Article Text

Abstract
Background The use of extracorporeal membrane oxygenation (ECMO) as salvage therapy for patients with severe acute respiratory distress syndrome is gaining greater acceptance among trauma intensivists. The objective of this study was to review ECMO usage in trauma patients in the USA.
Methods The National Inpatient Sample (NIS) from years 2002 to 2012 was queried for patients aged 15 and older treated with ECMO who had one or more acute traumatic injuries as defined by the International Diagnostic Codes, Ninth Edition (ICD-9). The primary outcomes of interest were incidence of ECMO and overall inpatient mortality.
Results A total of 1347 patients were identified in the NIS database who had both ECMO performed and ICD-9 codes consistent with trauma. Patients were predominantly aged 15 to 29 years (31.4%) and were male (65.5%). The incidence of ECMO for patients after traumatic injuries has increased 66-fold during the 10-year period. In-hospital mortality was 48.0% overall, with a decreasing trend during the study period that approached statistical significance (p=0.06).
Discussion Although ECMO use in patients in the post-trauma setting remains controversial, there is an increasing trend to use ECMO nationwide, suggesting an increasing acceptance and/or increased availability at trauma centers. Given the decrease in mortality during the study period, ECMO as a salvage method in trauma patients remains a potentially viable option. Evaluation in a prospective manner may clarify risks and benefits.
Level of evidence Level IV, epidemiological.
- ECMO
- trauma
- ARDS
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Trauma is the leading cause of mortality among patients under 46 years old and the leading cause of years of life lost within the USA.1 Acute respiratory distress syndrome (ARDS) remains a common complication among trauma patients, diagnosed in 6.5% of patients requiring mechanical ventilation greater than 48 hours.2 Extracorporeal membrane oxygenation (ECMO) has been used extensively in pediatric and pulmonary transplant patients who require additional cardiopulmonary support when standard means of ventilation are ineffective.3 Despite advances in ventilatory techniques and critical care, mortality remains significant. As a result, ECMO has received consideration as potential salvage therapy in the setting of refractory hypoxia during severe ARDS among trauma patients. Multiple case reports and small single-institution case series have been published to support the use of ECMO as a bridge for these patients as they recover from their underlying lung injury with reported improved mortality.4–13 However, to date, national estimates of the use of ECMO in trauma patients and their outcomes have not been published. The purpose of this study was to evaluate ECMO use and associated outcomes in trauma patients using nationally representative data.
Patients and methods
Data source
The National Inpatient Sample (NIS) is a database maintained as part of the Healthcare Utilization Project of the Agency for Healthcare Quality and Research. The NIS is the nation’s largest all-payer inpatient care database and contains data on approximately more than seven million hospital stays each year. Weighted, it estimates more than 36 million hospitalizations nationally.14 The NIS contains information on patient demographics, hospital characteristics, International Diagnostic Codes, Ninth Edition (ICD-9) codes diagnostic and procedure codes, and lengths of inpatient hospital stays following coded procedures.
Study population
The study is a retrospective analysis of the NIS database from years 2002 to 2012. The NIS database was queried for all patients aged 15 and older with at least one ICD-9 diagnosis code for injury (ie, 800 through 958) and an ICD-9 procedure code for ECMO (ie, 39.65). The database was further queried to determine which patients managed with ECMO were diagnosed with multiple rib fractures, hemorrhagic shock, or traumatic brain injury.
Variables and definitions
The primary outcomes of interest were incidence of ECMO and overall inpatient mortality in patients receiving ECMO.
Results
Between 2002 and 2012 an estimated 1347 patients older than 15 years of age with traumatic injuries were treated with ECMO (table 1).
