Article Text

Abstract
The detailed study of prehospital injury death is critical to advancing trauma and emergency care, as circumstance and causality have significant implications for the development of mitigation strategies. Though there is no true ‘Golden Hour,’ the time from injury to care is a critical element in the analysis matrix, particularly in patients with severe injury. Currently, there is no standard method for the assessment of time to definitive care after injury among prehospital deaths. This article describes a methodology to estimate total prehospital time and distance for trauma patients transported via ground emergency medical services and helicopter emergency medical services using a geographic information system. Data generated using this method, along with medical examiner and field investigation reports, will be used to estimate the potential survivability of prehospital trauma deaths occurring in five US states and the District of Columbia as part of the Multi-Institutional Multidisciplinary Injury Mortality Investigation in the Civilian Pre-Hospital Environment study. One goal of this work is to develop standard metrics for the assessment of total prehospital time and distance, which can be used in the future for more complex spatial analyses to gain a deeper understanding of trauma center access. Results will be used to identify high priority areas for research and development in injury prevention, trauma system performance improvement, and public health.
- prehospital
- preventable death
- trauma
- injury
- geographic information system
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
From a public health perspective, injury remains the leading cause of death in individuals up to the age of 44 and the leading cause of morbidity and mortality among children in the USA.1 A 2016 report from the National Academies of Science, Engineering and Medicine, entitled ‘A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths After Injury,’ estimated that approximately 30 000 of the 147 790 trauma deaths that occurred in 2014 had potentially survivable injury.2 Based on recommendations for leadership and action to develop and implement a national trauma system, the report set the goal of zero preventable death and disability from injury. Concomitantly, the National Trauma Institute has been developing the infrastructure to support the Multi-Institutional Multidisciplinary Injury Mortality Investigation in the Civilian Pre-Hospital Environment (MIMIC) study to elucidate the epidemiology of prehospital injury mortality. The pragmatic goals of this investigation are to estimate the impact of potentially preventable trauma death on society in terms of years of potential life lost and lost productivity and to develop a blueprint to improve the US civilian and military trauma system.
During the last several decades, advances in care in trauma centers and across trauma systems have substantially reduced death and disability associated with injury.3 However, there remains a substantial opportunity to further reduce the number of deaths in the prehospital setting. From an analysis done by the US military during operations in southwest Asia spanning 2001–2011, it was determined that the majority of battlefield deaths occurred prior to casualties receiving care at a military medical treatment facility. Furthermore, it was determined that approximately 25% of the prehospital casualty mortalities died to potentially survivable injury, largely from hemorrhage. Importantly, this work highlighted clear priorities for research and development of mitigation strategies to improve battlefield casualty outcomes.4 Unlike within the battlefield environment, the magnitude and impact of potentially preventable prehospital death from injury in the civilian environment has not been fully explored. These potential liabilities in civilian prehospital care must be identified and remediated to reduce the number of potentially preventable trauma deaths.
Understanding this deficiency, the purpose of the MIMIC study is to develop a coordinated, multidisciplinary, multi-institutional effort within the civilian clinical sector to identify and characterize the causes of mortality from trauma in the prehospital setting and to identify potential high-yield areas for research and development in prehospital medical care, injury prevention, and trauma systems. Using these data and a network of experts, the analysis aims to define the causes and pathophysiologic mechanisms of a nationally representative sample of 3000 prehospital deaths occurring in six regions of the country and estimate the potential for survivability. Key determinants of this investigation include mechanism of injury, physiologic cause of death, estimated time from injury to definitive care, geographic location of the injury, and access to components of the local trauma system.
