Article Text

Abstract
Background The elderly trauma patient has increased mortality compared with younger patients. During the last 15 years, initial treatment of severely injured patients at Oslo University Hospital Ulleval (OUHU) has changed resulting in overall improved outcomes. Whether this holds true for the elderly trauma population needs exploration and was the aim of the present study.
Methods We performed a retrospective study of 2628 trauma patients 61 years or older admitted to OUHU during the 12-year period, 2002–2013. The population was stratified based on age (61–70 years, 71–80 years, 81 years and older) and divided into time periods: 2002–2009 (P1) and 2010–2013 (P2). Multiple logistic regression models were constructed to identify clinically relevant core variables correlated with mortality and trauma team activation rate.
Results Crude mortality decreased from 19% in P1 to 13% in P2 (p<0.01) with an OR of 0.77 (95 %CI 0.65 to 0.91) when admitted in P2. Trauma team activation rates increased from 53% in P1 to 72% in P2 (p<0.01) with an OR of 2.16 (95% CI 1.93 to 2.41) for being met by a trauma team in P2. Mortality increased from 10% in the age group 61–70 years to 26% in the group above 80 years. Trauma team activation rates decreased from 71% in the age group 61–70 years to 50% in the age group older than 80 years. Median ISS were 17 in all three age groups and in both time periods.
Discussion Development of a multidisciplinary dedicated trauma service is associated with increased trauma team activation rate as well as survival in geriatric trauma patients. As expected, mortality increased with age, although inversely related to the likelihood of being met by a trauma team. Trauma team activation should be considered for all trauma patients older than 70 years.
Level of evidence Level IV.
- geriatric trauma
- triage
- outcome
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Life expectancy in high-income countries is steadily increasing, and consequently, the number of geriatric trauma patients will rise.1–4 Elderly patients present a challenge to trauma care not only because of their increasing numbers. The geriatric patient has limited physiologic reserves and often presents with comorbidities and preinjury medication associated with increased risk of complications and death.5–7 Already two decades ago, mortality was shown to be doubled in patients older than 65 years compared with younger patients with equivalent injury severity.8 Shortly thereafter, old age was suggested to be a criterion for trauma team activation9 and such a strategy has recently been shown to be associated with decreased mortality.10 However, undertriage of the elderly trauma patients are still reported by several studies in the USA.1 11–14
In line with international trends, our initial treatment of trauma patients has changed substantially during the last 15 years with increased focus on a multidisciplinary approach, updated Damage Control Resuscitation (DCR) protocols, and interventional radiology associated with improved outcomes overall and in subgroups of patients with specific injuries.15–18 However, whether there has been an improvement in outcome in the elderly trauma population during the same period has not been explored and constitutes one aim of the present study. Additionally, we wanted to assess whether there has been a change in the proportion of elderly trauma patients met by multidisciplinary trauma teams during the study period.
Methods
Oslo University Hospital Ulleval (OUHU) is a major Scandinavian trauma center with a catchment area of approximately 3 million people covering the southeastern part of Norway. The number of admissions has increased gradually with 1755 trauma team activations in 2013 versus 656 in 2002. Approximately 90% have sustained blunt trauma and approximately 30% are severely injured with an Injury Severity Score (ISS) more than 15.
We performed a retrospective study of all trauma patients >60 years admitted to OUHU and included in Oslo University Hospital Trauma Registry (OUH-TR) during the 12-year period, 2002–2013. OUH-TR includes all trauma patients admitted through trauma team activation, patients with penetrating injuries proximal to elbow or knee, or patients with ISS >9 admitted to OUHU directly or via local hospital within 24 hours after injury.
From the OUH-TR, we extracted age, gender, mechanism of injury (MOI), date of injury, Glasgow Coma Scale (GCS) score, admission systolic blood pressure (SBP), heart rate (HR), base deficit (BD), ISS, anatomic injury classified according to the Abbreviated Injury Scale (AIS) 1998,19 preinjury physical status according to the American Society of Anesthesiologists physical status classification system (PPS-ASA),20 21 transfusions prior to admission in the intensive care unit (ICU), team activation rate, hospital length of stay (LOS), LOS in ICU, probability of survival (Ps) calculated according to the Trauma and Injury Severity Score methodology with coefficients published from the National Trauma Data Bank in 2005,22 30-day mortality, and main cause of death. Survival status 30 days after injury was obtained from patient records and the Norwegian Population Registry. A patient with an ISS >15 not met by a multidisciplinary trauma team at admission was defined as undertriaged. Trauma team activation rate is the percentage of elderly patients included in the OUH-TR and admitted with trauma team activation.
The study population was analyzed for differences between the periods 2002–2009 (period 1 (P1)) and 2010–2013 (period 2 (P2)). The cut-off point was chosen to reflect effects of institutional changes in trauma organization including improved DCR strategies with an updated massive hemorrhage protocol23 and the implementation of the regional trauma system with defined triage and transfer criteria. Furthermore, the study cohort was stratified into three groups based on age: 61–70, 71–80, and >80 years of age and subjected to subgroup analyses.
Continuous data are presented as medians with IQR. Comparisons between groups were performed using Mann-Whitney U test. Categorical data are reported as proportions and tested for significance using Pearson’s χ2 test. For all analyses, a p value <0.05 (derived from a two-tailed test) was considered to indicate significance.
A forward stepwise selection of significant covariates including potential confounders was performed to identify variables independently associated with 30-day mortality. The variables selected for univariate analysis were: period, age, GCS, PPS-ASA (defined as low risk 1–2 and high risk 3–5), ISS, BD, PR, SBP, gender, transfusions, team activation, and MOI (defined as high and low energy). These core variables were then applied to construct a multiple logistic regression model evaluating factors affecting mortality. All variables were prespecified and considered clinically important. The fit of the model was measured with the Hosmer-Lemeshow goodness-of-fit-test statistic. Calculation of the accuracy of the test was measured by the area under the receiver operating characteristic curve for the prediction of 30-day mortality. A similar procedure was followed to construct a multiple logistic regression model to identify variables independently associated with trauma team activation. The variables selected for univariate analysis were: period, age, GCS, ISS, PPS-ASA (defined as 1–2 low risk, 3–5 high risk), gender, SBP, PR, transfusions, and MOI (defined as high and low energy trauma).
All statistical analyses were performed using the IBM SPSS V.25. The institutional data protection officer had no objections to the study.
Results
The study cohort consisted of 2628 patients; 62% were men and median age was 72 years. MOI was blunt in 96% of patients, most commonly secondary to falls (59%), motor vehicle crashes (16%), and pedestrian hit by motor vehicle (7%).
P1 compared with P2
