Article Text

Abstract
Objectives Hemoglobin (Hb) levels have been considered to remain stable in the early stages of bleeding due to trauma. However, several studies have reported that rapid compensatory fluid shifts cause Hb dilution earlier than previously thought. These reports are from Western countries where it is standard protocol to administer fluids during an emergency, making it almost impossible to eliminate the effect of prehospital intravenous fluid administration on Hb levels. This study aimed to determine the relationship between Hb levels and severity of injury on arrival at the hospital in severe trauma patients without prehospital intravenous fluid administration.
Methods This single-center observational retrospective study included patients with Abbreviated Injury Scale scores of 3 or above between 2008 and 2014. In Japan, prehospital life-saving technicians were not allowed to administer intravenous fluids until 2014. We investigated whether the difference between the measured blood Hb level at arrival and the corresponding standard blood Hb level for each age group and sex reported in the national survey was associated with the severity of injury and the need for hemostasis.
Results In total, 250 patients were included in this study (median age, 46 years; male patients, 183). The median time from injury to arrival at the hospital was 45 min, and there was no statistical correlation with the initial Hb level on arrival (ρ=0.092, p=0.14). When the study subjects were stratified into four groups according to the initial Hb levels, lower Hb levels correlated with higher rates of requirement for hemostatic interventions (p=0.02) and mortality (p=0.02). In addition, lower Hb levels were associated with the need for hemostasis.
Conclusion In severe trauma patients without prehospital intravenous fluid administration, decreased Hb levels on arrival may be associated with the severity of trauma and with the need for hemostasis.
Level of evidence Level IV.
- emergency department
- clinical assessment
- emergency treatment
- hemorrhage
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Trauma is still the leading cause of high morbidity and mortality both in industrialized and low-income and middle-income nations.1 Trauma-related death, especially in younger patients, is a huge socioeconomic loss.2 Early identification of bleeding sites for immediate surgical control is critical for severe trauma patients. Several physiological signs, such as heart rate, systolic blood pressure (SBP), altered mental status, or clammy skin can appear soon after the trauma and help physicians identify patients with ongoing traumatic bleeding. These physiological parameters, however, are non-specific, and lowered SBP often manifests only in the very late stage of trauma. Laboratory data such as base deficit or serum lactate levels are also parameters for insufficient peripheral perfusions due to hypovolemia, but these parameters are not always instantly available. The testing kit for peripheral blood hemoglobin (blood Hb) level, however, is generally available at the patient’s bedside. Blood Hb levels, however, have not been considered to be a marker for severe bleeding in the early stages of trauma because of a long-held belief that the compensatory mechanism that replaces the loss of blood volume in the vascular system takes effect slowly. Traditionally, it has been believed that blood component values require hours to equilibrate; however, recent investigations regarding Hb levels at the time of hospital admission of severe trauma patients have reported that peripheral levels of Hb can be lowered even during the very early stages of trauma.3–6 Bruns et al reported that an early decrease in Hb levels can be associated with the severity of bleeding in trauma patients.3 4 The study subjects in these previous studies, however, received prehospital intravenous fluid administration. The effect of prehospital infusion may be minimal; however, the dilution effect cannot be ignored. Other studies also included severe trauma patients with massive fluid resuscitation because of their hypotensive status, which may have resulted in lowered Hb levels.5 In Japan, until 2014, owing to restrictions imposed by the national legislation, certified prehospital emergency life-saving technicians were not allowed to administer intravenous fluids to hypotensive trauma patients. In our institution, prehospital infusions were gradually allowed to be performed under the direction of a doctor from the second half of 2014; but in 2014, no trauma patients with infusions were treated at our hospital. The aim of this study was to evaluate the relationship between early changes in Hb levels after hospital arrival, severity of the trauma, and need for hemostasis in severe trauma patients not receiving fluids. We hypothesize that severe trauma patients have an early decrease in Hb levels after an injury even if they are not receiving fluids.
Methods
Study design
The present study was a retrospective analysis of trauma patients. The study period was from January 2008 to December 2014, a period during which data of injured patients brought to the hospital without prehospital infusion owing to limited ambulance services were collected. To prevent inclusion of patients with minor injuries, only patients with Abbreviated Injury Scale (AIS) scores of 3 or more, but those without distinctive pathologies such as burns, hanging, strangulation injuries, intoxication, or hypothermia/hyperthermia, were included in the analysis. The exclusion criteria were as follows: (1) aged younger than 20 or older than 69 years; (2) cardiac arrest before hospital arrival; (3) transferred from other hospitals; (4) missing information on the time elapsed since the trauma; (5) missing information on Hb levels on arrival at the hospital; (6) isolated head injury with suspected elevated intracranial pressure, without injuries to the torso or extremities; and (7) history of anemia.