Demographics of NIS sample of trauma patients treated with ECMO
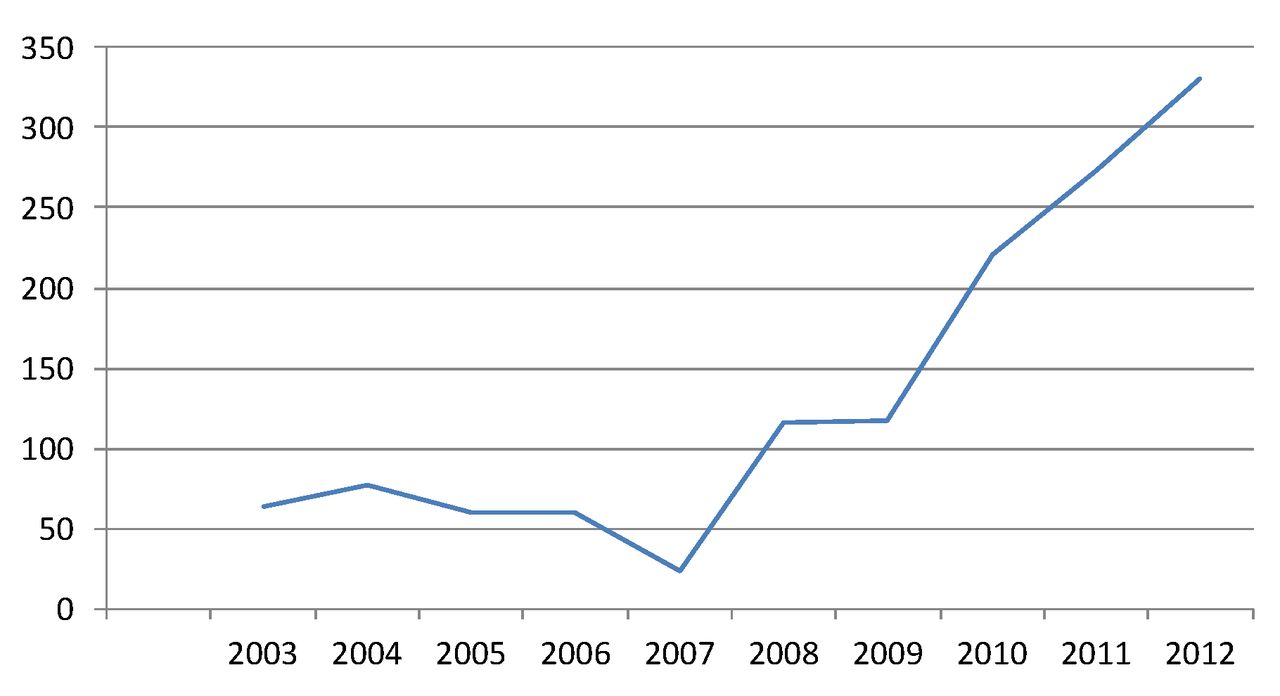
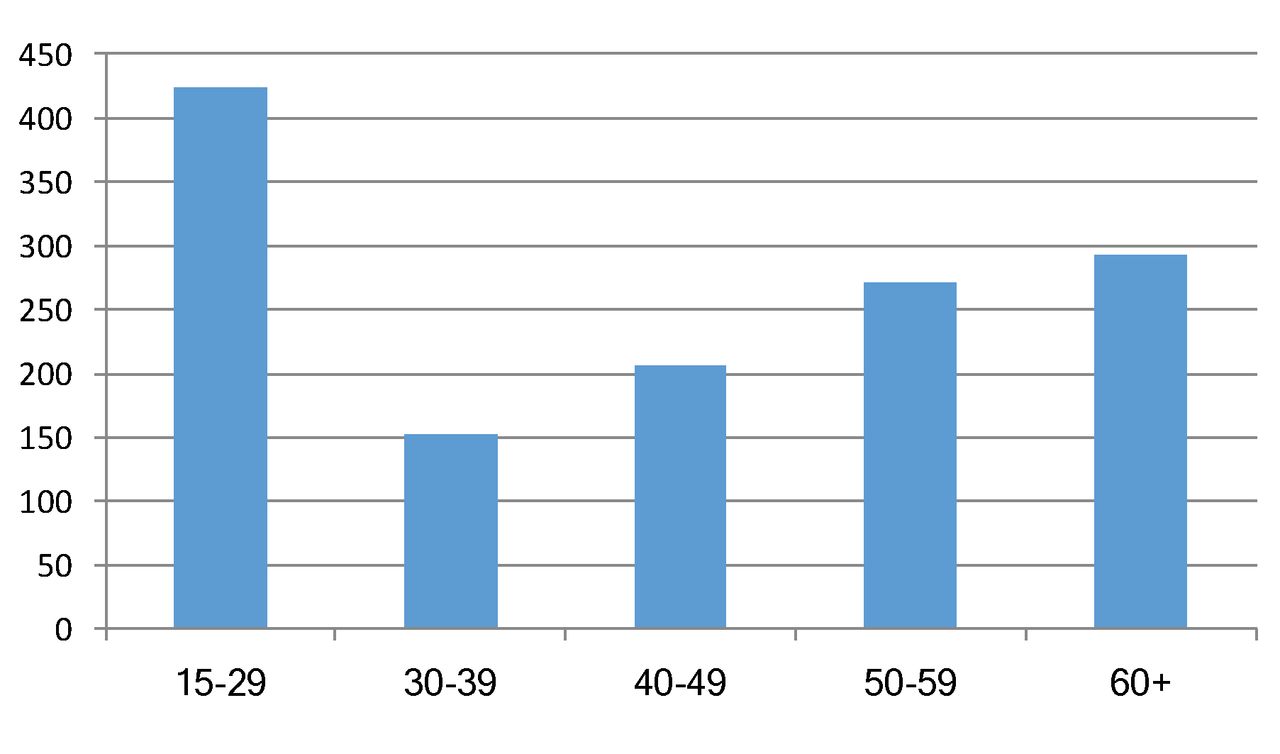
The frequency of ECMO for injured patients increased from 4 in 2002 to 330 in 2012, with the sharpest rise in usage during the last 5 years of the study (figure 1). The average hospital length of stay was 31.1 (SD 67.7) days. The average number of hospital days prior to initiation of ECMO was 6.2 (SD 