Article Text

Abstract
Background As a result of improvements in the early resuscitation phase of trauma, mortality is largely driven by later mortality due to multiple organ dysfunction syndrome (MODS), which may be mediated by an early overdrive in the host immune response. If patients at risk for MODS could be identified early, preventive treatment measures could be taken. The aim of this study is to investigate whether specific biomarkers are associated with MODS.
Methods Multiple trauma patients presenting to the Amsterdam University Medical Centers, location Academic Medical Center, between 2012 and 2018 with an Injury Severity Score of 16 or higher were sampled on arrival at the emergency department. A wide variety of inflammatory cytokines, endothelial and lung-specific markers were determined. Comparisons were made between patients with and without MODS. Univariate and multivariate logistic regression was used to determine associations between specific biomarkers and MODS. A p value of 0.05 was considered to be statistically significant.
Results In total, 147 multiple trauma patients were included. Of these, 32 patients developed MODS (21.7%). Patients who developed MODS were more severely injured, had more traumatic brain injury and showed more deranged markers of coagulation when compared with patients without MODS. Overall, both proinflammatory and anti-inflammatory cytokines were higher in patients with MODS, indicative of a host immune reaction. In the multivariate analysis, the combination of anti-inflammatory proteins interleukin 1 receptor antagonist (IL-1RA) (OR 1.27 (1.07–1.51), p=0.002) and Clara cell protein 16 (CC-16) (1.06 (1.01–1.05), p=0.031) was most strongly associated with the development MODS.
Conclusions In trauma, anti-inflammatory proteins IL-1RA and CC-16 have the potential to early identify patients at risk for development of MODS. Further research is warranted to prospectively validate these results.
Level of evidence Prognostic study, level III.
- trauma
- biomarkers
- ARDS
- AKI
- MODS
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Improvements in the management of major bleeding have led to shifts in morbidity and mortality towards later stages in the course of trauma.1 2 These improvements in early trauma survival result in an increase in patients prone to develop inflammatory complications later in time, such as acute respiratory distress syndrome (ARDS), acute kidney injury (AKI) and multiple organ dysfunction syndrome (MODS).1 3–7 These complications all contribute to late mortality, which is around 20% to 30% in multiple trauma patients.1 2 It is hypothesized that the development of organ failure is mediated by an augmented immune response to damage-associated molecular patterns, which are released from tissues in large amounts after trauma, leading to MODS.8–12 Multiple different pathways, including inflammation, coagulation and endothelial activation, are involved in the progression of MODS.13 14 Previous studies using biomarkers to predict ARDS in trauma have shown that both epithelial and endothelial markers are involved.15 16 For example, Clara cell protein 16 (CC-16), which is an anti-inflammatory pulmonary secretory protein,17 18 and angiopoietin-2, a marker of endothelial activation, were increased in patients with ARDS compared with patients without ARDS.16 Other markers of endothelial activation include thrombomodulin-1 and syndecan-1, which are increased in patients developing MODS already prior to hospital arrival.14 Moreover, a study evaluating biomarkers in the progression of AKI after trauma showed an early increase in interleukin 1 receptor antagonist (IL-1RA), indicating an upregulation in blocking of interleukin 1 pathways.19 Another study evaluating the prehospital immune response showed potential relationships between both immune activation and suppression in patients with MODS, underlining the multifactorial process.20 Additionally, evaluation of immune cell genes revealed a specific upregulation of pathways associated with cell death and a hyperacute innate immune response.13
Currently, however, it is unclear which markers from these different inflammatory pathways, endothelial activation pathways and/or lung-specific damage markers are most strongly correlated with the development of organ failure.21–23 If early measured biomarkers are associated with MODS, early targeted treatment strategies could be initiated.
The aim of this study was to identify biomarkers of inflammation, endothelial activation and markers related to lung-specific damage early in the course of trauma and investigate which of these biomarkers were most strongly associated with the development of MODS.