A multi-institutional and multidisciplinary group of trauma surgeons, neurosurgeons, orthopedic surgeons, forensic pathologist/medical examiners, and emergency medical service (EMS) personnel was created to review these prehospital deaths. These experts will evaluate the potential for survivability of medical examiner injury cases based on the assumption of immediate access to level I trauma center care and under the actual circumstances of the injury. Injury survivability assessments will be established using a specially developed electronic tool with data abstracted from medical examiner reports, field investigation reports, medical examiner radiographic imaging, injury severity coding, and EMS and trauma center accessibility. One major emphasis of this study is to determine the degree to which access to care in the field and the nearest trauma center impact the potential for survivability among deaths occurring prior to definitive care. Numerous studies have supported the argument that longer prehospital times contribute to higher mortality rates,5–8 and that timely delivery of trauma care to severely injured patients is an effective strategy for reducing mortality.9–11 Current research also indicates designated trauma centers significantly lower the risk of mortality and morbidity, with a 25% reduction in 1 year mortality when compared with non-trauma centers.12 Therefore, the potential to integrate data regarding access to designated trauma centers is critical in the panel’s assessment of potential for survivability, given the circumstances of the injury.
Geographic information system (GIS) analysis has been used in previous trauma studies to measure travel time and distance of medical transportation when EMS was not involved, or when an EMS record with time elements could not be obtained. Widener et al13 and Lerner et al14 used network analysis tools to compare ground emergency medical service (GEMS) and helicopter emergency medical service (HEMS) and determine in which areas each transportation method was faster. The purpose of this article is to describe the GIS methodology developed to estimate the total prehospital time and distance by GEMS and HEMS for 3000 prehospital deaths after injury.