19.8) days. The majority of patients were male (65.5%). ECMO was most frequently used in the 15 to 29 years age group (31.4%), with the 60+ and 50 to 59 years age groups having the second and third highest percentages, respectively (figure 2).

Frequency of extracorporeal membrane oxygenation use in trauma patients per year.
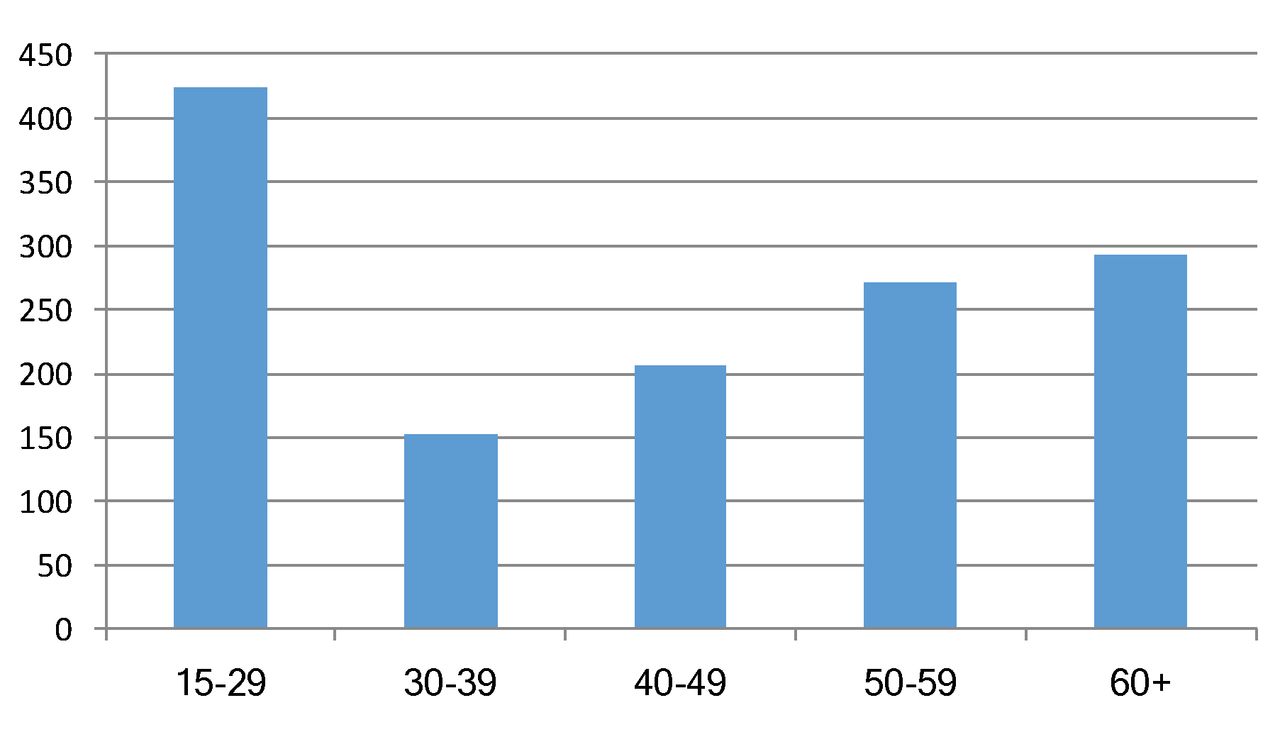
Extracorporeal membrane oxygenation for trauma age distribution (2002–2012).