Patient and public involvement
This study involved trauma patients from the civilian population.
Emergency medical service prehospital protocol for trauma
During the study period, emergency life-saving technicians, who are trained prehospital medical providers, were not allowed to administer intravenous fluids in the field or en route to the hospital in our study region. The emergency medical service crews had duties limited to oxygen administration, fixation of extremities with splints, and spinal immobilization. They could also manage the airways manually.
Initial trauma care in the emergency department
In Japan, initial trauma care is based on a unique protocol, Japan Advanced Trauma Evaluation and Care (JATEC).7 The structure of the primary survey (physiological, ABCDE approach) and secondary survey (history taking, anatomical, systemic approach) is the same as that of the Advanced Trauma Life Support.8 This unique protocol has been developed in response to the high prevalence of blunt trauma in Japan. The JATEC protocol recommends emergency hemostasis for bleeding that can lead to circulatory deterioration. In our institution, according to this protocol, aggressive surgical hemostasis or arterial embolization is indicated for active hemorrhage with circulatory deterioration, depending on the patient’s condition.
Hemoglobin measurement and data collection
Blood laboratory evaluations were performed soon after patients’ arrival at our emergency department. Whole blood cell counts were measured on LH 780 or DxH800 (Beckman Coulter, California, USA) using standard laboratory techniques.
Blood Hb levels are affected by age and sex.9 The Japanese Ministry of Health, Labour, and Welfare conducted a national survey on standard blood Hb levels (online supplemental table S1).10 This survey shows that Hb levels can physiologically be associated with age and sex. To minimize the effect of age and sex on initial Hb levels, we used the difference between the measured blood Hb level at arrival and an age-matched and sex-matched reported standard blood Hb level for each 10-year age group (delta Hb (ΔHb) g/L) as the evaluation variable.
Supplemental material
We stratified the study patients into quartiles (120<Hb, 120≤Hb <130, 130≤Hb <140, 140≤Hb) based on the initial Hb levels per 10 g/L with reference to the initial four Hb quartiles and assessed the following physiological variables: SBP, age, sex, Glasgow Coma Score, blood lactate levels, whether open thoracotomy or laparotomy for hemostasis or transcatheter arterial embolization was performed within 12 hours of arrival, the time from the emergency call to hospital arrival, and mortality. These data were collected from the electronic medical records of our institution.
Statistical analysis
Continuous variables are described as median and IQRs, and categorical variables are described as percentages. Spearman’s correlation coefficient was used to evaluate the distribution of blood Hb levels from the time of the emergency call to hospital arrival. Then, variables were compared between the stratified Hb groups using the Kruskal-Wallis test for continuous variables and the χ2 test for categorical variables. In addition, the effects of the information, such as ΔHb, age, sex, injury mechanism, time of injury to hospital arrival, and Injury Severity Score (ISS), determined before obtaining hemoglobin values on the need for hemostasis were assessed using logistic regression analysis. All statistical analyses were performed using a statistical analysis software (SPSS V.22, Chicago, Illinois, USA). Results were considered to be statistically significant at a p value <0.05.
Results
Among the 1271 trauma patients who presented to our emergency department during the study period, 250 patients met the inclusion criteria. A detailed flow diagram of the study is presented in online supplemental figure S2. Patients with missing data (time of the injury unknown (n=87) and Hb levels not available (n=29)) were excluded. The excluded isolated head injury patients did not differ significantly in age or sex from the study population. The characteristics of the study population are shown in table 1. The median age was 46 years, and 73.2% of the patients were male. Blunt trauma accounted for most injury mechanisms (96.0%). The median time from the emergency call to hospital arrival was 44.5 min. Online supplemental table S3 shows the distribution of AIS scores of the studied patients. Median values for the AIS score and the probability of survival (based on trauma and ISS) were 21 and 0.96, respectively. Generally, injuries with a lower severity (AIS score of 0–3) occurred on the skin and face, while injuries to the neck, head, abdomen, and extremities were more severe (AIS score up to 6). Sixty-seven patients (26.8%) underwent definitive hemostasis surgery or damage control surgery, either open thoracotomy or laparotomy, or emergency transcatheter arterial embolization within 12 hours of arrival. Death during hospitalization was 9.2% (23/250) with a median ISS of 38 and median probability of survival of 0.43. The cause of death was brain injury in 11 cases and hemorrhage from multiple traumatic injuries in the rest.
Supplemental material
Supplemental material
Characteristics of the study population
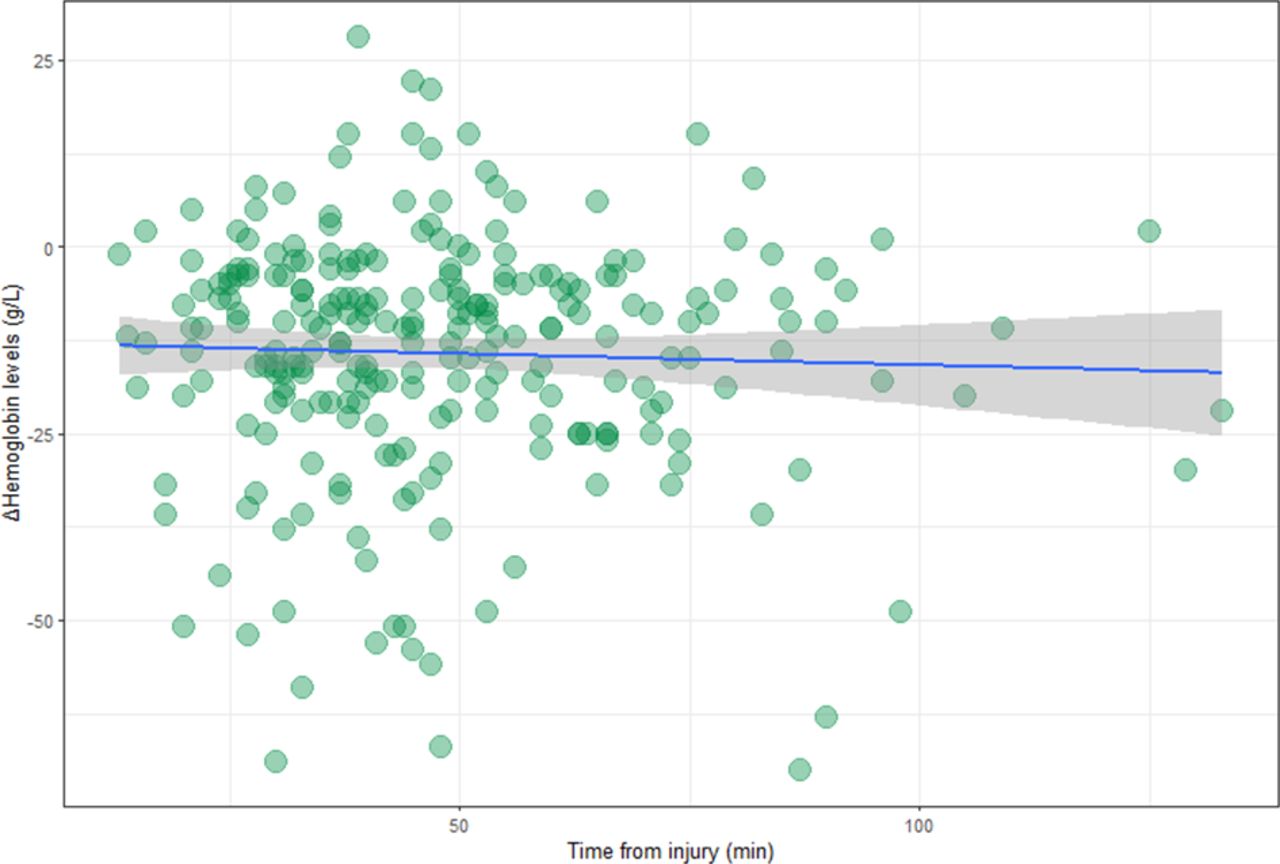
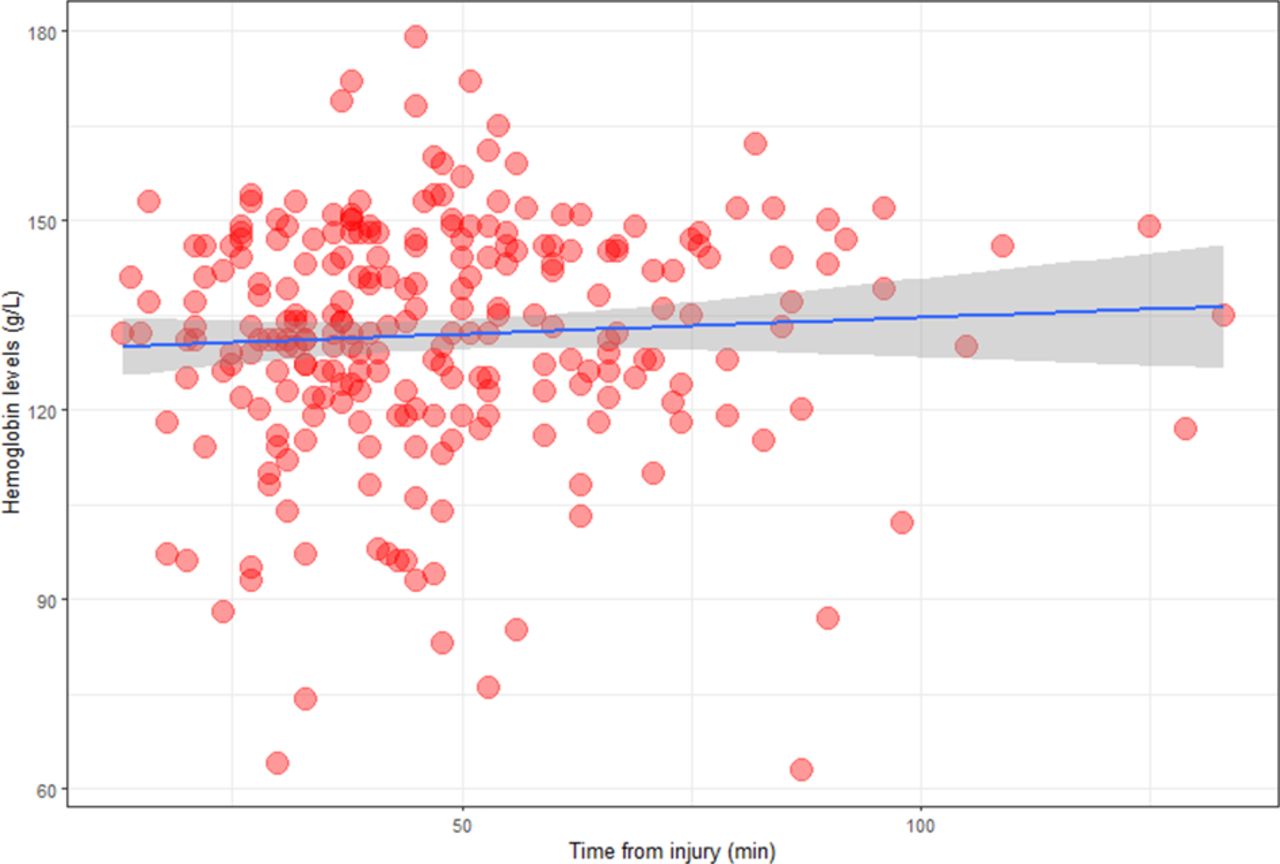
The median Hb level on arrival was 133 g/L with an IQR of 123–146. The correlation between admission Hb levels and time from the emergency call to hospital was weak with ρ=0.093 and p=0.14 determined using Spearman’s correlation (figure 1). The ΔHb levels, obtained by subtraction of the measured blood Hb level at arrival from the standard Hb levels reported by the national survey,10 also had no correlation with time from the emergency call to hospital arrival (ρ=−0.027, p=0.67, figure 2). Table 2 shows the comparison of various clinical factors between patient groups stratified by initial Hb levels. Patients with lowered Hb levels were found to be older (p<0.01), male (p=0.01), hypotensive (p<0.01), had a lower revised trauma score (p=0.02), and required interventions for hemostasis within 24 hours of arrival (p<0.01). These patients had higher mortality rates. A comparison of the stratified groups by ΔHb ensured that the effects of the physiological difference with age or sex were minimized; however, lower ΔHb levels continued to be correlated with a lower revised trauma score (p=0.01), higher frequency of requirement for hemostatic interventions (p=0.02), and mortality (p=0.02) (table 3). In addition, ΔHb showed a decrease greater than −10 g/L in 56% of the patients and was not related to the time from injury to hospital arrival, as shown in figure 2.
