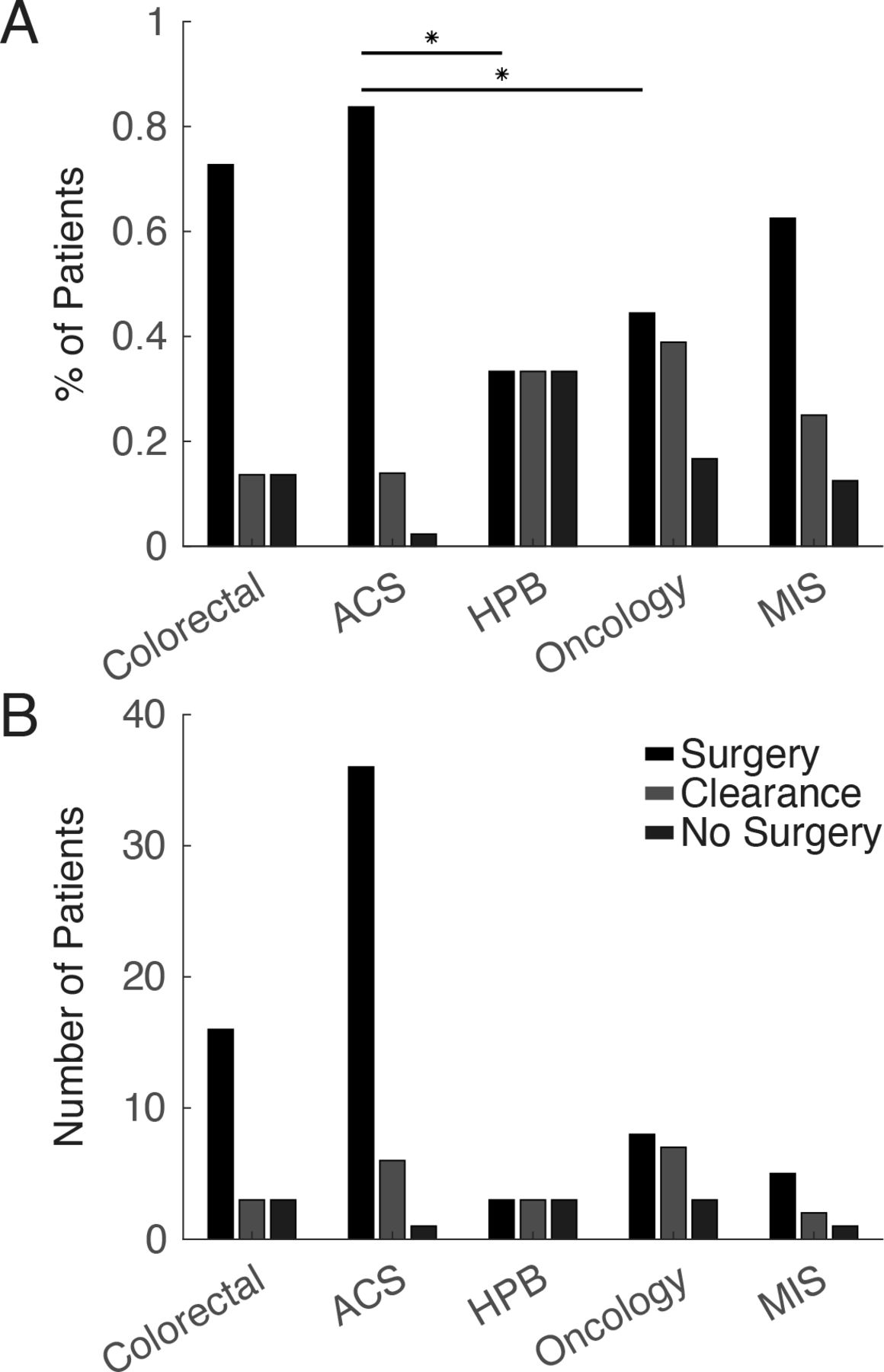
Surgeons were grouped based on subspecialty for secondary analysis on group consensus as practice patterns may differ. ACS surgeons managed 43 patients, colorectal surgeons managed 22 patients, surgical oncologists managed 18, HPB surgeons managed 9, and MIS surgeons managed 8. The decisions of these surgeons based on ED ultrasound are shown in figure 4. Subpanel A shows the number of patients normalized to the total number of patients managed by each subspecialty. This was done to account for the difference in total numbers of patients seen by each group. Subpanel B shows the raw number of patients each surgeon saw and what their survey decisions were. The ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties (p=0.0131). Additionally, the ACS surgeons would have sent only 6 of 43 patients for ERCP or MRCP (14% of patients) whereas surgical oncologists would have sent a higher percentage of patients for ERCP or MRCP (7 out of 18 or 38.9% of patients).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Percent patient by surgical subspecialty. (B) Raw numbers by surgical subspecialty. ACS, acute care/trauma; HPB, hepatobiliary surgeons; MIS, minimally invasive surgeons.
