Article Text

Abstract
Background Although strokes are rare in trauma patients, they are associated with worse functional and cognitive outcomes and decreased mobility. Blunt cerebrovascular injury (BCVI)–related strokes and mortality have decreased, likely due to refined screening and treatment algorithms in trauma literature; however, there is a paucity of research addressing non-BCVI strokes in trauma. The purpose of this study is to evaluate the incidence, etiology, and risk factors of stroke in our trauma population in order to identify preventive strategies.
Methods This study was a retrospective review of all adult trauma patients admitted to a level 1 trauma hospital who suffered a stroke during trauma admission from 2010 to 2017. Data were collected from the prospectively maintained trauma and stroke databases. Stroke etiology was determined by a vascular neurologist.
Results Of the 43 674 adult trauma patients admitted during the study period, 99 (0.2%) were diagnosed with a stroke during the index admission. Twenty-one (21%) strokes were due to BCVI. Seventy-eight (79%) strokes were due to non-BCVI etiologies. Patients with non-BCVI strokes were older, less severely injured, and had more medical comorbidities compared with patients with a BCVI stroke. While patients with a BCVI stroke were more likely to suffer multiple traumatic injuries from MVC (76% vs 28%, p<0.001), non-BCVI strokes had more isolated extremity injuries from fall mechanism (55% vs 10%, p<0.001). Over the study period, the age and incidence of stroke and BCVI (p<0.001) increased. However, the rate of BCVI strokes decreased while the rate of non-BCVI strokes increased.
Discussion The incidence of stroke has increased despite aggressive screening and treatment of BCVI. This increase is primarily due to non-BCVI strokes which are associated with advanced age and medical comorbidities after low mechanism traumatic injury. Medical optimization of comorbid conditions during trauma hospitalization will become increasingly important for stroke prevention as the population ages.
Level of evidence: Level III
- stroke
- blunt trauma
- cerebrovascular injury
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Blunt cerebrovascular injuries (BCVIs) after trauma have traditionally been a rare diagnosis, occurring in 1%–2% of all blunt trauma patients. However, with expanded screening criteria and improved diagnostic modalities,1–11 the incidence of BCVI has increased over the past three decades.12 Despite this increase, BCVI-related strokes and mortality have decreased,12 likely as a result of both improved diagnostic and treatment algorithms.12–15
Although strokes are rare after trauma, they can have significant short and long-term impact on functional and cognitive status. In a study from the Netherlands, Hundersmarck et al demonstrated that patients with BCVIs have worse long-term functional outcomes than those in the general trauma population.16 In addition, patients with BCVI and ischemic stroke had worse long-term outcomes in terms of mobility and self-care than patients with BCVI alone. Patients with BCVI and traumatic brain injury had worse cognitive outcomes. Shahan et al demonstrated that stroke, along with age, predicts decreased mobility after BCVI and that the occurrence of stroke predicts decreased activity and cognitive function.17 Given the association of BCVIs with traumatic brain injury, functional and cognitive impairment may be further exacerbated in the elderly in whom falls are common.
Although screening for BCVIs has traditionally been reserved for patients with high-energy mechanisms, recent studies have reported a higher-than-expected incidence in elderly patients (≥65) who were screened after low-energy mechanisms such as falls.18 19 In addition to BCVI being a known risk factor for ischemic strokes, elderly patients often have additional predisposing comorbidities such as atrial fibrillation, diabetes, hypertension, and atherosclerotic disease such as carotid artery stenosis.20–23 Given that the US population is aging rapidly,20 there has been an increased focus on the management and outcomes of trauma patients who are older or have multiple comorbidities. However, little is known regarding the incidence of BCVI-related versus non-BCVI-related strokes and their outcomes, particularly in elderly patients.
The purpose of this study is to evaluate the incidence over time, etiology, risk factors, and in-hospital outcomes of strokes in a trauma population cared for at a high-volume level 1 trauma center. The primary hypothesis of the study is that elderly trauma patients are more likely to have non-BCVI-related strokes than BCVI strokes. The implication is that stroke prevention in trauma patients will require additional interventions beyond early diagnosis and treatment of BCVIs.