Methods
Study participants
This cross-sectional study was conducted as a substudy of the observational prospective cohort study ‘Activation of Coagulation and Inflammation in Trauma-3 (ACIT-3)’.24
Patients from 2012 to 2018 admitted to the level 1 trauma unit were eligible for inclusion. Inclusion criteria were adult (18 years or older) patients suffering from blunt or penetrating trauma with vital signs indicative of shock (e.g. heart rate of 120 bpm or more, systolic blood pressure of 90 mmHg or less, or estimated blood loss >500 mL) or suspicion of one of the following clinical diagnoses: femur fracture, multiple rib fractures, pneumothorax, severe abdominal injury or pelvic fractures. Exclusion criteria were transferal from another hospital, presentation longer than 120 minutes after trauma, receipt of more than 2000 mL of crystalloids infusion prior to admission, burn injury of more than 5% of their body surface, use of anticoagulant medication, known bleeding diathesis or known liver disease (Child-Pugh classification B or C).
Baseline hemodynamic vital variables were recorded. Traumatic brain injury (TBI) was scored as a head abbreviated Injury Severity Score (ISS) of 3 or more. Blood gas analysis and laboratory tests were assessed.
In this substudy, patients who had an injury severity (ISS) of 16 or higher were selected. Patients were further subdivided into patients with and without MODS.
Outcome parameters
ARDS was diagnosed according to the Berlin criteria.25–27 Patients with AKI stage I, II or III, as determined using the RIFLE criteria (acronym for Risk of renal dysfunction, Injury to the kidney, Failure of kidney function, Loss of kidney function and End-stage kidney disease), were scored.28 29 MODS was defined by sequential organ failure assessment score of 3 or higher in two or more organ systems, scored from 48 hours after trauma onwards. Furthermore, ventilator-days, intensive care stay, total length of stay in hospital and early (24 hours) and late mortality (30 days) were recorded.
Laboratory analysis of biomarkers
Whole blood was collected in EDTA tubes at trauma presentation in the emergency department (ED). Plasma was prepared with a single centrifugation step (1750G, 10 minutes, 18°C, Eppendorf 5804R). The upper two-thirds of the plasma was collected and stored at −80°C for later analysis. Plasma samples were assessed using a multianalyte luminex kit (R&D Systems, Minneapolis, USA), consisting of the following biomarkers: myeloperoxidase (MPO), tumor necrosis factor-α (TNF-α), TNF-α receptor 1 and 2 (TNF-R1 and TNF-R2), interleukin 6 (IL-6), interleukin 8 (IL-8), receptor for advanced glycation end-products (RAGE), first apoptosis signal (FAS) ligand, surfactant protein D (SP-D), Krebs von den Lungen-6 (KL-6), IL-1RA, interleukin 10 (IL-10), macrophage migration inhibitory factor-1α (MIF-1α), CC-16, E-selectin, tissue factor (TF), intercellular adhesion molecule 1 (ICAM-1), vascular cellular adhesion molecule 1 (VCAM-1) and plasminogen antigen inhibitor 1 (PAI-1). This panel was chosen based on previous literature on inflammation,19 30 31 endotheliopathy14 and lung-specific complications16 in trauma.
Statistical analysis
Statistical analysis was done using SPSS Statistics V.25 (IBM), graphs were made employing PRISM V.8 (GraphPad, California, USA). Values of biomarkers below the detection value were rated as half of the lowest detectable value.32
Normality was checked using Kolmogorov-Smirnov test and visual assessment of histograms. For normal distributed data, Student’s t-test was used, and a Mann-Whitney U test was used for non-parametric data. χ2 test or Fisher’s exact test was used to detect differences between proportions.
After assessing the association between potential biomarkers and MODS, a univariate logistic regression was made using each biomarker independently. Biomarkers with p value <0.10 were further evaluated in the multivariate regression analysis using forward selection. A maximum of three association measures was used in the final multivariate regression analysis.33
Receiver operating curves were made to visualize the potential sensitivity and specificity of biomarkers. The combined estimate was calculated using the estimate calculation from the multivariate regression analysis. A p value <0.05 was considered to be statistically significant.