Patients requiring ECMO were more likely to have suffered multiple rib fractures, with 12.8% of patients with this injury compared with only 4.0% with hemorrhagic shock and 4.8% with traumatic brain injury (TBI).
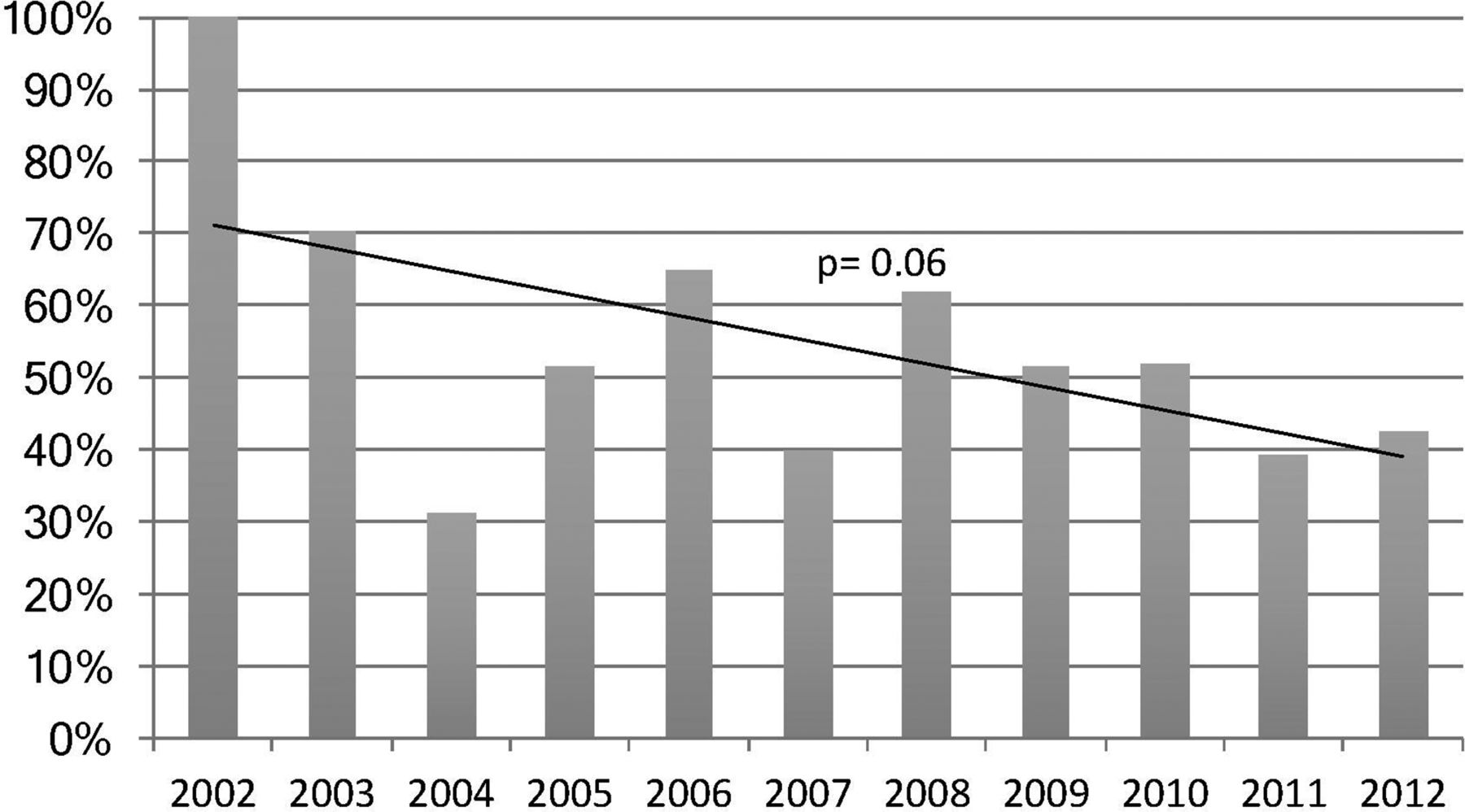
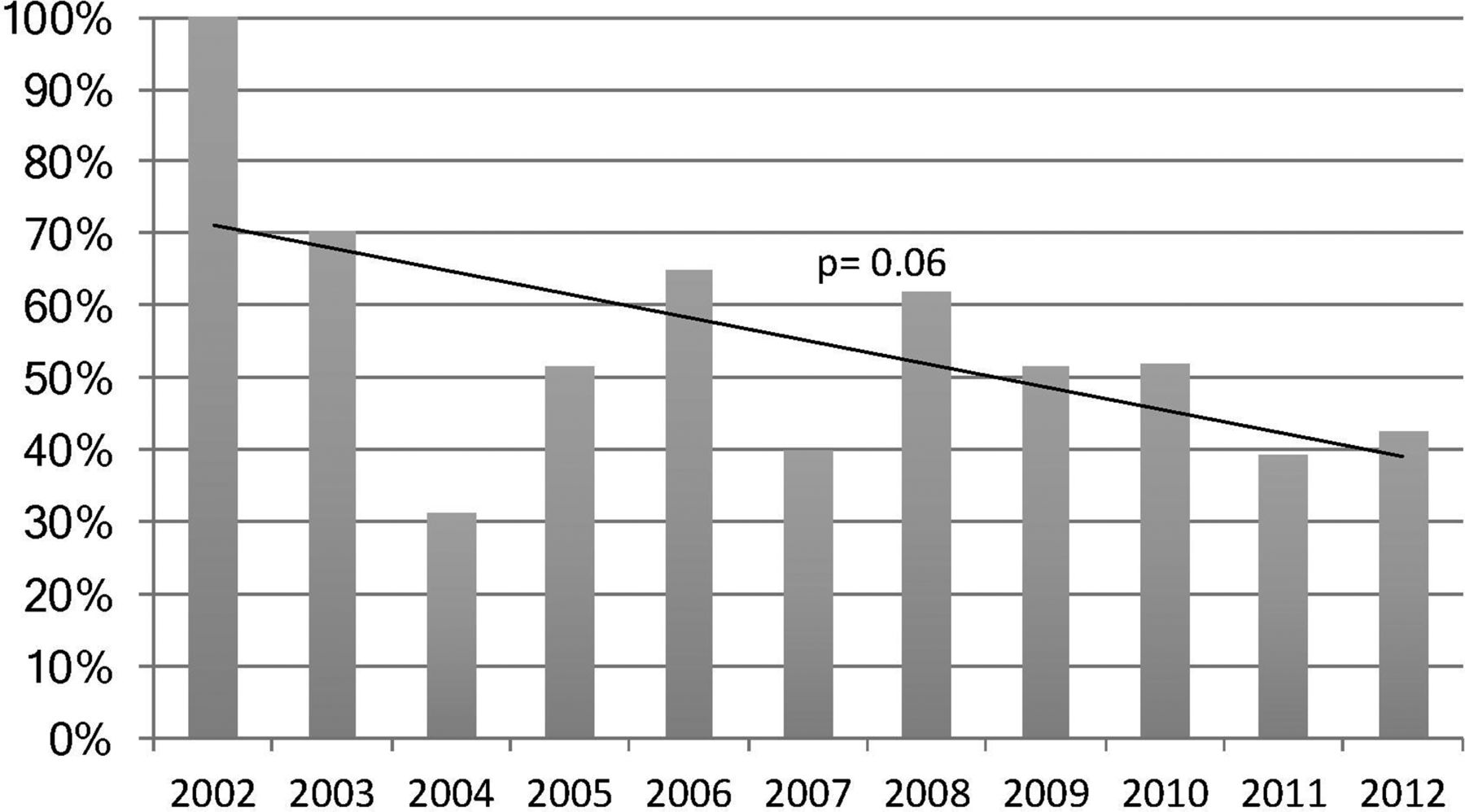
The overall mortality rate for all ages during the study period was 48.0%. Mortality rates fluctuated but decreased overall during the study period (figure 3). Mortality was noted to be highest in the patient group older than 40 years of age; the 40 to 49 years age group, 50 to 59 years age group, and 60+ years age group all demonstrated a mortality rate of greater than 50%. Mortality was lowest in the 30 to 39 years age group at 35%. No data are available regarding neurologic outcome or ability to complete activities of daily living.
{kind=link}
{kind=link}
{kind=link}
Extracorporeal membrane oxygenation mortality percentage per year.
On multivariate regression modeling, only the presence of hemorrhagic shock at admission was significantly associated with mortality in patients requiring ECMO (table 2).
Multivariate regression model of factors associated with mortality in trauma patients managed with extracorporeal membrane oxygenation
Discussion
The use of ECMO in trauma patients was first seen in 1972, when Hill et al 15 published a single case study reporting the first successful application of ECMO within the trauma population. Subsequently in 1979, Zapol et al 16 published the first National Institutes of Health-sponsored randomized controlled study on the use of ECMO in adults. In their study, the addition of ECMO to patients on high-pressure ventilation did not statistically improve 30-day survival. However, this study has several limitations preventing its application to trauma patients today. Namely, the study population consisted almost entirely of medical patients, with treatment limited to venoarterial ECMO. Additionally, ventilatory support consisted only of high-pressure and high fractional inspired oxygen support, rather than modern lung protective strategies.
Although initial support for the use of ECMO in adults waned, enthusiasm has again grown after publication of studies such as the conventional ventilatory support vs extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR) trial in 2009. This randomized controlled trial demonstrated decreased severe disability or death at 6 months among patients with respiratory failure receiving ECMO rather than conventional ventilator support alone.17 Incorporation of modern ventilator management and critical care techniques in collaboration with ECMO in this study and others suggests that ECMO has a role as a rescue therapy in the management of refractory ARDS.18 19 Definitive evidence for support of ECMO use in severe ARDS remains inconclusive. The recently published ECMO to Rescue Lung Injury in Severe ARDS (EOLIA) trial compared patients managed with ECMO with standard care to determine if ECMO improved 60-day mortality in patients with severe ARDS.20 Although patients managed with ECMO showed a lower rate of mortality, the results did not achieve significance.
Similar to other national trends, we demonstrated in our study that ECMO use is increasing in popularity among trauma patients. Our study is in line with the recent findings of ECMO use in trauma patients from the Extracorporeal Life Support Organization database described by Swol et al.21 Sixty-two percent of patients receiving ECMO did so from 2011 to 2016 compared with 48% from 1989 to 2010. The continued increase in popularity for ECMO should not be surprising. Initial support for application of ECMO to the trauma population followed several case reports and small case series that supported ECMO use as a bridge for trauma patients as they recovered from their underlying lung injury.4–13 With the increasing cumulative body of evidence, ECMO use in trauma has reflected similar national trends seen in all adult patients.22 This is best demonstrated in the article of all adult patients managed with ECMO measured in the NIS by McCarthy et al,23 in which annual ECMO use is displayed in a figure that closely mirrors our figure 1]. These trends are expected to continue as the EOLIA trial is now the first randomized control trial using ECMO in the treatment of ARDS to allow inclusion of trauma patients, although within an overall mixed population.20
The current study suggests that the use of ECMO to salvage traumatically injured patients has seen a dramatic increase in the USA, most significantly during the past 5 years. Corresponding improvements in mortality can be seen since 2002, approaching statistical significance. Although this study is incapable of determining the cause for the decrease in mortality, it may be due in part to a combination of increased experience with ECMO utilization, refined technology and patient management protocols, improved patient selection, and earlier use of ECMO as a rescue therapy. Among trauma patients with severe ARDS, we recently demonstrated that the early application of ECMO after the development of refractory hypoxia resulted in significantly decreased mortality compared with historical controls (13.3% vs. 64%; p=0.01), despite similar demographics, and Murray Lung Injury, sequential organ failure assessment, