Article Text

Abstract
Objectives Trauma-induced hemorrhagic shock is characterized by increased endothelial permeability and coagulopathy. Vasopressin analog ddAVP (desmopressin) acts by reorganizing and redistributing adhesive and tight junction molecules, enhancing endothelial barrier function. Furthermore, ddAVP increases von Willebrand factor (vWF) plasma levels and thereby potentially enhances platelet-based coagulation. The objective of this study was to assess whether the use of ddAVP results in improvement of both endothelial barrier function and platelet-based coagulation, thereby improving shock reversal and reduce organ failure in a rat model of trauma and transfusion.
Methods Blood products were prepared from syngeneic rat blood according to blood bank standards. Polytrauma was induced in Sprague Dawley rats by a fractured femur and crush injury to the intestines and liver. The rats were hemorrhaged until a mean arterial pressure of 40 mm Hg and transfused with RBCs, fresh frozen plasmas and platelets in a 1:1:1 ratio, and randomized to receive a single dose of ddAVP (n=7 per group). Blood samples were taken up to 6 hours after trauma to assess biochemistry, markers of endothelial injury and coagulation status by rotational thromboelastometry (ROTEM). Organ damage was assessed by histopathology.
Results Rats receiving ddAVP showed significantly better shock reversal compared with controls. Also, coagulation parameters remained stable in the ddAVP treated group, whereas rats in the control group showed deterioration of coagulation parameters, including decreased clot strength and decreased platelet functioning (89% (IQR 82% to 92%) of baseline values). Platelet count and vWF antigen levels at exsanguination did not differ between groups. ddAVP did not reduce markers of endothelial dysfunction nor markers of organ injury.
Conclusions The use of ddAVP in a rat trauma-transfusion model improved shock parameters and ROTEM parameters of clot formation. However, this did not abrogate the amount of organ failure.
Level of evidence Level III.
- multiple trauma
- blood coagulation
- hemorrhage
- animal experimentation
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Endothelial dysfunction in trauma is common. It is related to injury severity and is invariably present in hemorrhagic shock.1 2 Patients in trauma-induced hemorrhagic shock show increased endothelial glycocalyx shedding, as well as a decreased integrity of the endothelial cell tight junctions.3 In trauma, endothelial dysfunction is intrinsically related to coagulation disturbances, as markers of endothelial dysfunction correlate with deranged coagulation parameters,4 as well as a decreased response of platelets to aggregate, as was shown in a rat model of traumatic hemorrhage.5 Collectively, these changes result in organ failure.3 6 Thus, therapies aiming at improvement of endothelial dysfunction may be beneficial in trauma-induced hemorrhagic shock.
A potential therapeutic agent could be the vasopressin analog ddAVP (desmopressin). This agent acts through a cyclic adenosine monophosphate (AMP)-dependent pathway that activates endothelial cells, resulting in reorganization and redistribution of VE-cadherin and other adhesive and tight junction molecules, enhancing the endothelial barrier function.7 8 Thereby, ddAVP can result in an increase in blood pressure. Another potential advantage of using ddAVP in traumatic shock is an upregulation of endothelial cell shedding of von Willebrand factor (vWF),9 thereby improving platelet-based coagulation. In line with this, observational studies in traumatic brain injured patients who were on antiplatelet drugs suggest that ddAVP is associated with decreased hematoma expansion and improved platelet function.10 11 Outside the context of antiplatelet therapy, ddAVP also may reduce the amount of blood loss in patients undergoing cardiac operation.12
We hypothesized that ddAVP, as an additive to standard resuscitation strategies in traumatic hemorrhage, will result in restoration of the endothelial barrier function and improvement in platelet-based coagulation with ensuing hemodynamic improvement, thereby decreasing organ injury in a rat model of trauma and transfusion.
Methods
This study was conducted in compliance with the Animal Welfare Act, the implementing Animal Welfare Regulations, and the Principles of the Guide for the Care and Use of Laboratory Animals. Rats were given free access to water and standard rat chow and were housed under in a 12:12 hours light-dark cycle. All protocols were approved by the Animal Care and Use Committee of the Amsterdam University Medical Centers.
Blood product preparation
Preparation of red blood cells (RBC), fresh frozen plasma (FFP) and platelets (PLT) was conducted according to national Sanquin blood bank standards, as we have done before.13 Rat blood products were prepared 2 days before the experiment, by collecting blood by heart puncture, which was pooled for component preparation and stored according to national Blood Bank standards (Sanquin).
