Article Text

Abstract
Background Blunt cerebrovascular injuries (BCVI) remain a significant source of disability and mortality among trauma patients. The purpose of the present study was to determine whether knowledge silos exist in the overall BCVI literature.
Methods An object-oriented programmatic script written in Python programming language was used to extract and categorize articles and references on the topic of BCVI. Additionally, each BCVI article was searched for by digital object identifier in the other BCVI references to build a network analysis and visualize topic reference patterns. Analyses were performed using Stata V.14.2 (StataCorp).
Results A total of 306 articles with 10 282 references were included for analysis. Of these, 24% (74) were published in neurosurgery journals, 45% (137) were published in trauma journals, and 31% (95) were published in a journal of another specialty. Similar proportions were found when categorized by author departmental affiliation. Trauma surgery authors disproportionately referenced articles in the trauma literature, compared with neurosurgeons (73.5% vs. 48.0%, p<0.0001), and other authors. The biggest factor influencing reference proportions was the specialty of the publishing journal. Finally, a network analysis revealed that there are more trauma BCVI articles, and there are more frequently cited trauma BCVI articles by all specialties.
Conclusions This study revealed the existence of a one-way knowledge silo in the BCVI literature. However, a robust preference by both trauma and neurosurgery to cite trauma references when publishing in trauma journals may indicate a possible conscious curating of citations by authors to increase the likelihood of publication. These observations highlight the need for an active role by journal editors, peer reviewers, and authors to actively foster diversity of citations and cross-specialty collaboration to improve dissemination of information between these specialties.
Level of evidence Level IV. Observational study.
- BCVI
- trauma
- silos
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Blunt cerebrovascular injuries (BCVI) to the carotid and/or vertebral arteries are a significant source of ischemic stroke associated with potentially devastating outcomes in the trauma patient population. Historically, the majority of these injuries were only recognized after development of neurologic symptoms and were associated with a morbidity and mortality of nearly 80% and 40%, respectively.1 However, significant efforts led by the trauma community to introduce a classification system and screening guidelines during the late 1990 and early 2000s resulted in heightened awareness and earlier diagnosis of BCVI.2 3 The ability to identify these injuries in a timely manner was further potentiated by the rapid evolution of CT angiography during the ensuing decade.4–6 Furthermore, advances in the field of BCVI also served to attract the interest of overlapping specialties concerned with the management of cerebrovascular disease such as trauma surgery, vascular surgery, cerebrovascular and endovascular neurosurgery, interventional neuroradiology, interventional neurology, and stroke neurology, among others.
Ideally, an array of approaches to investigating the same disease process by different medical specialties would create a synergistic interdisciplinary effort that would strengthen the depth and the quality of the research. However, when effective communication among investigators in different specialties is impeded by the use of different terminologies and platforms for knowledge dissemination, knowledge silos can be created.7 Such a phenomenon stems from divergent rather than conjoint efforts to advance the same field of study and may ultimately frustrate the achievements of the interested parties involved. Knowledge silos may be a widespread but under-recognized issue affecting the medical literature. In the extreme form, complete knowledge silos close communication, with separate specialties pursuing knowledge independently from one another—also known as a two-way silo. Expanding on this concept, a true one-way silo in the theoretical sense then represents a scenario in which one specialty does not acknowledge another’s contributions, while the second specialty fully acknowledges the first. Even partial knowledge silos can delay dissemination of knowledge. Knowledge silos are being increasingly recognized throughout medicine.7–10Despite a sizeable body of literature about BCVI, consensus about the management of this disease remains elusive.11 Because many patients with BCVI also have coexisting injuries, prevention of stroke with antithrombotic medications is problematic and, presently, a wide array of different antithrombotic regimens are in use.12–14 Understanding and management of this complex patient population would benefit from a multidisciplinary approach. Knowledge silos have been found in the pediatric BCVI literature15; the purpose of the present study was to determine whether knowledge silos exist in the overall BCVI literature, to identify contributing factors and potential barriers to silo-busting interventions, and to foster communication between specialties.
Methods
This study did not include any human subjects and did not require Institutional Review Board approval.