P1 included 1411 patients and P2 included 1217 patients. Demographic and outcome data are presented in table 1. Median ISS was 17 in both periods. A total of 841 (60%) patients in P1 and 662 (54%) in P2 were severely injured with ISS >15.
Patient’s characteristics stratified by time periods
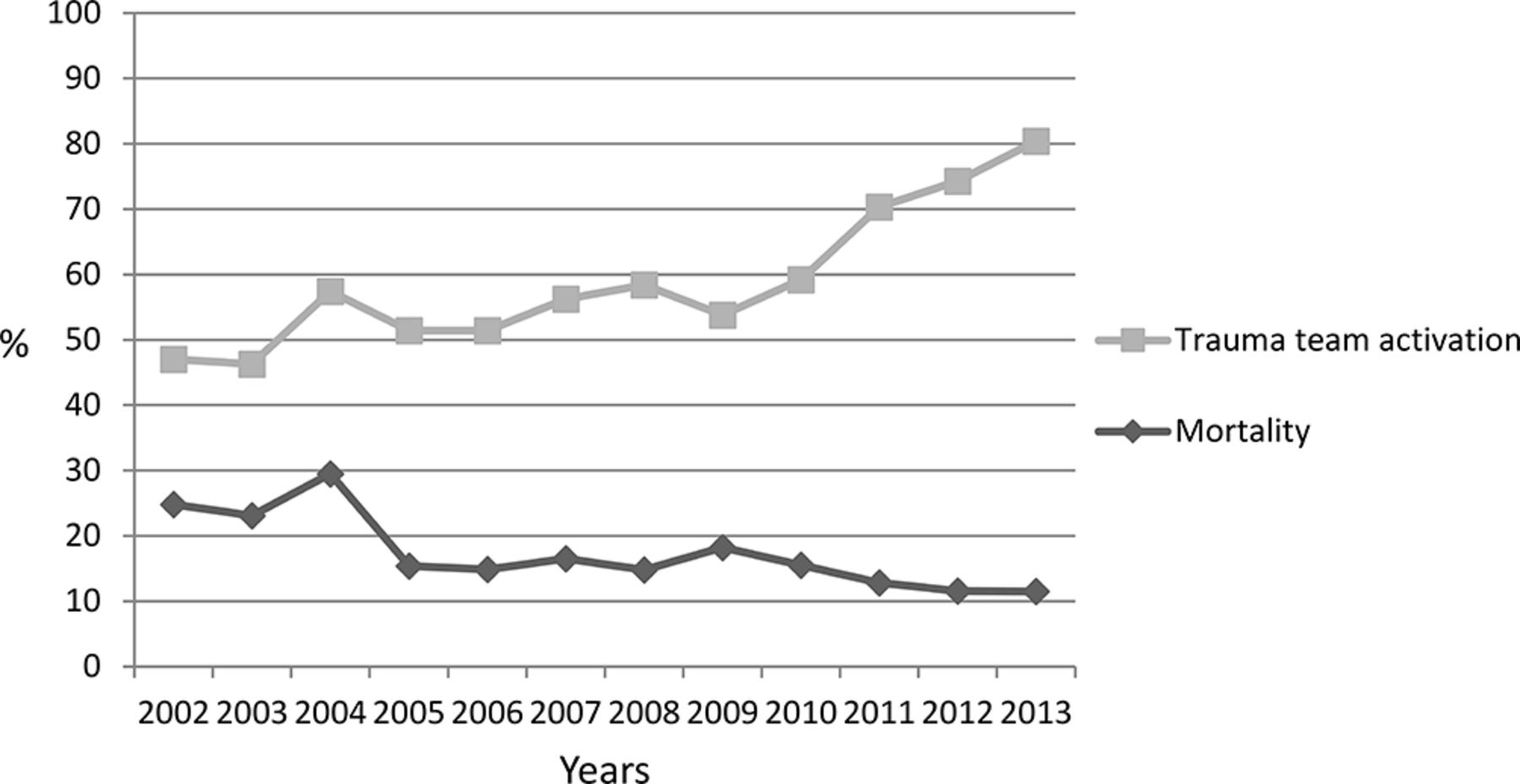
Trauma team activation rates increased from 53% in P1 to 72% in P2 (p<0.01), whereas crude mortality decreased from 19% in P1 to 13% in P2 (p<0.01). Main cause of death was traumatic brain injury in both periods, 67% in P1 and 70% in P2, respectively. The figure 1 illustrates a gradual increase in trauma team activation rates accompanied by a reduction in mortality rates during the study period.

Trends of mortality and trauma team activation rates in the total study population, Oslo University Hospital Ulleval, 2002–2013.
Comparison between age groups
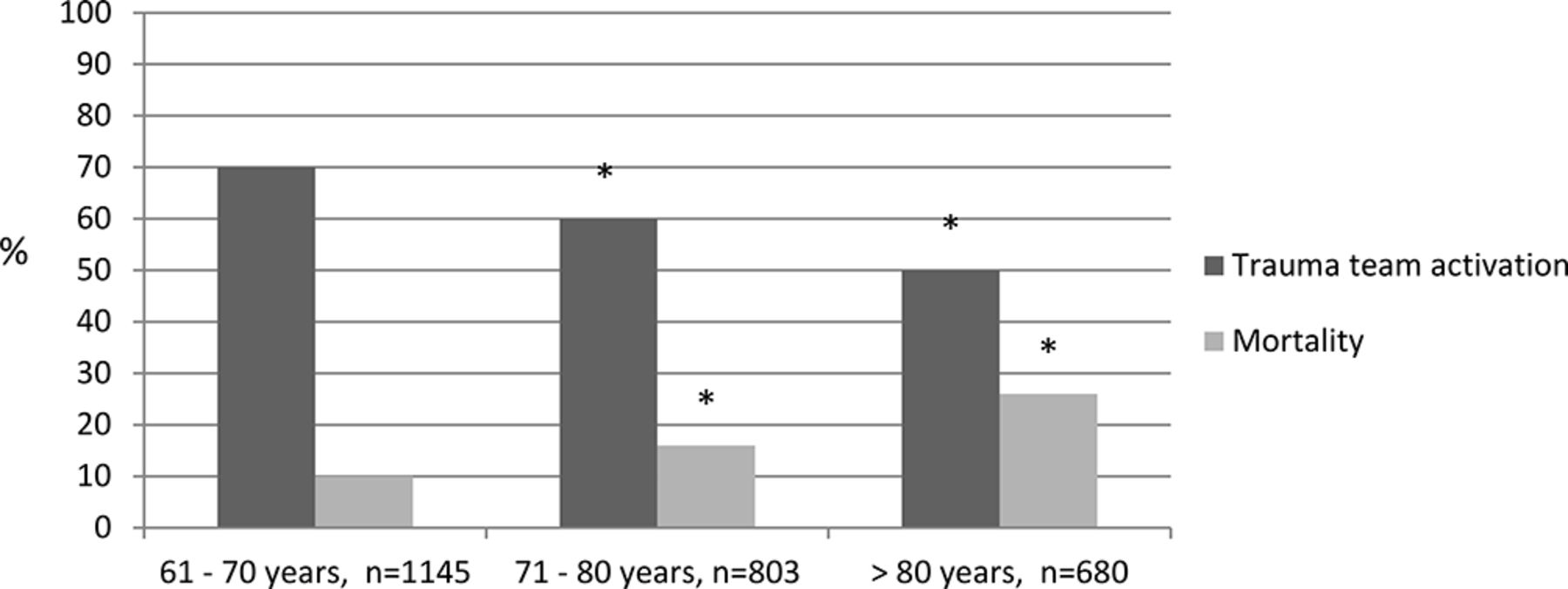
Although there were no significant differences in GCS, BD, ISS, or Ps between the three age groups (table 2), we identified an increase in mortality related to age; 10% in the age group 61–70 years, 16% in the age group 71–80 years and 26% in the age group above 80 years, respectively, accompanied by a decrease in trauma team activation rates as shown in the figure 2. In the subgroups of severely injured patients (ISS >15), team activation rates were 68% in the age group 61–70 years, 57% in the age group 71–80 years, and 51% in patients older than 80 years (table 2). When comparing P1 with P2, we found a significant decrease in mortality and increase in team activation rate in all three age groups (table 1).
Patient’s characteristics stratified by age groups

{kind=link}
{kind=link}
Mortality and trauma team activation rates stratified by age group. Asterisk indicates significant differences (p<0.05) from age group 61–70.
Multiple regression models
Table 3 presents crude and adjusted ORs, identifying P1, age, GCS, PPS-ASA, ISS, and BD to be independently correlated with 30-day mortality. The logistic regression model resulted in an OR of 0.77 (95% CI 0.65 to 0.91) for dying when admitted in P2. The area under the curve (AUC) for the score in the test data set was 0.90 (95% CI 0.88 to 0.92; p<0.01). The Hosmer-Lemeshow test statistic for model fit was acceptable (χ2=10.18, df=8, p=0.25).
Logistic regression model for identifying factors influencing mortality