Methods
Setting
The MIMIC study includes decedents after injury assessed at six medical examiner study sites. Four states (Connecticut, Maryland, New Mexico, Oklahoma), the District of Columbia, and one county (Johnson County, Iowa) were selected based on their centralized medical examiner system, utilization of an electronic case management system, demographic representation of the USA population, and varying levels of population density. In total, these areas serve a population of approximately 16 million with 14 000 medical examiner cases per year in composite.
The Institutional Review Board at UT Health San Antonio and the Human Research Protection Office at the Department of Defense both deemed this research as non-human subject research.
Data
While having real-time EMS run sheets is ideal for assessing time from injury to definitive care, approximately 80% of this cohort of prehospital decedents after injury is expected to have no EMS activation or engagement. A GIS will, therefore, be used to estimate total prehospital time and distance using current local trauma system resources. For the remaining 20% of the cohort expected to have had EMS interaction, the National Emergency Medical Services Information System (NEMSIS) data set will be used to match real-time EMS data with each subject through cross-referencing individual state-level data sets.
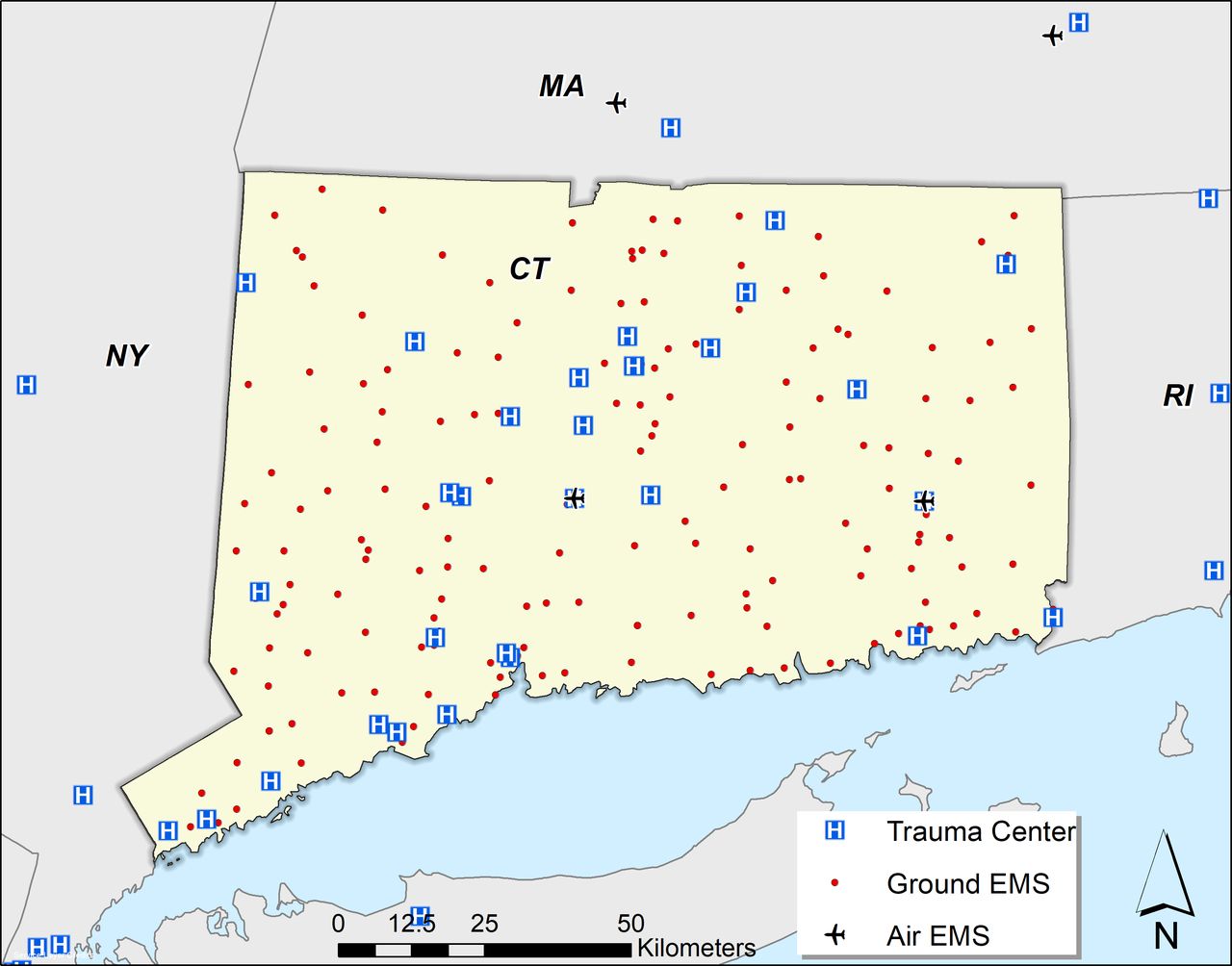
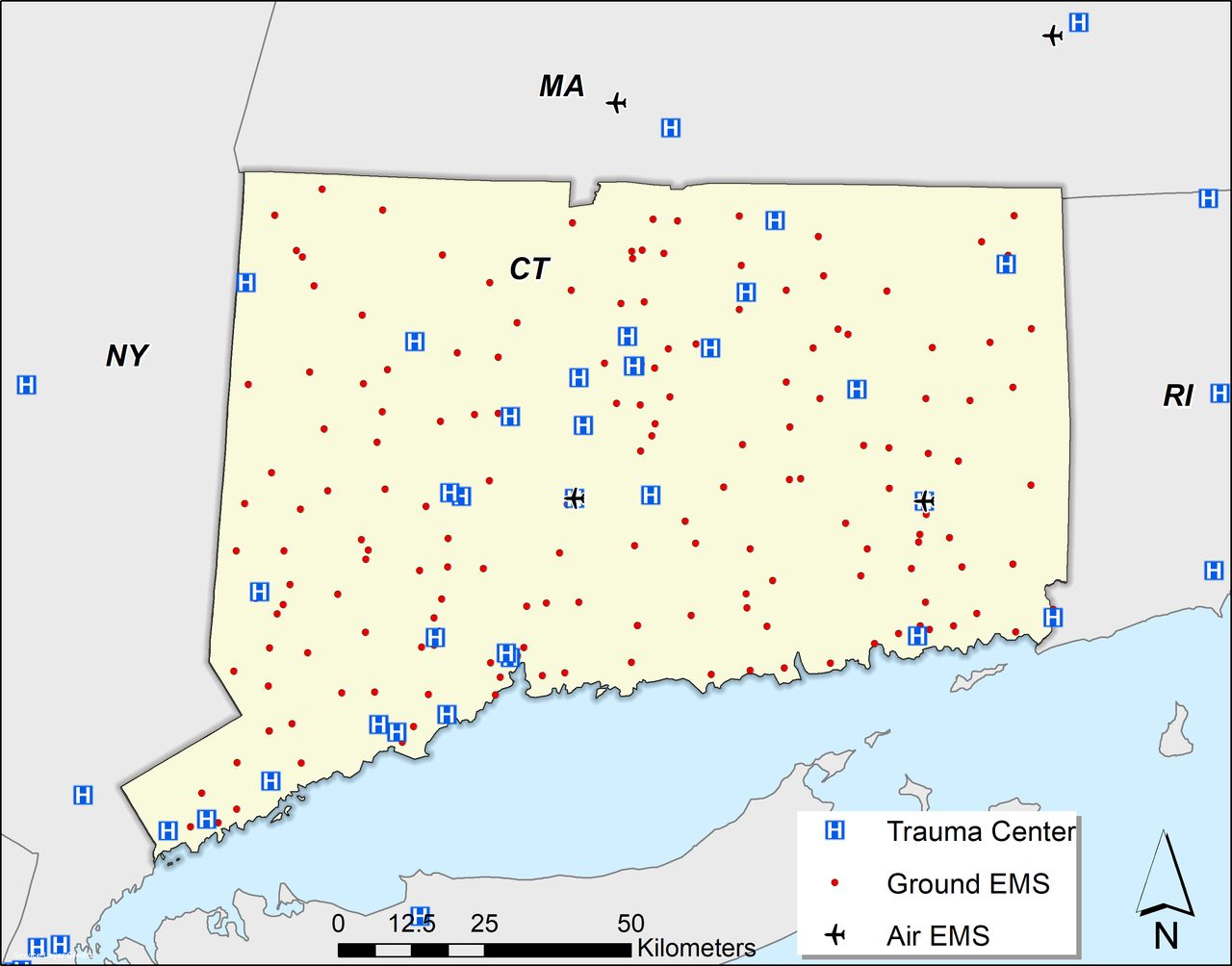
To calculate total prehospital time and distance, geographic data for GEMS depots, HEMS helipads, injury locations, and designated trauma centers were needed in the form of Global Positioning System (GPS) coordinates, physical address, road intersection, or highway mile marker. GEMS depot locations were obtained from respective state Departments of Health and local municipalities. For those rural depots in Maryland and New Mexico that provided PO boxes and no physical addresses, Google Map’s Street View and the depot name were used to visually identify the GEMS depot and retrieve a physical address. HEMS base locations were obtained from the Atlas and Database of Air Medical Services (ADAMS),15 which is a compilation of information on air medical services in the USA that respond to the scene of trauma or medical emergency. HEMS base locations present in the study area as well as in adjoining states were included in the analysis. Level I and II trauma centers were verified by the American College of Surgeons. The study team reached out to state agencies at each of the six study sites to develop a database of all trauma centers for each state, with their physical address, and trauma center designation level. Furthermore, trauma centers in bordering states were included as an assumption that the patient would be transported to the nearest trauma center without regard to state boundaries. Designated trauma center locations obtained using this method were verified using the 2017 American Trauma Society Trauma Information Exchange Program. This comprehensive inventory includes a physical address for all designated level I–IV trauma centers across the USA. After collecting location data for trauma centers, GEMS, and HEMS, a template map for each study area was created. Figure 1 illustrates the geographic locations used for the Connecticut study area.
{kind=link}
Trauma centers, ground emergency medical service (GEMS) and helicopter emergency medical service (HEMS) depots for Connecticut analysis. CT, Connecticut; EMS, emergency medical service; MA, Massachusetts; NY, New York; RI, Rhode Island.
Location of injury will be abstracted from field investigation and police reports by medical examiner offices at each location. If a physical address or GPS coordinates cannot be obtained from these records, the narrative will be reviewed for any supplemental geographic information, including mile markers, landmarks, and in-depth descriptions of the location of injury.
Design
Once an injury location physical address or GPS coordinate is obtained, location data will be geocoded using an address locator tool in ArcGIS V.10.6 (Environmental Research Systems Institute, Redlands, CA). Addresses unable to be geocoded will be manually added to the mapping software using the location narrative in field investigation reports. Results not lying directly on a road network will be snapped to the nearest point on the road network. Rurality of the injury location will be determined based on US Census guidelines. Areas with a population less than 2500 are classified as rural; areas with a population of at least 2500 and less than 50 000 people are classified as urban clusters; and areas with a population of 50 000 or more people are categorized as urbanized areas.
Planned analysis
Multiple time intervals are considered when calculating total prehospital time. Numerous studies13 16 17 have adapted a four-component definition for total prehospital time, which includes activation, response, on-scene, and transport intervals. The activation interval is the time from receipt of 9-1-1 call to EMS departure from depot. The response interval is the time from EMS departure to arrival at scene. The on-scene interval is the time from EMS arrival at the scene to the time when EMS departs the scene for the trauma center. The transport interval is the time from EMS departure from the scene to arrival at the trauma center. This study uses this four-component definition to calculate total prehospital time to level I–IV trauma centers.
The response and transport estimates for GEMS will be computed using a GIS-based network analysis. The StreetMap Premium for ArcGIS (North America V.2018.1) road network will be used in conjunction with the Closest Facility tool within the Network Analyst (ArcGIS V.10.6) to model vehicle transport routes and determine travel times and distances. The road network uses TomTom GPS units in use to provide historic traffic data and accurate time estimates. This model assumes that GEMS are immediately notified about the incident, an ambulance from the nearest GEMS base is sent to the incident location, time is spent at the scene to render emergency medical care and transfer the patient to the vehicle, and the ambulance drives to the nearest trauma center. This is represented by the formula below:
TtotalG=TdispG + TresponseG +TsceneG + TtransportG
TtotalG is the total time in minutes from the placement of the call to trauma patient arrival at the trauma center. TdispG is defined as the time from when the 9-1-1 call was received until the time the GEMS unit was dispatched. Using Carr et al’s16 meta-analysis of prehospital times, 2.9 and 1.4 minutes were applied for rural and non-rural locations, respectively. TresponseG is the travel time in minutes from the nearest GEMS depot to the site of the incident, using the road network. Based on prior literature, TsceneG is the assumed time spent at the incident location by the EMS team to render aid, move the patient into the ambulance, and prepare the patient for transport. Intervals of 13.5, 13.5, and 15.1 minutes were used for urban, suburban, and rural locations, respectively.16 TtransportG is defined as the travel time from scene to the closest trauma center by the available ground network.
The HEMS estimates will use the same assumptions as the GEMS estimates (eg, immediate notification), however our estimates use travel times that characterize helicopter transport, which uses straight-line routes instead of a road network. The Near tool (ArcGIS V.10.6) will be used to select the nearest HEMS depot and calculate the straight-line distance. The total HEMS time is represented by the formula below:
TtotalH=TdispH + TresponseH +TsceneH + TtransportH
TtotalH is the total time in minutes from the placement of the 9-1-1 call to patient arrival at a trauma center via helicopter. TdispH is defined as the time from when the 9-1-1 call was received until the HEMS unit was dispatched. A constant of 3.5 minutes was used, drawing from a meta-analysis of literature on HEMS prehospital times for trauma care.16 TresponseH is the estimated travel time from the nearest HEMS to the injury location using a straight-line flight path and an average helicopter cruising speed of 142.6 mph.16 TsceneH is equal to a constant 21.6 minutes, and is the average time spent on-scene to stabilize a patient and move to the helicopter.16 TtransportH is the estimated travel time from the injury location to the nearest trauma center using straight-line flight path and cruising speed of 142.6 mph.