Search methodology
Peer-reviewed literature on the topic of BCVI was reviewed to assess for knowledge silos. We aimed to categorize articles and their references by their specialty affiliation to quantitatively assess cross-specialty knowledge sharing on BCVI. A broad search of the Web of Science database was performed to capture as many relevant articles on the topic as possible. ‘Blunt cerebrovascular injury’ was searched with filters for English language and article (document type) from earliest available date through April 2020. Web of Science was selected because it is a citation index that allows for detailed assessment of citation data. While no database is exhaustive, Web of Science represents a large and representative sample to allow for confident conclusions. Articles returned were evaluated by the authors for topic relevance and excluded if the publication was not related to BCVI or was non-original (eg, review articles).
Categorization
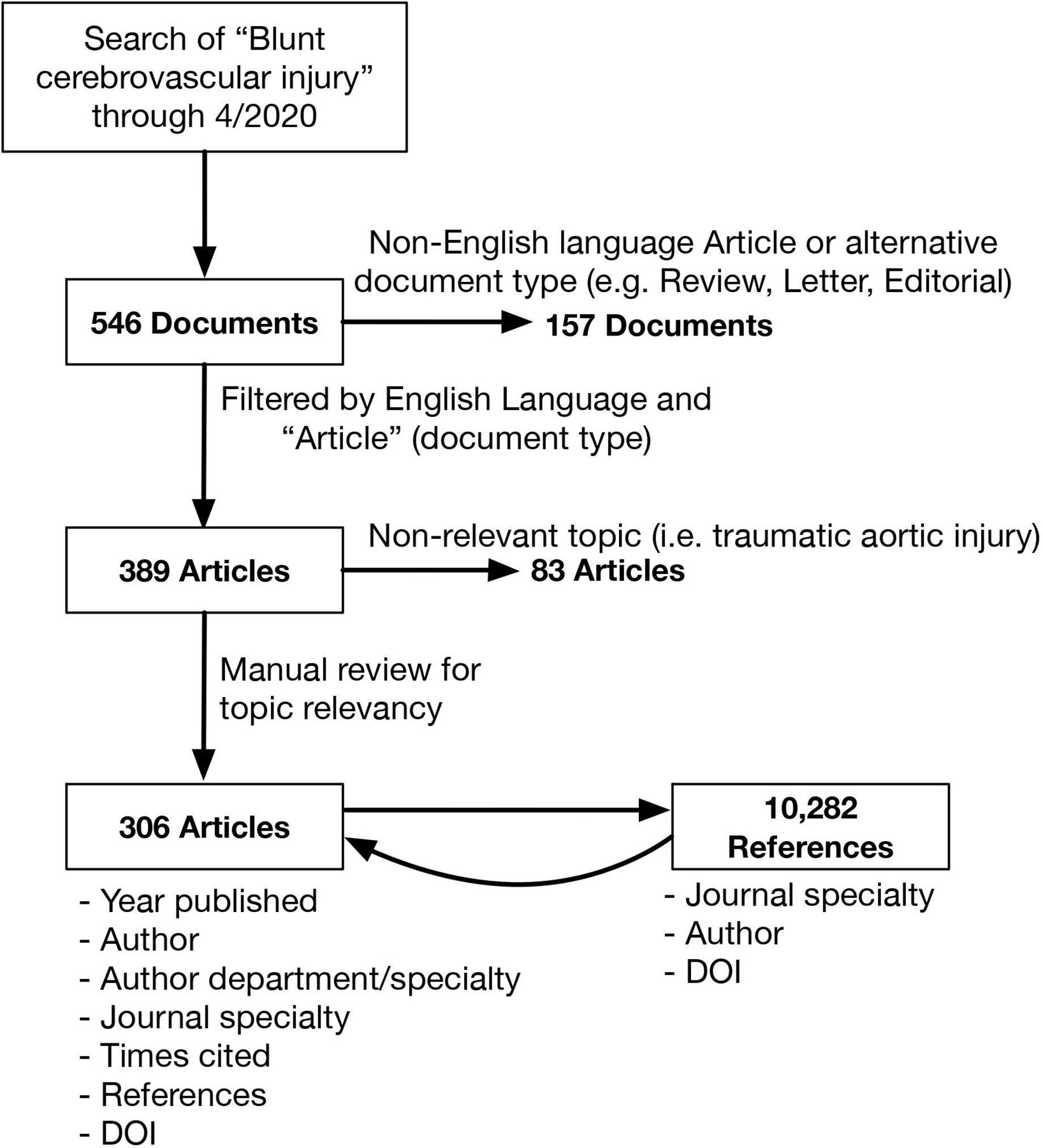
A total of 306 articles with 10 282 references were included for analysis (figure 1). An object-oriented programmatic script written in Python programming language was used to extract and categorize articles and references. All unique journal and cited references, with corrections for abbreviations or typography, were extracted and manually labeled as a neurosurgery, trauma, or ‘other’ journal. The addresses of all corresponding authors were searched, and departmental affiliation was used to determine primary author specialty, defined as neurosurgery author, trauma author, or ‘other’ author. Common ‘other’ specialty authors included radiology, neurology, and emergency medicine authors.

Flow chart demonstrating search and filtering methodology. DOI, digital object identifier.
Statistical analysis
On completion of a quality control programmatic run, the following variables were used for analysis from each article: published year, author, title, publishing journal, journal specialty, author specialty (based on department affiliation), times cited, total number of references, digital object identifier (DOI), number of each specialty’s references. Additionally, each BCVI article in the sample was searched for by DOI in the other BCVI references to build a network analysis and visualize topic reference patterns.
Analyses were performed using Stata V.14.2 (StataCorp). Two-sample t-tests, two-sample tests of proportions, and Pearson’s χ2 test were used to assess for significance.
Results
The initial search returned 546 articles on the topic of BCVI. After exclusions, 306 articles were included in the analysis. Of these, 24% (74) were published in neurosurgery journals, 45% (137) were published in trauma journals, and 31% (95) were published in a journal of another specialty. Similar proportions were found when reviewing author departmental affiliation. For the 306 BCVI articles, 20% (61) were written by authors based in a neurosurgery department, 42% (129) were written by authors affiliated with a trauma service, and 38% (116) were written by authors from a different department.
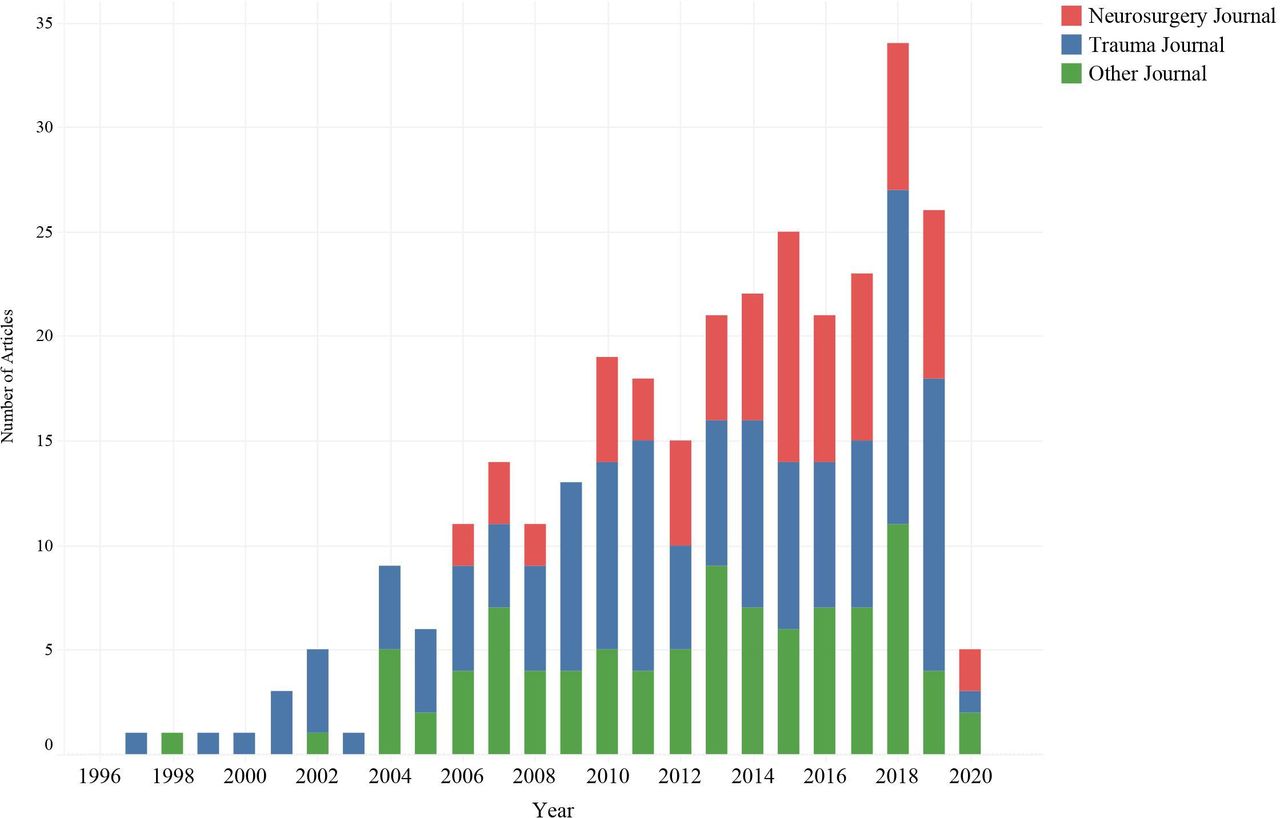
These proportions have not remained stable over time (figure 2). The earliest reports of BCVI in the peer-reviewed literature occurred in the late 1990s,16 17 primarily in trauma journals. The volume of reports on the topic has steadily grown since, and in 2006, the earliest articles were published in the neurosurgical literature,18 19 with steadily increasing number of subsequent reports in neurosurgical journals.