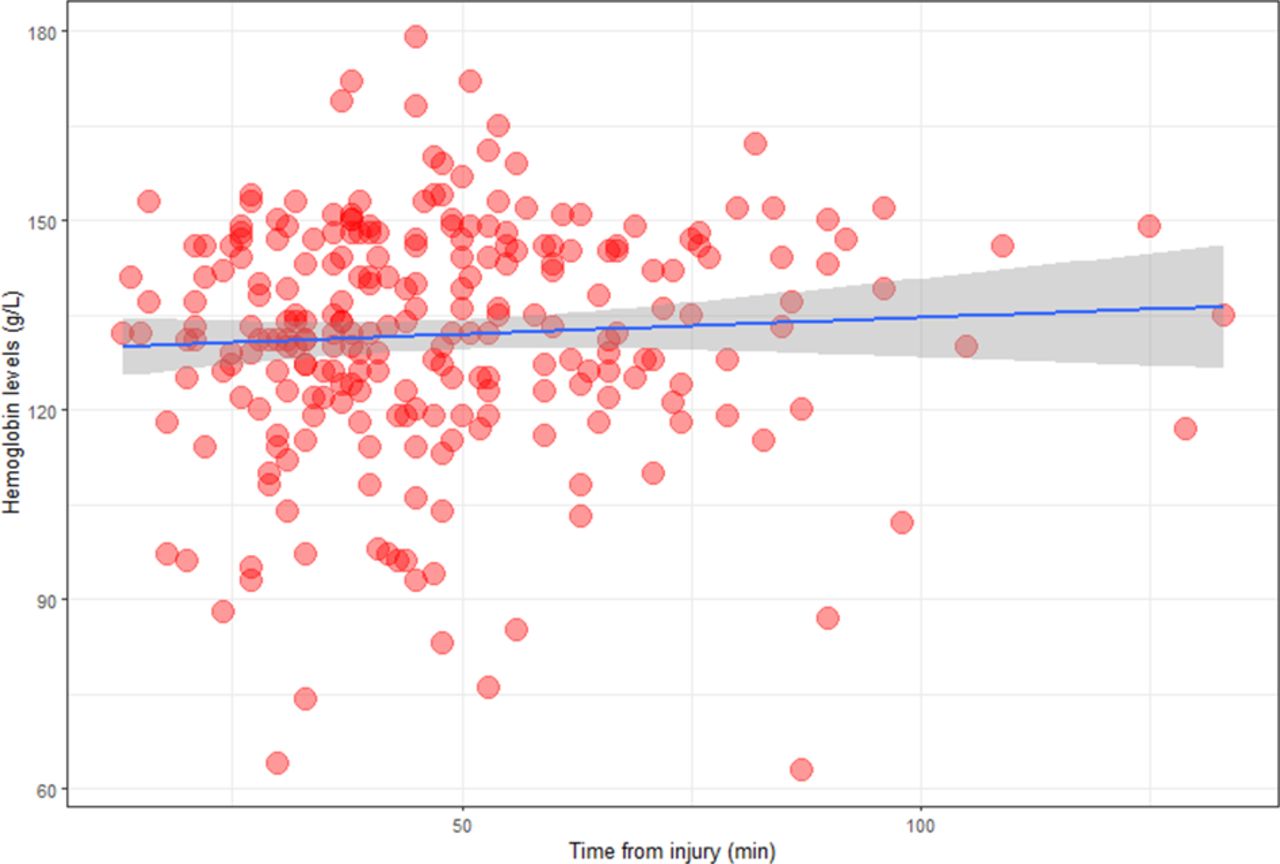
Correlation between hemoglobin level on arrival and time from the emergency call to arrival at the hospital. The blue line and grey range depict the least-squares method of approximation and the range of SEs, respectively. The median hemoglobin level on arrival was 133 g/L, and there was no correlation between hemoglobin levels and the time from the emergency call to arrival at the hospital.
{kind=link}
{kind=link}
Correlation between Δ hemoglobin level on arrival and time from the emergency call to arrival at the hospital The blue line and grey range depict the least-squares method of approximation and the range of SEs, respectively. There was no correlation between Δ hemoglobin level on arrival and the time from the emergency call to arrival at the hospital. Spearman’s rank correlation coefficient=−0.027, p=0.67.
Association between decreased Hb levels and clinical variables
Association between Δ hemoglobin (∆Hb) levels and clinical variables
Logistic regression analysis of risk factors associated with the need for hemostasis showed that lower Hb levels were associated, even after considering age and sex, injury mechanism, and the time from injury to hospital arrival (table 4).
Logistic regression analysis of risk factors associated with the need for hemostasis
Discussion
This study investigated initial Hb levels of severe trauma patients (AIS score of 3 or more) without prehospital fluid administration. When matched for age and sex, ΔHb values were not associated with the time from injury to hospital arrival, and some patients showed a decline immediately after injury. These decreases in ΔHb levels were found to be associated with lowered SBP, more frequent need for hemostatic procedures, and mortality. Furthermore, even after accounting for risk factors for decline in ΔHb levels on hospital arrival, the decline in ΔHb was still associated with the need for hemostasis.
Our study findings of lower Hb levels in trauma patients without prehospital intravenous administration were consistent with those of previous studies. Bruns et al conducted a retrospective study on 404 trauma patients and found that patients were more likely to require surgical hemostasis, if Hb levels on arrival were 100 g/L or lower.4 Similarly, Ryan et al reported that the hematocrit level on arrival was associated with signs of hypovolemic shock and the amount of blood loss.6 Additionally, a recent prehospital study focused on the very early phase of injury and found that for a given prehospital fluid volume infused, the magnitude of the Hb drop was significantly higher in patients with significant hemorrhage than in controls.3 However, we could not draw direct comparisons with this study, as Hb drop was measured after prehospital fluids were administered.
A question that arises from these findings is how long it takes for the body to compensate for blood loss. It has been conventionally believed that after the compensation mechanisms for acute blood loss come into effect, it takes a relatively long time before Hb levels decrease.11 There are animal experiments12–15 and human studies1 5 6 16–20 indicating that the compensatory mechanism comes into effect early after blood loss and hematocrit levels decrease immediately. However, a thorough literature search revealed that no human studies or animal experiments12–15 have investigated how this mechanism takes effect in the absence of fluid administration. In human studies, it is practically impossible to exclude trauma patients that have received prehospital fluid administration when investigating Hb levels among severe trauma patients. In this study, we were fortunate to be able to retrospectively investigate trauma patients with no prehospital fluid administration and could validate the findings through a retrospective analysis of patients’ data. Furthermore, we examined the association between transport time intervals and Hb levels on arrival and found that no significant correlation exists between the time intervals and decreased Hb levels. The median time interval for transportation was 45 min, which indicates that the compensatory mechanisms come into effect soon after the injury.
Our study, similar to previous studies, indicates that a simple blood Hb measurement can be used to distinguish severe trauma patients who require immediate surgical hemostasis and massive blood transfusion from other trauma patients. ISS was more strongly associated with the need for hemostasis. However, ISS is determined after imaging and cannot be confirmed immediately on arrival at hospital. Hb measurement is a simple and readily available test in both clinics and hospitals. Our results also suggest that it may be beneficial to measure Hb even in prehospital settings.
There are several limitations to this study. First, this study was a retrospective study, which limited the data that could be collected. The condition of the trauma patients on arrival at hospital is influenced by a large variety of factors. For example, we could not be certain whether respiratory or circulatory influences were responsible for the high lactate levels. In addition, as the severity of the injury was assessed using the AIS score, injuries that could not be coded using the AIS scoring system, such as soft tissue injuries, may have been underestimated. Second, this study was conducted in a single trauma center in Japan. Further studies comprising larger populations are needed to validate the present results. However, it will be seemingly impossible to enrol only severely injured patients who have not received prehospital fluid administration in industrialized countries, since many countries’ protocols of emergency medical services allow this procedure. Third, although we excluded unwitnessed cases, time intervals of the included cases may not be always entirely accurate owing to the observational nature of these data. Fourth, while we attempted to exclude patients with pre-existing conditions that could lower patients’ blood Hb levels, some patients with undiagnosed conditions known to lower Hb levels may have been included. Finally, the decision as to when hemostatic interventions should be performed was made by the physicians in charge and were not controlled in this study. This could have led to an unknown bias—lower the Hb level, the more likely the patients were to receive hemostatic interventions.
This study focused on severe trauma patients without prehospital intravenous administration of fluids and identified that lower Hb levels on arrival at the hospital were associated with the severity of the trauma. Furthermore, lower Hb levels were found to be associated with the need for hemostasis. This indicates that the Hb level, which can be easily measured on site, may be clinically useful for estimating the severity of trauma patients.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the ethics committee of Nara Medical University, Nara, Japan (No. 2322), and the need for informed consent was waived owing to the retrospective observational nature of the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors YK: conceptualization, formal analysis, investigation, methodology, visualization, writing—original draft, writing—review and editing, guarantor. HF, HA, KT, AO, YT, and NM: data curation, formal analysis, writing—review and editing. FB: writing—review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.