Results
Baseline characteristics
In total, 189 patients with an ISS of 16 or higher were included in ACIT trial between 2012 and 2018. Of the 189 patients, 42 were retrospectively excluded in this substudy based on: no informed consent obtained (n=33), anticoagulant medication use (n=4), time from hospital to admission longer than 2 hours (n=3), and burn injury of more than 5% of body surface (n=2). The baseline characteristics of the included patients (n=147) are shown in table 1. 21.7% of patients developed MODS, with a median time to development of 3 days. The most prevalent complication was AKI (13.6%) followed by ARDS (6.8%). Patients with MODS had significantly higher ISS compared with patients without MODS, more often had brain injury, had a higher base deficit on arrival and had more deranged coagulation parameters. As expected, patients with MODS had longer intensive care unit and hospital stay than patients without MODS. As patients need to survive the initial hit of trauma, early mortality occurred only in patients without MODS and was related either to TBI (80.0%) or exsanguination (20.0%). Reasons for late mortality included severe TBI (58.3%), severe organ failure (25.0%), circulatory collapse (8.3%) and psychiatric condition leading to suicide (8.3%). In patients who survived the first 24 hours but died within 30 days, mortality occurred after a median of 7.5 days.
Baseline characteristics
Biomarkers are associated with multiple organ failure
Patients who developed MODS had significantly higher baseline levels of proinflammatory cytokines (IL-6, IL-8, TNF-R1, FAS ligand, RAGE and MPO) than patients without MODS. Also, higher levels of baseline IL-1RA were seen in patients with MODS compared with patients without MODS (table 2), indicative of an elevated anti-inflammatory response.
Panel of systemic and lung proinflammatory and anti-inflammatory, endothelial and coagulation biomarkers
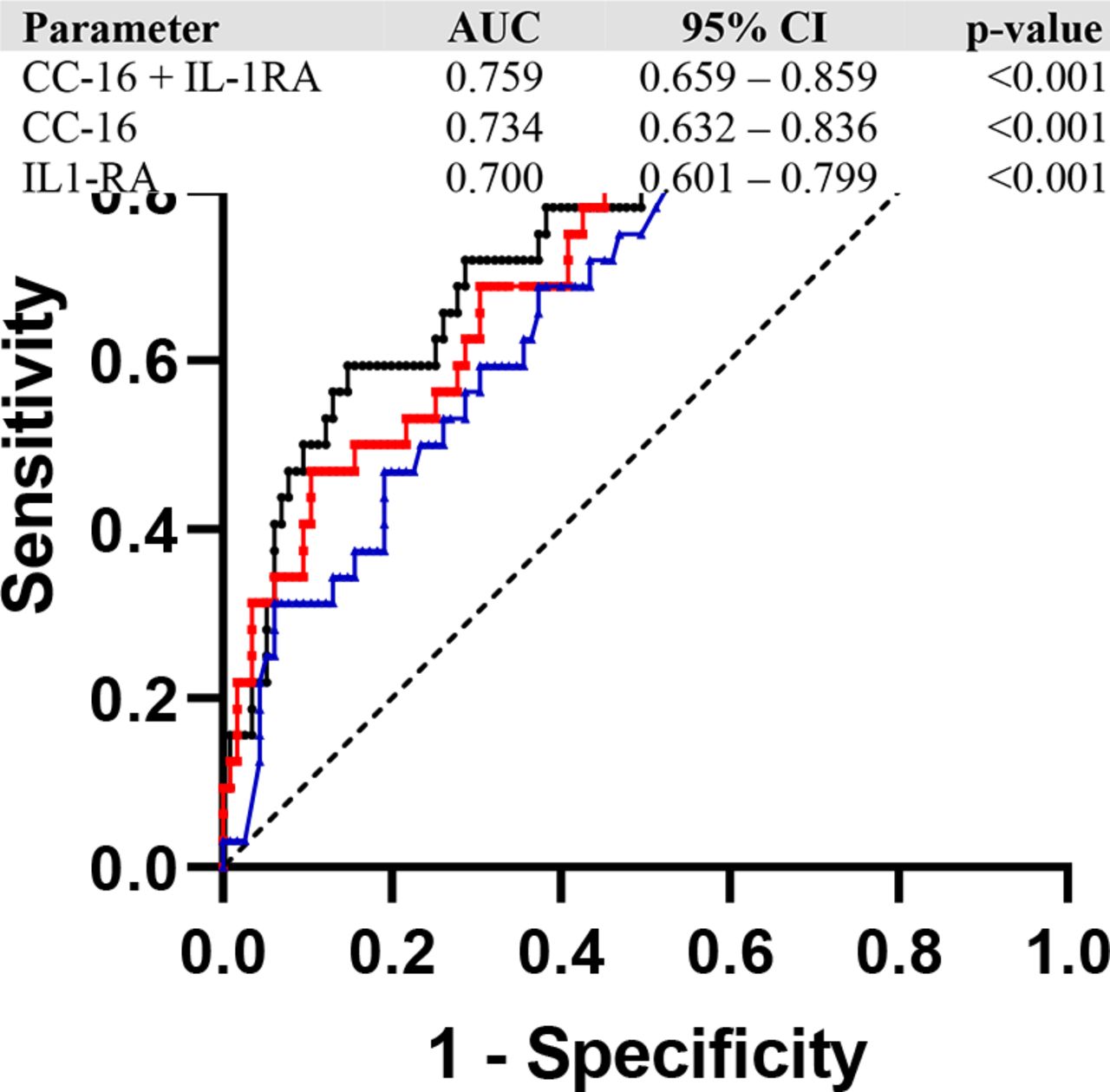
Baseline endothelial markers such as TF, ICAM-1, VCAM-1 and E-selectin did not differ between groups (table 2). CC-16, but not other lung-specific markers, was significantly higher in patients developing MODS compared with patients without MODS. In the univariate analysis IL-1RA and CC-16 were most strongly associated with the development of MODS (table 3). This association remained after correcting for injury severity. Receiver operating characteristic curve revealed fairly good prediction of MODS using CC-16 (area under the curve (AUC) 0.70), IL-1RA (AUC 0.73) and a two-biomarker model (AUC 0.76) (figure 1).