Methods
Study setting
The Red Duke Trauma Institute (RDTI) at Memorial Hermann Hospital (MHH) is an American College of Surgeons–verified Level 1 trauma center in Houston, Texas and serves as the primary teaching facility for McGovern Medical School at UT Houston. The RDTI treats over 7500 trauma patients per year and has approximately 5000 adult trauma admissions per year.
Selection of participants
After obtaining Institutional Review Board approval, a single-center retrospective study was performed using electronic medical records and the prospectively maintained trauma and stroke registries from MHH. All adult (≥16 years of age) trauma patients diagnosed with a stroke during the index trauma admission between January 2010 and December 2017 were included in this study.
Definitions
A BCVI-related stroke was defined as an ischemic stroke in the vascular distribution of the BCVI. Non-BCVI-related strokes were defined as ischemic strokes in the absence of BCVI or ischemic strokes in a vascular distribution not consistent with the BCVI. Adjudication was performed by a stroke neurologist not involved in the care of the patient who reviewed the imaging reports and studies. Time of CT angiography (CTA) neck acquisition was used as time of BCVI diagnosis. Time of treatment was the time of receipt of initial antithrombotic or therapeutic anticoagulation medication. Time of stroke was the time of radiographic diagnosis of stroke with either CT or MRI brain. Death was classified as stroke-related based on divisional mortality review forms and independent clinical review.
The etiology of ischemic strokes were classified based on the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) stroke subtype classification system.24 The TOAST classification system classifies ischemic stroke based on the major pathophysiologic mechanisms and includes five categories: large artery atherosclerosis, cardioembolic, small vessel occlusion, stroke of other determined etiology, and stroke of undetermined etiology. Undetermined etiology includes patients with a negative evaluation, an incomplete evaluation, or with two or more potential causes identified. A vascular neurologist not involved in the care of the patient classified all of the strokes using the TOAST classification system.
Statistical analysis
A two-piece linear trend line was used to model the incidence rates of BCVI and strokes, including BCVI-related and non-BCVI-related strokes between 2011 and 2017. Significance for a trend was evaluated by the Wald test on zero slope, while the Jonckheere-Terpstra test was used to evaluate trends in age. Continuous characteristics were summarized as median and IQR. Association with type of stroke was evaluated by Wilcoxon rank-sum test and Fisher’s exact test for continuous and categorical characteristics, respectively. Mortality rates and proportions of death due to stroke of BCVI and non-BCVI stroke were evaluated by both risk difference and relative risk. Relative risk is calculated as ratio of two proportions. We conducted the Wald tests to compare two proportions and test the relative risk equal to 1. We reported two-sided p values and p values less than 0.05 were considered as significant. All statistical analyses were performed using the SAS software (V.9.4; SAS Institute, Cary, NC).
Results
Incidence
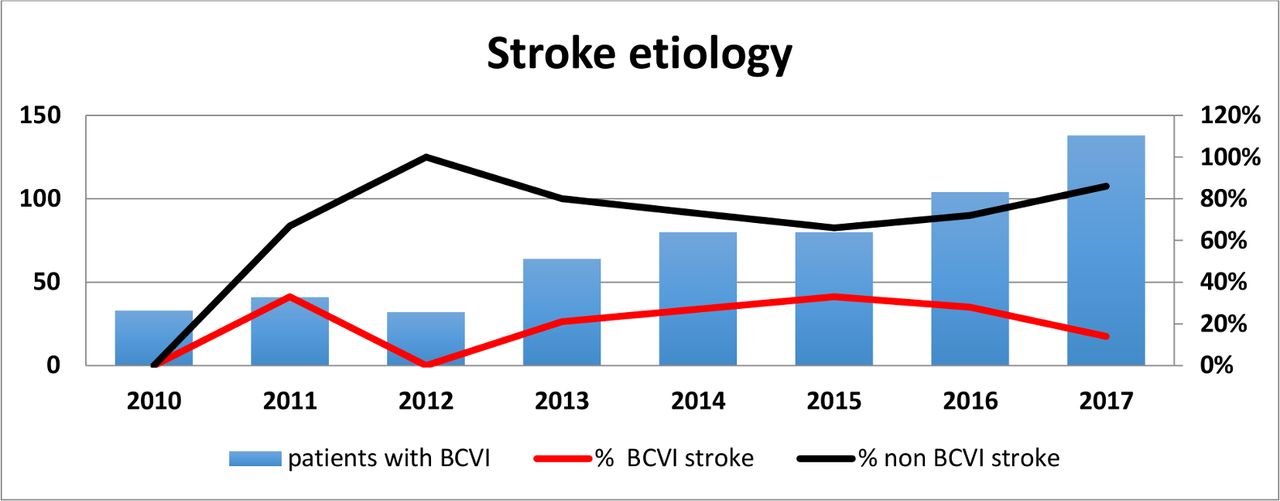
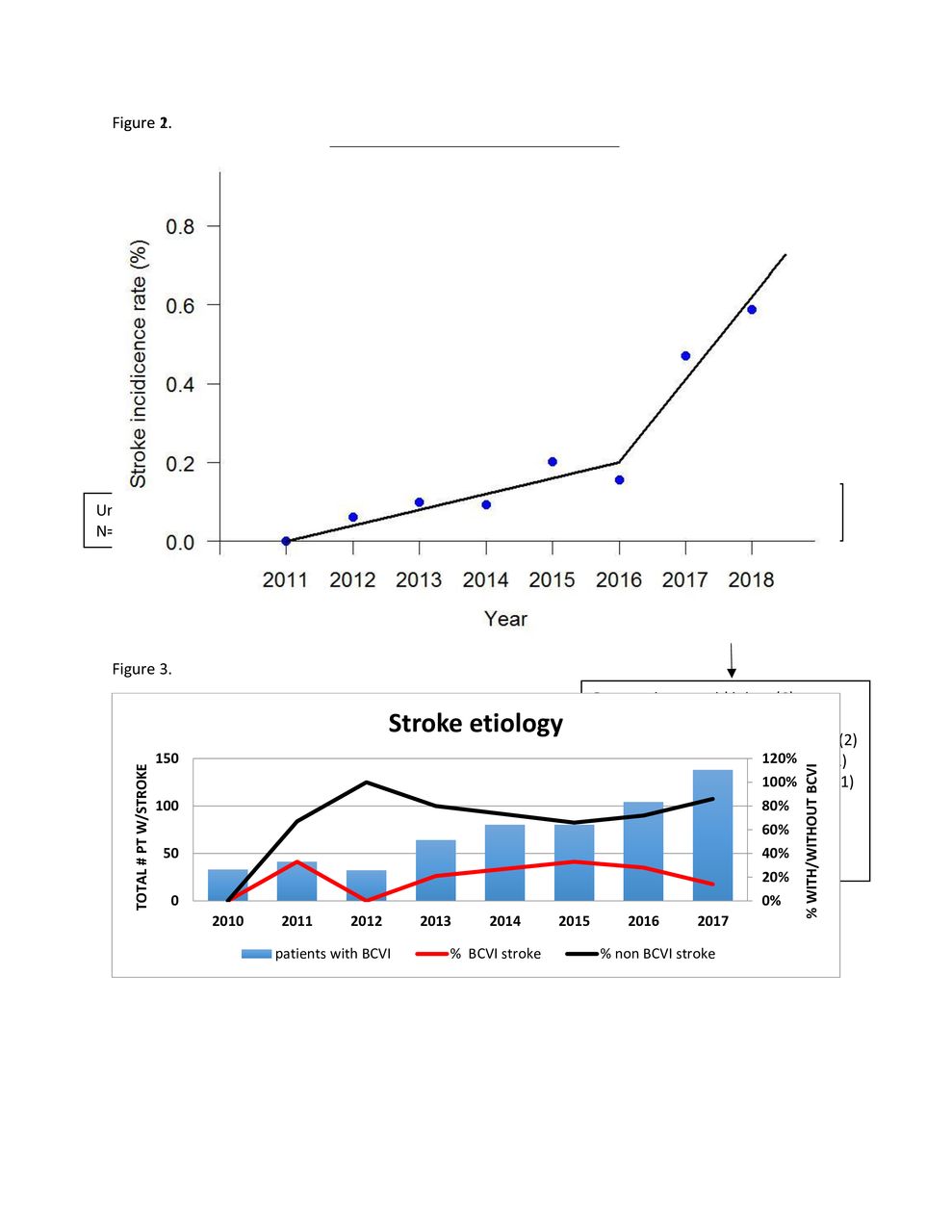
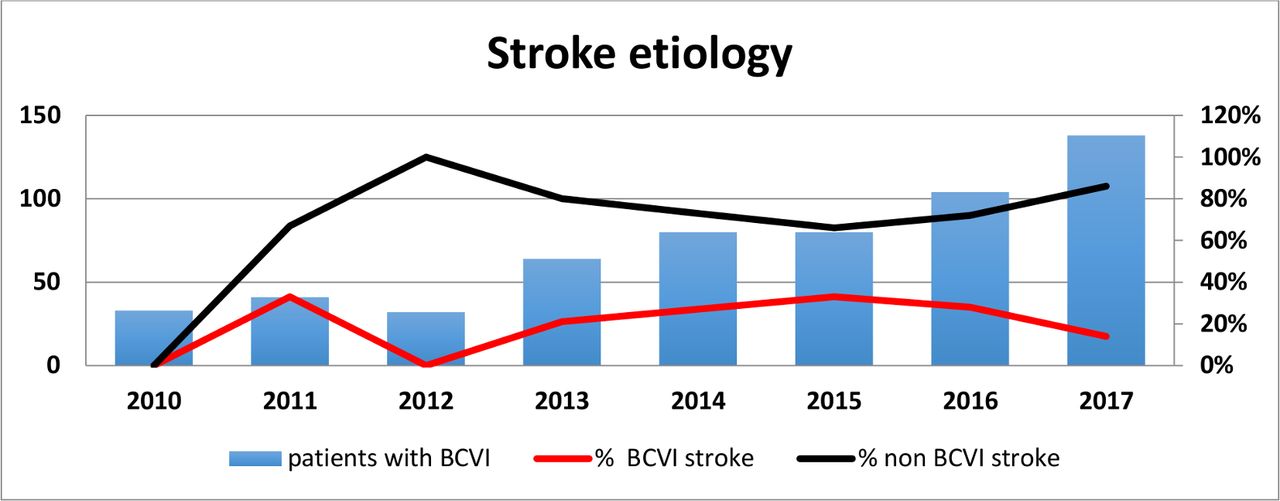
Of the 43 674 adult trauma patients admitted during the study period, 99 (0.2%) were diagnosed with an ischemic stroke during the index admission, of which only 21% were BCVI related (figure 1). The incidence of both BCVI and stroke, regardless of etiology, increased during the 7-year study period (figure 2). However, the incidence of BCVI-related stroke decreased while that of non-BCVI-related stroke increased (figure 3). The number of screening neck CTA studies also increased as a result of revisions to our BCVI screening criteria with 12.8% of patients receiving screening neck CTA compared with 5.5% at the beginning of the study period. The median age of adult trauma patients also increased from 41 to 46. All of these trends were statistically significant (p<0.001).

Consort diagram.

Incidence of stroke over time.
{kind=link}
{kind=link}
{kind=link}
Etiology of stroke over time.
Etiology
The majority (78/99, 78%) of strokes were non-BCVI related. Using the TOAST classification system, the etiologies of these strokes included, in descending order of frequency, cardioembolic (41%), other determined etiology (26%), undetermined etiology (13%), large artery atherosclerosis (11%), and small vessel occlusion (9%).
Risk factors
The BCVI-related stroke group were significantly younger than the non-BCVI-related stroke group. They also had a significantly higher median injury severity score (ISS), higher abbreviated injury scale (AIS) head, and lower Glasgow Coma Scale (GCS) score in the emergency department (table 1). Motor vehicle collisions were the most common mechanism of injury in the BCVI-related stroke group while ground level fall predominated in the non-BCVI stroke group. While patients with BCVI-related stroke were more likely to suffer multiple traumatic injuries from MVC, non-BCVI strokes had more isolated extremity injuries from fall mechanism.
Baseline data for BCVI and non-BCVI stroke
The non-BCVI-related stroke group was older and more frequently had pre-existing medical comorbidities, especially atrial fibrillation and prior stroke or transient ischemic attack. Twelve of the 32 patients with a cardioembolic stroke had pre-existing atrial fibrillation: five patients had a stroke present on admission, three suffered a stroke while holding anticoagulants for surgery, two were taking no anticoagulants, and two suffered a stroke despite continuing aspirin. More patients with non-BCVI-related stroke were taking antiplatelet or anticoagulant medications, although this difference was not statistically significant.
Management of BCVIs
The median time from ED arrival to stroke diagnosis was similar for BCVI-related and non-BCVI-related strokes (table 2). Also, 95% of patients with BCVI received treatment with aspirin or heparin infusion. While the median time to diagnosis of BCVI was only 1.4 hours, the median time of treatment initiation was 15 hours after the diagnosis. Eleven of the 21 patients with BCVI had a traumatic brain injury or solid-organ injury which contributed to the delay in starting antithrombotic therapy. Ischemic stroke was diagnosed in 10 patients prior to initiation of antithrombotic therapy (five patients with severe traumatic brain injury and five suffered a stroke prior to arrival to the ED) and 11 patients despite treatment of BCVI. Median time to stroke diagnosis was 44 hours after ED arrival with five patients diagnosed with stroke at time of arrival to the emergency center, resulting in a 24% non-preventable BCVI stroke rate.
Outcomes data for BCVI and non-BCVI stroke
Outcomes
Despite the non-BCVI-related stroke group having less severe injuries, the hospital length of stay, ICU length of stay, and number of ventilator days were similar to those in the BCVI-stroke group (table 2). The mortality rate for BCVI strokes and non-BCVI strokes were 38% and 22%, respectively, and patients with BCVI strokes were 1.7 times more likely to die in the hospital than those with non-BCVI strokes (relative risk (RR) 1.75, 95% CI 0.88 to 3.48, p=0.11). Of the patients who died, death was the direct result of the stroke more frequently in the BCVI group (75%) than the non-BCVI group (53%) (RR 1.42, 95% CI 0.78 to 2.58, p=0.26).
Discussion
In this single-center study, ischemic strokes were rare with an incidence of 0.2% in an adult trauma inpatient population. Although low, the incidence has increased over the past 5 years, corresponding with an increasingly older population. The majority of strokes were not caused by BCVI but instead occurred in elderly patients with medical comorbidities and isolated extremity injuries from ground level fall. Only one of every five ischemic strokes were BCVI related, and one out of four of those were present on admission and thus non-preventable. These findings have important implications on strategies to mitigate stroke risk.
For BCVI-related strokes, best practice includes following evidence-based screening guidelines for early BCVI diagnosis and treatment with antithrombotic therapy. At our institution, criteria for obtaining CTA to screen for BCVI have been in place since 2003 and were expanded in 2014 (box 1). As a result of the expansion of screening criteria, there was a significant increase in the number of CTA neck studies and a subsequent increase in BCVI diagnosis. The evidence-based management algorithm includes initiation of either aspirin or low-dose heparin infusion as soon as possible. Similar to the results reported by Shahan et al,12 this study demonstrates that aggressive screening for BCVI was associated with an increased incidence of BCVI. More importantly, there was a decreased risk of stroke among the entire trauma cohort. The increased BCVI incidence corresponds with changes to our evidence-based guidelines for diagnosis and treatment of BCVI.25 Nonetheless, despite aggressive screening for BCVI, some strokes remained non-preventable such as those with stroke present on arrival or patients with severe traumatic brain injury and contraindication to immediate BCVI treatment.
Screening criteria* for BCVI
Injury patterns
Complex facial fractures (LeFort II or III).
Mandible fracture.
Basilar skull fracture or occipital condyle fracture.
Cervical vertebral body or transverse foramen fracture at any level (C1–7).
Any fracture at level C1–C3.
Cervical subluxation or ligamentous injury at any level.
Severe traumatic brain injury (TBI) with GCS score <6.
Near hanging with anoxic brain injury.
Seatbelt or other clothesline-type injury with significant swelling, pain or AMS (Altered Mental Status).
Combined TBI and major thoracic injury.
Scalp degloving injury.
Thoracic vascular injury.
Signs and symptoms
Potential arterial hemorrhage from neck/nose/mouth.
Cervical bruit in patient <50 years of age.
Cervical hematoma.
Focal neurologic defect: TIA, hemiparesis, vertebrobasilar symptoms, Horner’s syndrome.
Neurologic deficit inconsistent with head CT.
Stroke on CT or MRI.
*The screening criteria are an adaptation of the expanded Denver criteria based on literature review and group consensus.
For non-BCVI-related strokes, further studies are needed to identify high-risk elderly trauma patients and modifiable risk factors in order to focus efforts on stroke prevention. One potentially modifiable risk factor is occult hypoperfusion which is prevalent in the elderly population and associated with increased morbidity and mortality following trauma.26 27 Further study is necessary to determine the impact of early recognition and treatment of occult hypoperfusion on complications such as ischemic stroke.
The majority of strokes in this study were not BCVI related and occurred in patients with advanced age and medical comorbidities. The non-BCVI strokes occurred in elderly patients who were more likely to suffer an isolated extremity injury from a low mechanism of injury such as ground level fall. This observation has important implications regarding service admission patterns (non-surgical service vs trauma surgery) and the importance of optimization of these high-risk but low-acuity trauma patients. Regardless of admitting service, elderly patients may benefit from a comprehensive geriatric assessment, or an interdisciplinary approach to assessing and treating frail older patients’ medical, psychosocial, and functional limitations.28 29 A recent systematic review of models of care for geriatric hip fracture patients demonstrated that patients under the care of a coordinated orthogeriatrics model or a geriatrics-led model had a shorter time to surgery, decreased length of stay, and reduced postoperative mortality rates.30 A similar interdisciplinary approach has been demonstrated to reduce 30-day readmissions in a more diverse older trauma patient population.31 Whether such interdisciplinary care is achieved through geriatric consultation or development of a specialized geriatric trauma service with evidence-based protocols is dependent on each hospital’s resources and surgeons’ preferences.
This study has several limitations based on its retrospective design. Data were collected from the medical record, trauma registry, and stroke registry, which are only as accurate as documentation and data entry. The study did not include long-term follow-up data and included strokes occurring during the index hospital admission—not after discharge. Another limitation of the study is that there may be unmeasured confounders that affect the development of stroke.
Finally, since data were not collected on management of all patients with BCVI, the decreased stroke rate in patients with BCVI cannot be directly attributed to the evidence-based management of these patients.
Conclusion
The incidence of stroke has increased over time at a large level 1 trauma center with aggressive BCVI screening and management protocols. The low number of BCVI-related strokes supports the practice of early identification and treatment of BCVIs. In addition, the increase in non-BCVI-related strokes in elderly patients with isolated extremity injuries secondary to ground level fall suggests the need to focus future efforts on managing medical comorbidities of an increasingly aging trauma population. Strategies to mitigate non-BCVI-related strokes should focus on optimizing medical conditions such as through early identification and treatment of occult hypoperfusion or through development of multidisciplinary geriatric protocols and services. Understanding of the incidence and etiology of strokes in trauma patients is necessary to guide future improvement efforts.
References
Footnotes
Contributors MKM, SIS, CEW, and LSK made substantial contributions to the conception and design of study. MKM, CS, DR, HKRI, XZ, BAC, and LSK made substantial contributions to the acquisition, analysis, and interpretation of the data. MKM wrote the manuscript. BAC, JH, CEW, SIS, and LSK performed critical revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The protocol was approved by the Institutional Review Board (IRB) at the University of Texas Health Science Center (HSC-GEN-13_0325). As this was a retrospective study, the consent by the subjects was not required by the IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplementary information. Data will be made available under a Data Use Agreement through the University of Texas McGovern Medical School.