Bar graphs of number of blunt cerebrovascular injury (BCVI) articles published per year by each journal specialty.
Reference analysis
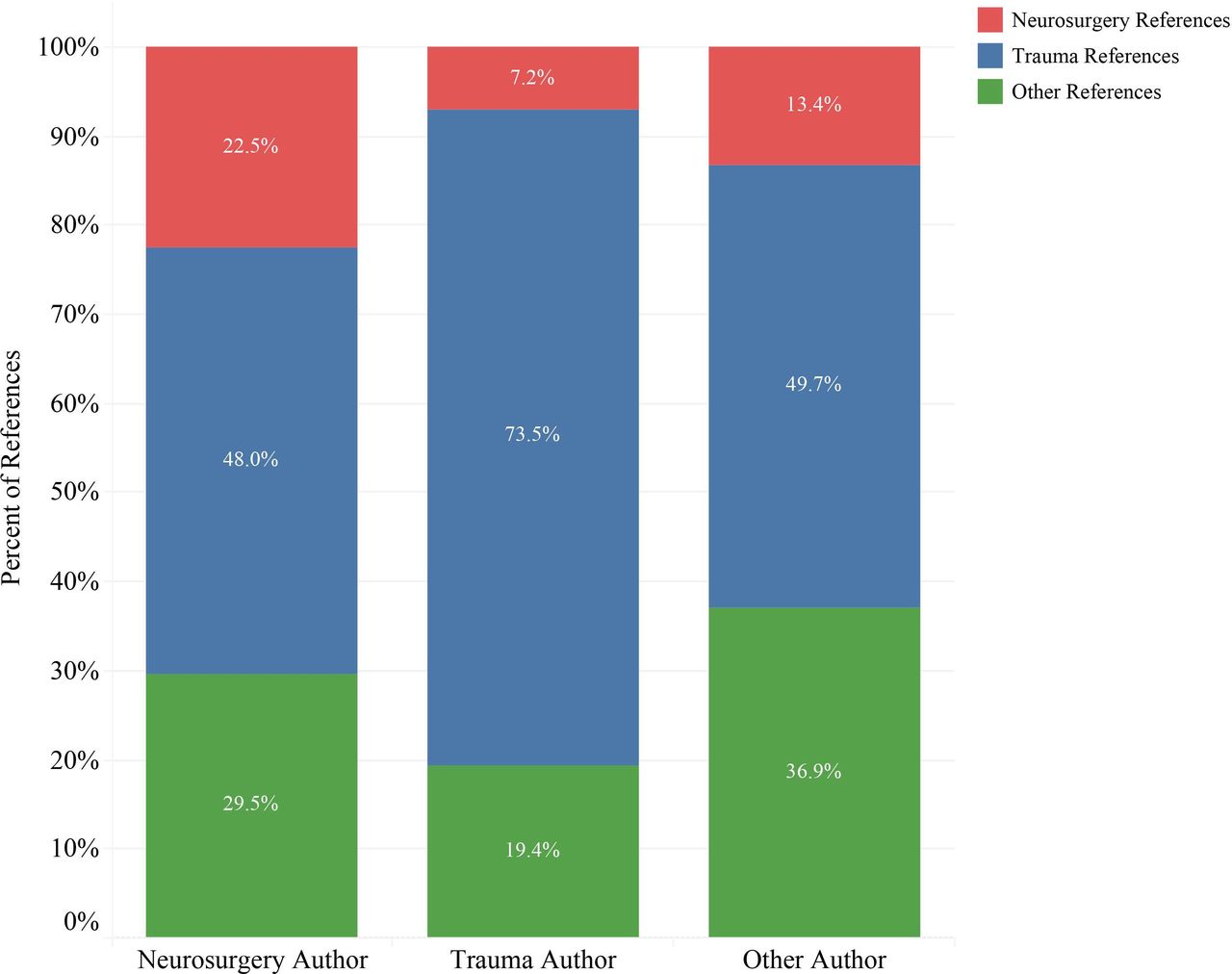
Comparing the citation patterns of authors from trauma and neurosurgery departments (figure 3), trauma surgery authors disproportionately referenced articles in the trauma literature, compared with neurosurgeons (73.5% vs. 48.0%, p<0.0001), and other authors. Neurosurgery authors referenced a higher percentage from neurosurgical journals (22.5% vs. 7.2%, p<0.0001) and ‘other’ journals (29.5% vs. 19.4%, p<0.0001) compared with trauma surgery authors.

Bar graph demonstrating specialty distribution of references by journal specialty.
While the majority of authors published in their own specialty’s journals (67% of neurosurgery authors in neurosurgery journals, 89% of trauma surgery authors in trauma journals), 12% of neurosurgery authored articles were published in trauma journals and 4% of trauma surgery authored articles appeared in neurosurgery journals. To further delineate the impact of author and journal specialty on references, the reference proportions for each author–journal combination were calculated and compared (figure 4).

Changes in specialty reference proportions with changes in author or journal specialty. Each corner represents a combination of author specialty (rectangle) and publishing journal specialty (oval) with average specialty reference proportions noted to the side. Along each arrow shows the change in average proportions of neurosurgery and trauma references from change of author or journal specialty.
This analysis demonstrated that the biggest factor influencing reference proportions was the specialty of the publishing journal. Trauma surgery authors publishing in trauma journals used a significantly larger share of trauma references (75.2% vs. 52.2%, p<0.0001) and smaller share of neurosurgery references (6.8% vs. 17.2%, p<0.0001) than when they published in neurosurgical journals. Similarly, neurosurgical authors publishing in trauma journals had a larger proportion of trauma references (68.0% vs. 48.3%, p=0.03) and smaller proportion of neurosurgical references (9.1% vs. 25.4%, p=0.02) than when publishing in neurosurgical journals. There was not a statistically significant difference in proportion of neurosurgery (p=0.2) or trauma references (p=0.7) when comparing trauma or neurosurgery authors publishing in neurosurgery journals, and no significant difference in proportion of neurosurgery (p=0.4) or trauma references (p=0.2) by author specialty published in trauma journals.
Network analysis
To further characterize how BCVI articles reference other articles on the same topic and the influence of journal specialty, the connections between articles within the BCVI sample were characterized and a network analysis was performed. Of the sample of 306 BCVI articles, 96% (293) cited another article in the sample. From 72 articles from neurosurgery journals, there were 792 references to other BCVI articles. 12.6% (91) were referencing articles in neurosurgery journals (NS-NS), 79.7% (577) were referencing a trauma journal article (NS-Trauma), and 7.7% (56) were referencing an article published in another specialty journal (NS-Other). For 131 BCVI articles in trauma journals, there were 1362 references to other articles in the sample. 1.5% (20) referenced a neurosurgery journal article (Trauma-NS), 93.1% (1268) referenced a trauma journal article (Trauma-Trauma), and 5.4% (74) referenced an article published in a different specialty’s journal (Trauma-Other). These differences in proportion of references within the BCVI sample were highly statistically significant between trauma and neurosurgery journal articles (p<0.0001).
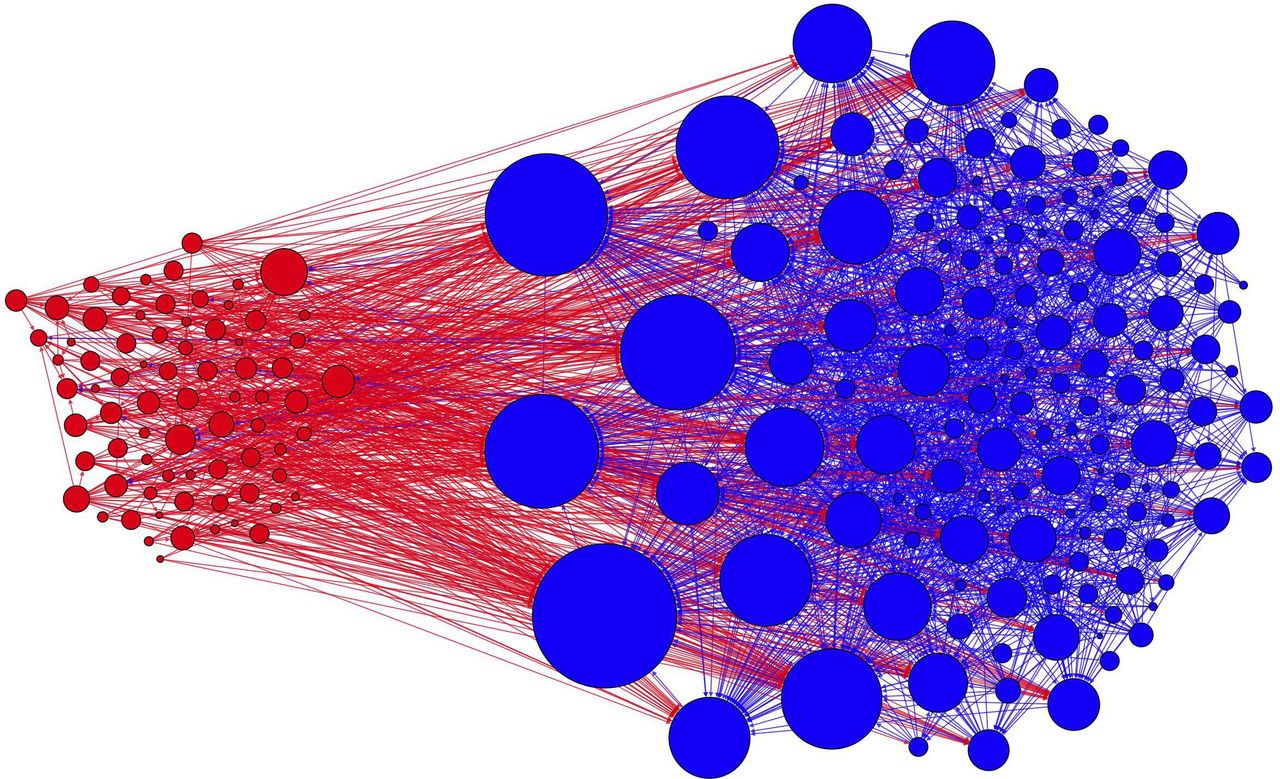
These differences in specialty reference patterns can be visualized when mapped into a network analysis, as seen in figure 5. Not only are there more trauma BCVI articles, there are more frequently cited trauma BCVI articles (larger circle indicates more citations). While both specialties have a high density of citations to articles of the same specialty (ie, red lines to red circles, and blue lines to blue circles), there are relatively few citations of neurosurgery journals by trauma articles (blue lines to red circles) but a large volume of neurosurgery citations to trauma articles (red lines to blue circles).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Network analysis of blunt cerebrovascular injury (BCVI) articles. Blue circles are articles in trauma journals (sorted to right) and red circles are articles in neurosurgery journals (sorted to left). Directional lines connecting each journal to a reference (color of line is based on the color of the referencing journal). Size of each circle is based on how many times it was cited, with larger circle indicating more citations.
Discussion
The trauma community deserves credit for the earliest recognition of BCVI as a significant source of disability in trauma patients. Their development of a classification scheme and screening criteria for BCVI heightened awareness and identification of patients at greatest risk, and established trauma surgeons as academic leaders in this field. As the clinical management of BCVI has evolved to adopt contributions from other specialties, the body of literature has seen an increase in peer-reviewed publications by authors from specialties such as neurosurgery, radiology, neurology, and emergency medicine (figure 2). In an ideal ‘knowledge sharing environment’, a proportional increase in citations of relevant studies on the same subject would be expected, independent of author subspecialty or journal affiliation. This has not occurred in the BCVI literature.
While the distribution of BCVI publications by journal affiliation has closely mirrored that of articles when classified by author departmental affiliation, this investigation revealed that trauma surgery authors have continued to disproportionately reference articles of their own specialty over time (figure 3). Not surprisingly, trauma remains the dominant specialty in publishing about BCVI and is heavily referenced by neurosurgery. But the lack of reciprocal referencing by trauma surgeons indicates a continued hesitancy to cite neurosurgery articles despite neurosurgery’s growing contributions to the field. Regardless of the cause, the existence of a one-way knowledge silo in the BCVI literature can be visualized with a network analysis of the literature (figure 5).
Several reasons may exist for this observed referencing bias. For example, the first reports from the trauma community16 17 on BCVI preceded those from neurosurgery by over a half decade.18 19 In the world of scientific research, this kind of unmatched temporal separation may be sufficient for a specialty to single handedly drive the growth of a given field of study. Indeed, the earliest and most impactful studies on BCVI were published by trauma surgeons during this time frame. Trauma surgeons have a long history of maintaining registries, which facilitate large-scale retrospective studies. In addition, at least in the USA, trauma surgery is usually the primary clinical service caring for patients with BCVI. This historical relationship between trauma surgery and consulting services, coupled with their dominance of BCVI research, creates the potential for a perceived sense of competition among the trauma community over other specialties. Another plausible explanation may be familiarity of authors with certain references. Authors tend to most frequently have access, be more familiar with, and best trust articles published by authors and journals of their own specialty. Separation of professional and scientific societies may also further insulate specialties from each other, preventing widespread distribution of information, and contribute to silo behavior. While these are all plausible theories behind the existence of silos in the BCVI literature, future research is needed to confirm the existence of silos in other areas of trauma research and to further quantify their resultant clinical impact.
A closer look, however, reveals that trauma and neurosurgery may not be acting wholly independently from one another and strongly suggests additional factors at play. While the existing number of cross-specialty BCVI peer-reviewed publications to date remains small, a comparison of citation proportions revealed a robust preference by these two specialties to cite trauma references when publishing in trauma journals. Unfortunately, one limitation of this study lies in the potential to miss jointly authored articles by both neurosurgeons and trauma surgeons, which is challenging given such data are not always available to export and analyze using our current methodology. But independent of specialty, authors publishing in trauma journals used a significantly larger share of trauma references and a smaller share of neurosurgery references than when publishing in neurosurgical journals. This observation may indicate a possible conscious curating of citations by authors to increase likelihood of publication in trauma and neurosurgery journals alike. Whether this behavior is driven by authors’ preferences or results from inherent specialty journal biases leading to barriers to publication is difficult to determine, but it serves to identify key areas for silo-busting interventions. Journal editors, peer reviewers, and readers should recognize the existence of knowledge silos and their potential impact, and actively foster diversity of citations and cross-specialty collaboration between trauma surgery and neurosurgery.
Conclusion
In this study, we quantitatively assessed knowledge sharing between trauma surgery and neurosurgery on the subject of BCVI. It has been previously recognized that the existence of knowledge silos in other fields of medicine hinders scientific advancement at the expense of quality and depth of medical research. Recognition and increased awareness of the existence of a knowledge silo in BCVI is the first important step in breaking down the barriers created by this observed segregation of specialties. More importantly, this investigation serves to identify potential silo-busting interventions, such as the need for an active role by journal editors, peer reviewers, and authors to actively foster diversity of citations and cross-specialty collaboration to improve dissemination of information between trauma surgery and neurosurgery.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors Conception and design: MRH. Literature search: GC, ZS, MRH. Data collection: GC, ZS. Data analysis: ZS. Data interpretation: all authors. Drafting of the article: GC, ZS. Critical revision of the article: MRH, JOJ. Reviewed the submitted version of the article: all authors. Approved the final version of the article on behalf of all authors: MRH. Administrative/technical/material support: JOJ, MRH. Study supervision: MRH. MRH is the guarantor and accepts responsibility for this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.