Discussion
This prospective study of patients presenting to the ED demonstrates that in 90% of cases, biliary POCUS provides information sufficient to guide surgical decision-making. Furthermore, among patients that did have a clinical plan change after RUS, only one patient had a missed common bile duct stone. In another case, radiology department imaging demonstrated a dilated common bile duct not seen on POCUS; however, subsequent ERCP showed no choledocholithiasis. In all other cases, it appears that the outcome was not impacted by the additional information provided by a RUS. In most of these cases (table 3), the patient’s clinical status changed between the POCUS and the radiology department imaging. It was this clinical change that appeared to drive the shift in decision-making by the surgeons. Therefore, a change in clinical course resulting from a discrepancy between POCUS and radiology department imaging occurred in only 2% of patients.
These results further support the growing literature that in appropriate clinical settings biliary POCUS can be used for surgical decision-making in the absence of confirmatory imaging.9 The use of POCUS to guide surgical decisions in the absence of radiology department imaging is not new. Focused assessment by sonography for trauma was the first real-world case and is now the standard of care displacing diagnostic peritoneal lavage in the hemodynamically unstable blunt trauma patient.14 15 Previous research from our group went further and looked at the positive predictive value of point of care ultrasound findings in the ED and found that more than 50% of patients presenting with abdominal pain and gallstones ultimately went on to have an operation.9
What makes this article unique is that for the first time we focused specifically on surgical decision-making. We asked what choice a surgeon would make for a given patient if the POCUS was the only ultrasound available to them, then compared that choice to their actual management once all the information was available. In 90% of cases, the ultimate management was the same as the management based on the point of care ultrasound. In only 2% of the cases was this change clinically relevant and based on the addition of RUS.
Hesitation to use point of care ultrasound to guide surgical decision-making seems to come from many sources. Lack of confidence in the accuracy of POCUS and its ability to provide the requisite information seems to be chief among these concerns, despite the literature demonstrating that POCUS is reliable.13 In jurisdictions such as the USA, concerns over medicolegal risk and/or financial incentives may be a barrier to adoption of POCUS for surgical decision-making. The research presented in this article suggests that the subspecialty of the surgeon managing the patient may have an influence. Acute care surgeons were more likely to operate based on the findings from the point of care ultrasound and surgeons from surgical oncology more likely to seek advanced imaging to rule out complicating factors or an alternative diagnosis. Bilirubin levels also represent an important factor in surgeons decision-making. As expected, elevated bilirubin levels were associated with the surgeon choosing to proceed with advanced imaging prior to surgery.
This research focused on surgical decision-making. As a result, there are several potential limitations to this study. The surgeons were aware that they were reviewing a POCUS report. In some cases, the preconceived biases of the reviewing surgeons may have influenced their decision-making, and the difference in choices made by acute care surgeons and surgical oncologists may be partially explained by this. In addition, the emergency medicine physicians participating in this study were fellowship trained in point of care ultrasound and this hospital system allowed the results of the point of care ultrasound to be reported by the emergency medicine physicians and entered permanently as part of the electronic medical record. This permanent record serves the purpose of quality assurance, the absence of which at other institutions, may potentially limit the generalizability of the results of this study.16 Finally, patients were included in this study if the emergency medicine physician clinically felt they likely had acute biliary disease and their POCUS findings supported that diagnosis. These patients would be similar to the types of patients a surgeon could expect to be referred if POCUS was routinely used at their facility for the diagnosis of biliary disease.
Supplemental material
Conclusion
This prospective study has shown that in the vast majority of cases the additional information afforded by formal RUS does not alter clinical management. Point of care biliary ultrasound has been demonstrated to be reliable in the diagnosis of acute biliary disease and offers a safe and efficient diagnostic pathway for patients presenting in the emergency room.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Western University Research Ethics Board (ID 111808). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors participated actively in this study and attest to accuracy of the results presented. Specific contributions are as follows. Study design: RH, RL, DT, FM. Data collection: RH, RL, DT, FM. Data analysis: RH, NM, JH, RL, DT, FM. Data interpretation: RH, NM, JH, RL, DT, FM. Writing: RH, NM, FM. Critical review: RH, NM, JH, RL, DT, FM. Guarantor: RH.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.