Table 4 presents crude and adjusted ORs identifying period, age, GCS, ISS, PPS-ASA, gender, SBP, transfusions, and MOI to be independently correlated with trauma team activation. The logistic regression model resulted in an OR of 2.16 (95% CI 1.93 to 2.41) for being met by a trauma team in P2. The AUC for the score in the test data set was 0.83 (95% CI 0.81 to 0.85; p<0.01). The Hosmer-Lemeshow test statistic for model fit was acceptable (χ2=11.38, df=8, p=0.18).
Logistic regression model identifying factors influencing trauma team activation
Discussion
This study demonstrates a decrease in crude mortality in the elderly trauma patients from 19% in P1 to 13% in P2. Moreover, a multiple regression model for predicting 30-day mortality identified an OR of 0.77 for dying when admitted in P2. Although many studies have shown increased survival in the adult trauma population related to the development of trauma systems,24–26 to our knowledge, the present study is the first to show a general survival benefit in the geriatric trauma population treated in a single institution. The explanation for the improvements is likely multifactorial since an institutional system is not static over time and mortality decreased gradually throughout the study period (figure 1). During the last 15 years, there has been a continuous dedicated focus on trauma care in our institution. Previously, we have shown that formalization of a dedicated trauma service, development of a clinical governance structure, and performance improvement programme coincided in time with an overall significantly increased survival.17 Later, the impact of updated massive transfusion protocols and a more multidisciplinary DCR approach probably contributed to further improvement in outcomes.18
Age has been shown to be associated with increased overall mortality after trauma in numerous studies.8 27–29 Due to reduced physiologic reserve, comorbid conditions, polypharmacy including anticoagulant medication, and increased risk of malnutrition the elderly injured patients are at increased risk of complications and death compared with younger patients.5–7 9 30–35 That mortality was more than doubled in patients over the age of 80 compared with the group of patients aged between 61 and 70 years in our study (table 2) was expected. However, mortality was reduced in all three age cohorts from P1 to P2 (table 1), indicating that even the oldest trauma patients benefitted from the institutional improvements in trauma care.
We might speculate that the formalization of a regionalized trauma system with defined triage and transfer criteria in 2010 contributed to the increase in trauma team activation rates (figure 1). Age is not an independent criterion for trauma team activation in these guidelines. The Eastern Association for the Surgery of Trauma’s practice management guideline from 2012 recommended lowering the threshold for trauma team activation in patients aged 65 or older. Numerous reports have pointed out that the use of standard triage criteria is followed by undertriage of patients over the age of 60.1 11 12 14 28 36 Several studies have tried to demonstrate an effect on undertriage and outcome by redefining trauma criteria for the elderly.13 37 38 Brown et al found that substituting SBP of less than 110 mm Hg with the current 90 mm Hg in patients older than 65 achieves a larger reduction in undertriage than increase in overtriage and the risk for mortality is similar in these groups.39 Caterino et al reported the effects of a statewide modification of adult trauma triage criteria to a geriatric substitute by changing cut-off in blood pressure from 90 mm Hg to 100 mm Hg, GCS from 13 to 14 in patients with suspected brain injury, fractures from two or more long bones to one, and introducing additional criteria for injury to two or more body regions, injury from fall from any height with evidence of traumatic brain injury, and pedestrian struck by motor vehicle.40 With these changes, they managed to improve sensitivity in identifying older adults in need of trauma center care, but only minor changes in mortality in the group with an ISS less than 10 and no improvement in mortality for the patients with higher ISS. In our study, trauma team activation was not identified as significantly associated with increased survival. Bradburn et al evaluated implementation of two geriatric-specific practice management protocols, the high risk geriatric protocol (HRGP) and the anticoagulation and trauma alert (ACT).33 Implementation of the HRGP alone did not have a significant effect on mortality. When combined with ACT, mortality was significantly reduced from 7.24% to 4.0%. Implementing a separate set of activation criteria for geriatric patients, as described above, would be challenging in most institutions. Hammer et al reported decreased mortality by simply introducing mandatory highest-level trauma activation on arrival in all injured patients 70 years or older regardless of physiology or MOI.10 In a recently published follow-up study aiming to identify an age cut-off that conveyed a mortality benefit, the authors reported reduced mortality in patients 77 years or older.3 Considering the potential consequences of undertriage in frail elderly, the limited increase in trauma team activations caused by compulsory team activation in all trauma patients 70 years or older seems reasonable.
We found that increased age was inversely related to the likelihood to be met by a trauma team despite the fact that median ISS was 17 in all three age cohorts and thereby that undertriage was most common among the oldest patients (table 2). If our criteria had mandated all patients older than 70 years of age to be met by a multidisciplinary trauma team, the average monthly increase in team activations during the study period would have been 4.6 patients.
There are several limitations to this study including those associated with its retrospective nature. The study design does not allow an evaluation of the influence of undertriage on outcome because differences in case mix and patient volume could influence outcome independent of institutional improvements. The number of patients increased steadily during the study period and may have contributed to a general improvement in trauma care. Higher patient volumes have been associated with increased survival in some studies, whereas others have failed to detect any association between patient volume and mortality.41–44
In this retrospective single-center study on geriatric trauma patients, we found decreased mortality and increased proportion of patients examined by a multidisciplinary trauma team compared with historic controls. Increased age was inversely related to the likelihood to be met by a trauma team despite equivalent injury severity. Trauma team activation should be considered for all trauma patients older than 70 years.
References
Footnotes
Contributors AHR, HR, CG and PAN designed the study. AHR, IAG, NOS, CG and PAN analyzed the data. AHR, CG and PAN conducted the literature search and wrote the article. All authors participated in revising and editing the article.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The institutional Data Protection Officer had no objections to the study.
Provenance and peer review Not commissioned; externally peer reviewed.