Red blood cell products were prepared by centrifuging whole blood for 10 min at 1892 g at 20 °C. Plasma was separated and the buffy coat was removed. Saline-adenine-glucose-mannitol was added to the erythrocytes to an hematocrit of 55% to 60%. The final products were stored in 50 mL Falcons at 4°C. For preparation of FFP product, plasma was separated from the red blood cells and frozen at −80°C. For preparation of the platelet product, the buffy coat separated from the red blood cell product was diluted with pooled plasma to an hematocrit of approximately 20% and centrifuged for 10 min at 288 g at 20°C to remove the majority of the remaining erythrocytes and leucocytes. The supernatant, platelet-rich plasma was stored under continuous movement in culture flasks at 22°C under a 5% CO2/95% air.
Trauma model
Sprague Dawley rats were anesthetized using an intraperitoneal injection of KDA (a mixture of Ketamine (1.8 mL 100 mg/mL; Eurovet Animal Health BV, Bladel, Netherlands), Dexmedetomidine (0.5 mL 0.5 mg/mL; Orion Pharma, Espoo, Finland) and Atropine (0.2 mL 0.5 mg/mL; Pharmachemie BV, Haarlem, Netherlands)) in 0.5 mL of NaCl 0.9%. Rats were tracheotomized and put on a mechanical ventilator for the duration of the experiment (Babylog 8000, Dräger, Lübeck, Germany; pressure-controlled mode, 10 cm H2O peak inspiratory pressure, 5 cm H2O positive end expiratory pressure, FiO2 40%). Polytrauma was induced by performing a midline laparotomy, followed by crush injury to the left and medial liver lobes and the small intestine using a surgical clamp covered with silicone tubing. After this, the right femur was fractured using a blunt guillotine.13 An arterial line was placed in the carotid artery to continuously monitor mean arterial pressure (MAP).
Rats were hemorrhaged until a MAP of 40 mm Hg was reached and left in a shock state for 45 min after which transfusion was initiated. At the day of the experiment, all blood products were pooled together to achieve a 1:1:1 ratio of RBCs, FFPs and platelets. Transfusion was given at a rate of 8 to 12 mL/hour through a jugular vein, with a maximum of 25 mL/kg. To quantify endothelial leakage, 30 min before sacrifice rats were infused with 70 kDa dextran labeled with fluorescein isothiocyanate (dextran-FITC, 0.5 mL 100 mg/mL in NaCl 0.9%; Sigma-Aldrich, St. Louis, Missouri, USA) based on previous models.14 15
Randomization
Concurrent with transfusion, rats were randomized to receive a single dose of 3 µg/kg ddAVP intravenously (Sigma-Aldrich, St. Louis, Missouri, USA). Controls animals were given IgG (DAKO, Santa Clara, California, USA). The dose was based on a previous study in hemorrhaged rats.16 Each group consisted of 7 rats. No sham group was used in this experiment, since previous experiments with this model showed that rats do not survive the full duration of the experiment without any resuscitation.13
Sacrifice
Six hours after polytrauma, rats were sacrificed by exsanguination. After exsanguination, the right lung, right kidney, small intestine and liver were removed after ligation of the circulation and fixed in 10% buffered formalin and embedded in paraffin awaiting further histopathological analysis. To determine the amount of leakage of Fluorescein isothiocyanate (FITC) labelled dextran into organs, the circulation was flushed with heparinized saline (200 IE of heparin per liter saline) through the apex of the left ventricle as the inlet, after which the jugular vein was used for the outlet, thereby removing any intravascular blood containing dextran-FITC.
Measurements
At the start and end of the experiment, blood samples were taken to assess full blood count, fibrinogen, Aspartate transaminase (ASAT), Alanine aminotransferase (ALAT), creatinine and lactate dehydrogenase levels. Blood gas analysis was performed every hour (Siemens Medical Solutions Diagnostics, Erlangen, Germany).
To further assess the coagulation status of the rats, rotational thromboelastometry (ROTEM Delta, Werfen, Bedford, USA) was used. An EXTEM, INTEM and FIBTEM assay was performed at baseline, start of resuscitation, during resuscitation, 120 min after start of resuscitation and just prior to exsanguination. Platelet based coagulation was defined by subtracting the EXTEM and the FIBTEM assay, as this reflects the contribution of platelets to the clot formation.
ELISA
At baseline and after sacrifice, levels of endothelial dysfunction markers soluble syndecan-1 and soluble vascular endothelial (sVE)-cadherin were measured using enzyme-linked immunosorbent assays (ELISA) according to the manufacturer (Elabsience, Houston, Texas, USA). Also vWF levels were analyzed, using pooled plasma (made in the preparation of FFP products) as a control (A0082, Dako, Agilent Technologies, Carpinteria, California, USA).
Histopathological examination of organs
For histopathological examination, H&E staining was performed. A pathologist blinded to the treatment groups examined the tissues and graded the severity of injury to the organ on a scale of 0 to 3 (0=absent, 1=mild, 2=moderate, 3=severe), as we have reported before.13 In short, liver injury was assessed by scoring the presence of necrosis, hemorrhage, portal inflammation and neutrophil infiltration. Kidney injury was scored on the presence of epithelial necrosis or luminal necrotic debris in the cortical tubules, tubular dilation, neutrophil extravasation and hemorrhage. Lung injury was assessed by scoring the presence of lung edema, interstitial inflammatory cell infiltration, endotheliitis and hemorrhage. Injury to the small intestine was scored on the presence of diffuse swelling of the villi, neutrophil infiltration in the submucosa, necrosis and hemorrhage.
Organs were also examined for the presence of thromboembolic events.
Fluorescence microscopy
To determine the amount of dextran-FITC leakage through the endothelium into organs, pathology slices of the lungs were deparaffinized using alcohol and colored using a rabbit—anti-FITC/anti-rabbit HRP and NovaRed coloring method. Every slice was photographed five times using a 10× magnification without any vessels in the frame. Images were acquired using a Leica DM-RA Microscope, coupled to a CCD camera (Leica Microsystems, Wetzlar, Germany) equipped with Image‐Pro Plus software (Media Cybernetics, Rockville, USA). Five random inverted pictures were used to set a threshold positive for 70 kDa dextran-FITC leakage. Median percentage of area intensity was used as measure for endothelial leakage. All pictures were coded prior to assessments to blind the assessor for treatment allocation.
Statistics
Data was presented as a median and IQR and comparisons between groups was tested using the Mann Whitney U test. For differences over time, the Wilcoxon Signed Rank test was used. In a previous rat transfusion model, infusion of ddAVP reduced vascular leakage in the small intestine, with a mean difference of 70 µg/g (SD, 40 µg/g).17 Therefore, to obtain a power of 80%, assuming a 5% significance level and using a two-sided unpaired t test, a total of seven rats should be randomized to each group. All statistics were performed using SPSS Statistics 25.0. P values of 0.05 or smaller were considered to be statistically significant.
Results
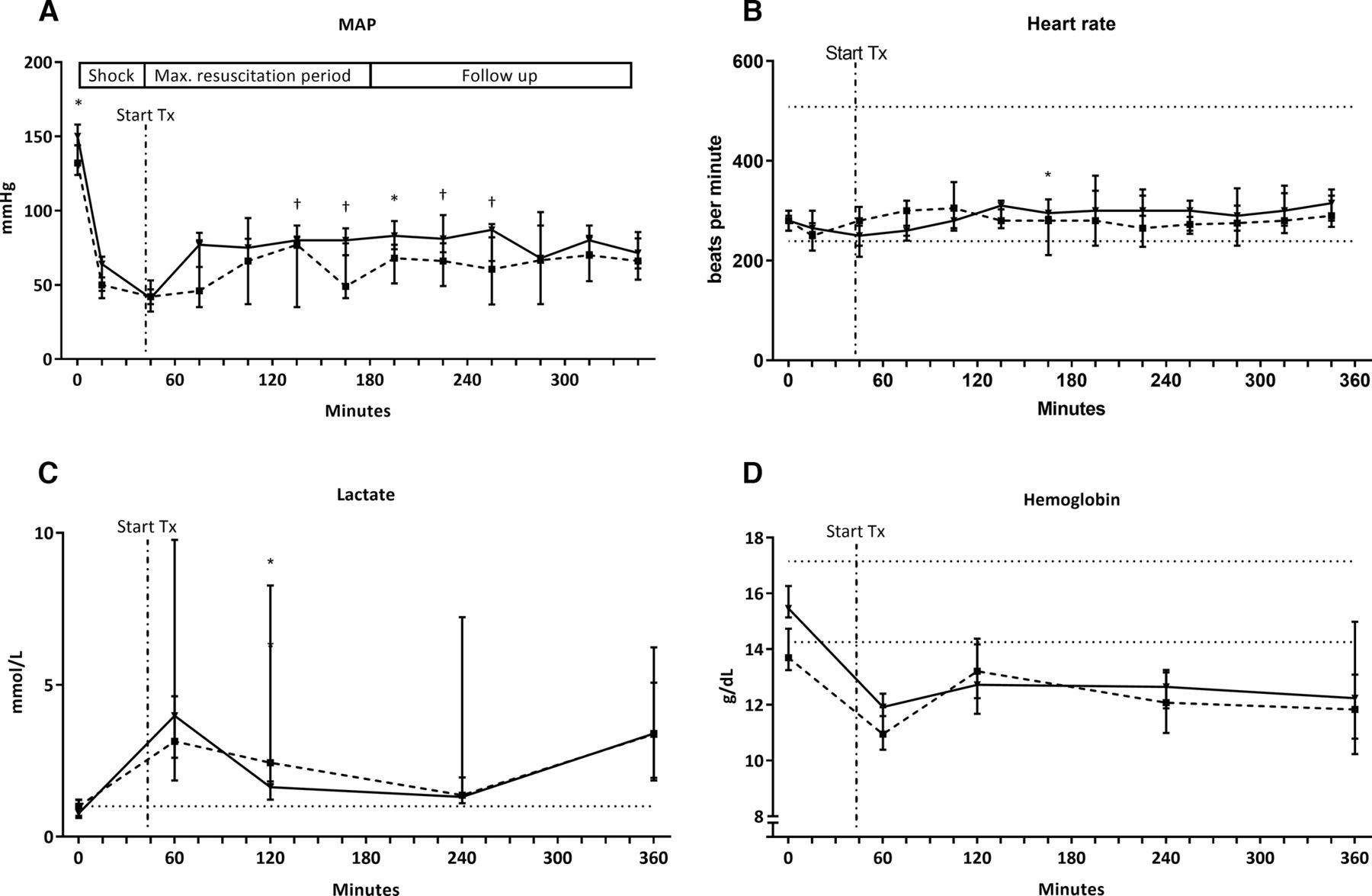
Baseline hemodynamic, biochemistry and coagulation characteristics were similar between rats in the control group and rats receiving ddAVP, with the exception of baseline MAP which was higher in the ddAVP group (table 1 and figure 1A). After trauma and hemorrhage, rats in the ddAVP and control group showed similar signs of hypovolemic shock, with low MAP, base deficit and increased lactate levels, without differences between groups (table 1). Mortality rates differed between groups, as two rats in the control group did not survive the full duration of the experiment. Animals expired at 4 and 5 hours postinjury. Macroscopic autopsy of these rats did not show a clear cause of death. Rats receiving ddAVP all survived until the moment of sacrifice.

Hemodynamics and shock parameters over time. Values presented as median and IQR.  ddAVP
ddAVP  ; control. (A) MAP expressed in mm Hg. Start Tx (dot-dashed line) is the initiation of resuscitation, as well as when the ddAVP bolus was given. (B) Heart rate expressed in beats per minute. (C) Lactate levels expressed in mmol per liter. (D) Hemoglobin levels expressed in grams per dL. Dotted lines are reference values. *P<0.05, †p<0.10. MAP, mean arterial pressure.
; control. (A) MAP expressed in mm Hg. Start Tx (dot-dashed line) is the initiation of resuscitation, as well as when the ddAVP bolus was given. (B) Heart rate expressed in beats per minute. (C) Lactate levels expressed in mmol per liter. (D) Hemoglobin levels expressed in grams per dL. Dotted lines are reference values. *P<0.05, †p<0.10. MAP, mean arterial pressure.
Baseline and shock characteristics
The effect of ddAVP on hemodynamic parameters
After transfusion was initiated, median duration to reach a MAP of 70 mm Hg was 66 (18 to 300) min for control rats, whereas rats in the ddAVP group reached this within 23 (21 to 50) min (p=0.654).