Discussion
Since trauma is such a significant public health issue and one of the leading causes of death in the USA, the MIMIC study intends to evaluate prehospital deaths after injury and highlight opportunities for performance improvement and trauma system development and maturation. As the majority of injury death occurs prior to hospital care, the capacity to evaluate casualty access across the continuum of care is a key element in making potential survivability determinations. GIS technology based on a four-component prehospital domain definition provides a standard reproducible method to obtain a quantitative assessment of prehospital time.
During the initial data collection process, several opportunities for improving data linkage within the EMS system were discovered. First, while the HEMS locations consolidated by ADAMS15 provided detailed location information, state-wide GEMS location data proved more challenging. Due to the regional nature of EMS systems, a comprehensive list containing all GEMS depots for an entire state was difficult to obtain. For two study sites, lists provided by the Departments of Health contained PO Box information. This is not the physical location of EMS services and could not be used for travel time calculations using GIS. Moreover, the verification process for obtaining physical addresses was quite cumbersome and time consuming.
Linking prehospital EMS records was difficult. The nature of the medical examiner process limits the value and necessity of detailed information with respect to EMS interactions. Likewise, arrival times for responders other than EMS were frequently absent from reports, as were GPS coordinates and physical addresses. Therefore, to add more granular detail and precision to this study, we cross-referenced death cases with an EMS intervention to matching records in state-level EMS databases after effecting data use agreements with each entity.
Current methodologies quantifying overall access to trauma centers in the USA have limitations in their design, and use average driving speeds based on rurality instead of historic traffic data3 18; or they estimate time from GEMS depot to injury location using empirically determined constants instead of network analysis.3 18 19 Viewing trauma care accessibility in this way does not provide a realistic view based on how trauma systems are designed, as they are predicated on convenience due to the inherent limitations posed by regulated or incomplete data linkages and the non-standardized geopolitical oversight of agencies and organizations across the spectrum of care. Results from this study will include GIS-calculated response intervals from GEMS/HEMS depot to injury location, and therefore, may provide more accurate total prehospital time.
Future directions
There is currently a gap between the availability of spatial methodologies and the extent to which they are employed in understanding medical evacuation.20 While prehospital time and distance calculated with this planned methodology may prove useful as a surrogate when EMS was not involved or a record with time elements could not be obtained, these values may also be useful for more advanced and robust spatial techniques such as hot spot analysis, cluster analysis, and spatial interpolation. An ordinary least squares or kernel density analysis can be used to determine statistically significant hot and cold spots of severe trauma incidents and help guide trauma system resources, as was done for Mobile, AL.21 Local Moran’s I may be used to identify spatial clusters of incidents with high or low transport times22 or injury severity.23 Spatial interpolation methods, such as kriging, use existing points to estimate values of other points.13 Kriging could be used to more accurately estimate trauma center accessibility. Both spatial analysis techniques can be combined with publicly available US Census demographic data to provide insight and perspectives on the current state of the USA trauma system on a local, state, or national level.
There are also more advanced methods that can be applied to calculate total prehospital time. The study team is working on analyzing NEMSIS data to determine if a more accurate estimate for total prehospital time—specifically, mean on-scene time—can be determined. The study methods for calculating total prehospital time may be adjusted if the analysis yields results that provide a more precise estimation of time for the data used in this study.
GIS integration into MIMIC study design will be one of the most important components to identify potential high-yield areas for research and development in prehospital medical care, injury prevention, and trauma systems.
References
Footnotes
Contributors BJE devised the project and the main conceptual ideas of the MIMIC project. NWM designed the model and took the lead in drafting the article. All authors provided critical feedback and helped shape the research and article.
Funding This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs, through the Defense Medical Research and Development Program under Award No W81XWH-17-2-0010.
Disclaimer The US Army Medical Research Acquisition Activity, 820 Chandler Street, Fort Detrick, MD 21702-5014 is the awarding and administering acquisition office. Opinions, interpretations, conclusions and recommendations are those of the authors and are not necessarily endorsed by the Department of Defense.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.