Increased levels of IL-1RA and CC-16 are associated with MODS
{kind=link}
Receiver operating characteristic (ROC) curve of a single and two-biomarker model. Receiver-operator curve with CC-16, IL-1RA and a logistic estimate of these two biomarkers combined. AUC, area under the curve; CC-16, Clara cell protein 16; IL-1RA, interleukin 1 receptor antagonist.
Discussion
The aim of this study was to examine the potential prognostic properties of plasma biomarkers to identify patients at risk for development of MODS after trauma. In this cohort of severely injured patients, 21.7% developed MODS. An early increase in anti-inflammatory proteins IL-1RA and CC-16 at presentation to the ED was associated with the development of MODS after 3 days, which was independent of the ISS.
In this study, proinflammatory cytokines were higher in patients with MODS compared with patients without MODS, but these were not independently associated with development of MODS. The strongest association was found with the anti-inflammatory biomarker IL-1RA. Previous studies have shown a profound immune cell activation in trauma with components of activation and suppression, occurring already at ED presentation.20 This suppression of immune cells after trauma, depicted by lower cytokine production, was also present in this cohort. Previously, we showed that the ex vivo ability of these trauma patients to generate an immune response to lipopolysaccharide stimulation was impaired when compared with healthy volunteers.34 Also, trauma patients have lower expressions of monocyte toll-like receptors compared to healthy volunteers.35 Furthermore, underlining these results, a study performed in 166 polytrauma patients revealed a similar pattern of early IL-10 release and a decrease in human leukocyte antigen—DR isotype expression, potentially reducing macrophage functions.36 Additionally, although based on a small number of patients (n=44), major trauma was associated with an impairment of neutrophil function.37 Interestingly, in mice with TBI and tibia fracture receiving IL-1RA treatment, a decrease in neutrophil activation markers and cerebral edema was seen.38 The exact mechanism of immune paralysis directly after trauma is poorly understood. Our results suggest that IL-1RA might play a role in the progression of MODS.
In line with this, we found that CC-16 levels in patients with MODS were higher compared with patients without MODS. CC-16 is also an anti-inflammatory protein and suggested as biomarker for the development of pneumonia in trauma patients.17 In a study of 101 polytrauma patients with severe chest trauma, higher levels of CC-16 were found at admission and day 2 in patients who developed pneumonia compared with patients without pneumonia.17 Furthermore, patients with ARDS from multiple causes including trauma showed higher levels of CC-16 compared with patients without ARDS.39 In this study, 28.1% of patients with MODS also fulfilled the ARDS criteria, which could partly explain the association of CC-16 with the development of MODS in this study. The anti-inflammatory effects of CC-16 have been studied in a murine model of thoracic trauma. In this study, mice were treated with anti-CC-16 antibodies or IgG directly after trauma. Early anti-CC-16 treatment was associated with more neutrophil infiltration and more damaged lung tissue compared with IgG vehicle-treated mice.40 Taken together, in the present study MODS seemed more related to anti-inflammatory proteins than to proinflammatory proteins. It remains to be determined how these cytokines contribute to organ failure after trauma, as their function is thought to be inhibition of the inflammatory response to prevent further tissue damage. We speculate that an overshoot in inflammation causes an overshoot in anti-inflammatory proteins. Alternatively, IL-1RA in trauma may exert more functions than inhibition of IL-1, in a fashion which is as yet undetermined.
Remarkably, markers of endothelial dysfunction did not differ between patients with and without MODS. Both groups had elevated VCAM-1 and ICAM-1 levels at presentation, indicative of endothelial barrier dysfunction, which is in line with previous literature.41 However, the finding that patients with MODS did not exhibit more endothelial dysfunction at presentation is in contrast with previous findings. These studies showed persistent higher syndecan-1 and thrombomodulin levels in patients who developed MODS.14 An explanation for this result could be that endothelial barrier function was measured with different biomarkers in this study (e.g. TF, ICAM-1, VCAM-1), which might increase later in the course of trauma42 than markers of glycocalyx degradation (eg, syndecan-1 and thrombomodulin). Alternatively, differences between the timing of measurement of biomarkers may have played a role.
This study has several limitations. Patients with MODS differed from patients not developing MODS. They were more often female and more often had TBI compared with patients without MODS. Also, these patients had higher base deficits and had more deranged coagulation parameters. Many factors contribute to the development of MODS including trauma mechanism, shock, coagulopathy and resuscitation strategies.43 44 Due to the limited number of MODS in this cohort, correction in the association model was limited. However, we did correct for injury severity, which is associated with many of these parameters, including shock, coagulopathy and TBI.45
In conclusion, in this study, increased levels of anti-inflammatory proteins CC-16 and IL-1RA were associated with the development of MODS in trauma patients. Future research should validate these results in other trauma cohorts. Furthermore, the mechanisms by which anti-inflammatory pathways contribute to trauma-related MODS should be further studied.
References
Footnotes
Contributors DJBK drafted the article, performed luminex and statistical analysis, and revised all versions of the article. AMTB performed luminex analysis. MWH supervised the project. NPJ supervised the project, and revised all versions of the article. All authors approved the final article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The ACIT-3 study was approved by the Ethics Committee of the Amsterdam University Medical Centers, location Academic Medical Center, and deferred informed consent for blood draws was obtained from patients or relatives.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article. No data are available.