Overall during resuscitation, rats receiving the ddAVP bolus had higher median MAP values compared with control rats. Also, correction of shock seemed to be more effective in ddAVP treated rats, as reflected by lower lactate levels 120 min postinjury (2.4 vs 1.6 mmol/L, p=0.046). After the resuscitation period, lactate levels increased gradually in both groups (figure 1).
The effect of ddAVP on coagulation parameters
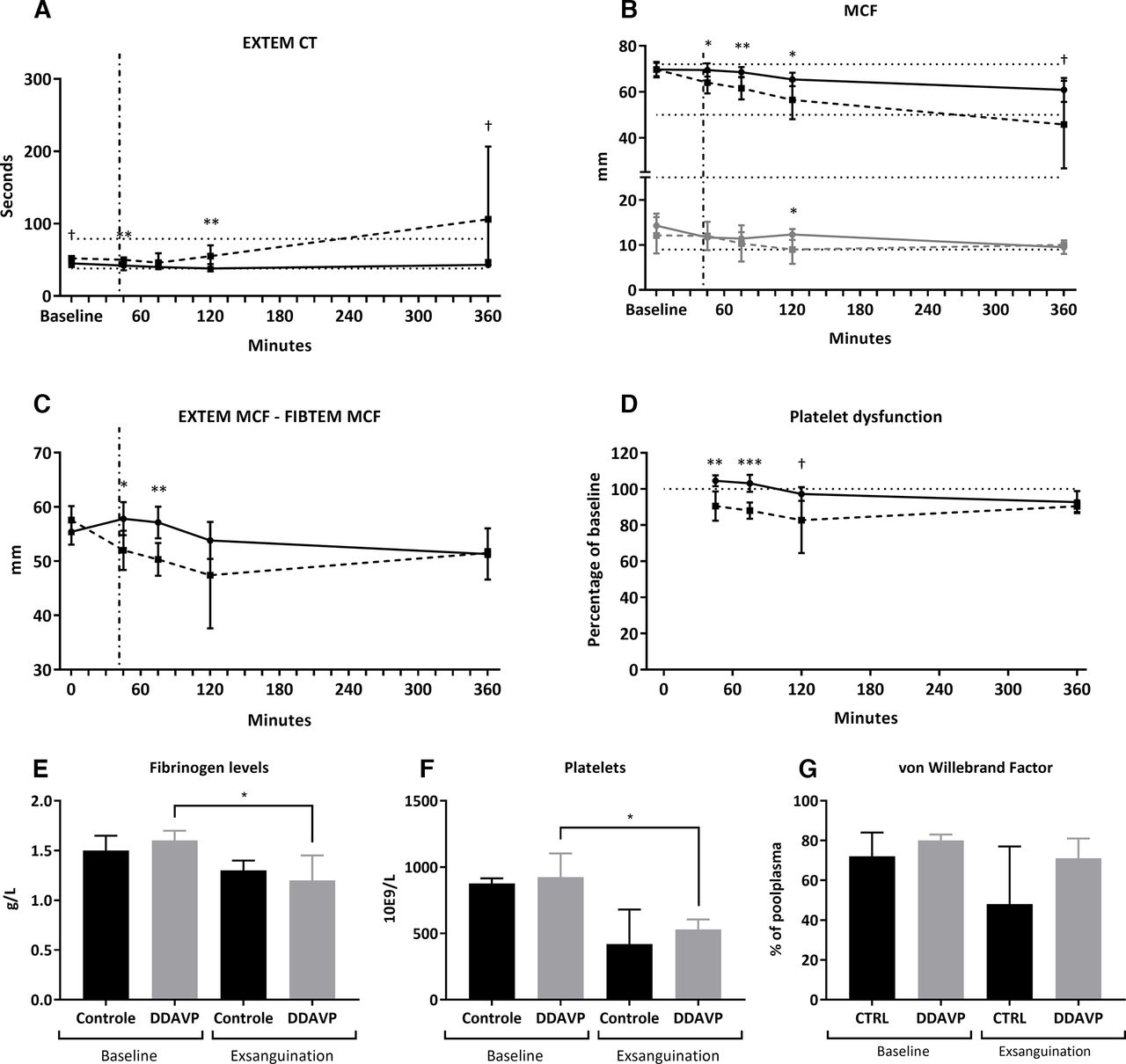
Rats randomized to the ddAVP group showed a stable EXTEM clotting time (CT) and maximum clot firmness (MCF) after resuscitation was initiated, whereas rats in the control group deteriorated, as reflected by a prolongation of EXTEM CT and a decrease in EXTEM MCF. This difference between the groups increased for both parameters over time (figure 2A,B).

Coagulation parameters. Values presented as median and IQR.  ddAVP
ddAVP  ; control. Dot-dashed line is the initiation of resuscitation as well as when the ddAVP bolus was given. (A) CT expressed in seconds, as measured in the EXTEM assay. (B) MCF expressed in millimeters, as measured in the EXTEM and FIBTEM assay. (C) Reflection of platelet dysfunction expressed in mm, as measured by subtraction of EXTEM and FIBTEM MCF. (D) Platelet function relative to baseline values expressed as a percentage. (E) Levels of fibrinogen measured in grams per liter, at baseline and at sacrifice. (F) Levels of platelets ×109 per liter, at baseline and at sacrifice. (G) Levels of von Willebrand factor measured as a percentage of pooled plasma, at baseline and at sacrifice. Dotted lines represent (human) references values. †P<0.10, *p<0.05, **p<0.01, ***p<0.001. CT, clotting time; MCF, maximum clot firmness.
; control. Dot-dashed line is the initiation of resuscitation as well as when the ddAVP bolus was given. (A) CT expressed in seconds, as measured in the EXTEM assay. (B) MCF expressed in millimeters, as measured in the EXTEM and FIBTEM assay. (C) Reflection of platelet dysfunction expressed in mm, as measured by subtraction of EXTEM and FIBTEM MCF. (D) Platelet function relative to baseline values expressed as a percentage. (E) Levels of fibrinogen measured in grams per liter, at baseline and at sacrifice. (F) Levels of platelets ×109 per liter, at baseline and at sacrifice. (G) Levels of von Willebrand factor measured as a percentage of pooled plasma, at baseline and at sacrifice. Dotted lines represent (human) references values. †P<0.10, *p<0.05, **p<0.01, ***p<0.001. CT, clotting time; MCF, maximum clot firmness.
Also, directly after the ddAVP bolus was given, rats in the ddAVP group showed significant higher EXTEM-FIBTEM MCF values when compared with the controls (56.5 vs 52.0 mm, p=0.015). This difference remained 30 min after the bolus was given (56.5 vs 49.5 mm, p=0.012). Platelet function relative to baseline values remained around 100% in the ddAVP group, whereas it approximated 89% (IQR 82% to 92%) of the baseline values in the control rats. At the end of the experiment, these differences had disappeared (figure 2C,D).
FIBTEM MCF and fibrinogen levels did not differ between groups (figure 2B,E). Platelet counts and levels of vWF were also similar between groups at the start of the experiment and at exsanguination (figure 2F,G).
The effect of ddAVP on markers of endothelial barrier function
At sacrifice, both groups showed higher levels of circulating syndecan-1 compared with baseline (control: 24 vs 29 ng/mL, p=0.043; ddAVP 23 vs 30 ng/mL, p=0.173) and higher VE-cadherin levels (control: 5746 vs 9874 pg/mL, p=0.068; ddAVP: 5577 vs 7753 pg/mL, p=0.028), indicating endothelial injury. The change in markers of endothelial injury relative to baseline trended to be lower in ddAVP treated rats compared with rats in the control group (syndecan-1: 130 vs 149%, p=0.361; VE-cadherin: 133 vs 311%, p=0.136), although not reaching statistical significance. Vascular leakage of dextran-FITC (1.8 vs 0.9% of area intensity, p=0.638, figure 3) did not differ between groups.

{kind=link}
{kind=link}
{kind=link}
Markers of endothelial and organ functioning. Values are expressed as median percentage and IQR. (A) Syndecan-1 levels expressed as a percentage relative to their baseline values. (B) VE-cadherin levels expressed as a percentage relative to their baseline values. (C) Percentage of area covered by dextran-FITC leakage into pulmonary parenchyma. (D) Creatinin levels measured in heparinized plasma at baseline and exsanguination. (E) Protein levels as measured in urine samples at baseline and exsanguination. (F) Aspartate transaminase (ASAT) levels measured in heparinized plasma at baseline and exsanguination.
The effect of ddAVP on organ failure
Trauma resulted in signs of liver cell degradation, kidney injury and an impaired coagulation system. However, ddAVP treated animals did not differ from controls in terms of biochemical assessment of organ function (figure 3). Also, histopathological examination and scoring was similar between ddAVP treated and control rats (kidney score 0.8 vs 0.5; liver score 0.8 vs 0.4; lung score 0.8 vs 0.6; small intestine score 0.5 vs 1.0; total score 2.8 vs 2.4).
Discussion
In our rat model of traumatic injury and hemorrhage, the addition of ddAVP to standard therapy resulted in a transient improvement of shock reversal and of ROTEM parameters of coagulopathy when compared with rats receiving standard therapy only. The trauma model was characterized by a loss of endothelial integrity and organ injury. However, ddAVP did not reduce vascular leakage, nor the amount of organ damage.
In this model in which a fixed resuscitation volume was used, ddAVP treated rats had higher MAP values. Although several trauma hemorrhage models17 18 and clinical studies19 have investigated the use of vasopressin, a vasopressor analog targeting the V1 receptor in vascular smooth muscles resulting in a direct vasoconstrictor effect on the vascular system and an increase in systemic blood pressure, ddAVP (desmopressin) is less studied and appears to have no apparent vasopressor effect. ddAVP binds to V2 receptors in the renal collecting ducts, resulting in water reabsorption,20 which may at least in part have resulted in an increased volume in the systemic vasculature and subsequently higher blood pressure. Several studies have also proposed an effect of ddAVP on V1 receptors during severe volume depleted states, such as in our hemorrhage model, resulting in vasoconstriction.21 The differences in MAP and lactate levels between groups in our experiment became apparent approximately 1.5 hours after infusion, which is when plasma levels of ddAVP are highest.22 We also noted that effects of a single dose of ddAVP were transient.
Our results add to these findings by showing that ddAVP administration results in improved platelet-based coagulation. This may have been a result of increased release of vWF into the circulation after ddAVP infusion,23 as was also shown in patients with von Willebrands disease. However, no differences between vWF antigen levels were found between groups at the end of the experiments. Possibly, this timepoint was too long after DDAVP infusion, as vWF levels normalize to baseline values within hours after infusion.24 This may also explain why the differences in the coagulation profiles of our groups no longer existed at the 6-hour postinjury time point.
Previous studies have suggested that the use of ddAVP may improve the endothelial barrier function,8 as was shown in a model of septic sheep.25 In our study, ddAVP resulted only in a trend towards decreased glycocalyx shedding of syndecan-1 and lower levels of circulating VE-cadherin in ddAVP treated rats, without reducing vascular leakage of dextran-FITC to the pulmonary parenchyma. The increase in blood pressure in the ddAVP treated rats may have contributed to increased vascular leakage, thereby nullifying the effect of ddAVP treatment, as was proposed in a previous model of hemorrhagic shock.17 Alternatively, increased shedding of vWF in ddAVP treated rats may have led to formation of microthrombi leading to an occlusion of the microcirculation leading to endothelial damage and dysfunction, although evidence supporting (micro)thrombosis after ddAVP infusion is scarce12 26 and histopathologic examination of the organs of the rats in our experiment showed no signs of thrombosis in both groups. Also, the timespan of our model may have been too short to find a significant difference in endothelial barrier function between groups.
It should be noted that organ and endothelial functioning were measured at baseline and sacrifice only, as blood sampling of these shocked rats was possible only to a limited extent. Thereby, at sacrifice (6-hour postinjury), the possible beneficial effect of ddAVP may have worn out, as its tmax is approximately after 1.5 hours. Therefore, future experiments should measure the effect of a continuous or intermittent administration of ddAVP with repeated measurements of vWF kinetics, endothelial integrity and organ functioning.
In conclusion, the use of a single bolus of ddAVP transiently improves shock reversal and ROTEM parameters of clot formation in a rat trauma-transfusion model, without an effect on endothelial barrier function or organ injury. The use of ddAVP as an adjunctive therapy in trauma hemorrhage shows promising results in our preclinical model but should be further studied.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
The authors gratefully acknowledge professor Jan Voorberg (Department of Plasma Proteins, Sanquin Research, Amsterdam, The Netherlands) for his help interpreting the results.
References
Footnotes
Contributors MRW performed experiments. MRW analyzed results and made the figures. JJR performed histopathological examination of the organs and scored them as described in the methods section. MRW, JCG and NPJ designed the research and wrote the article. JCG and NPJ are guarantor of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.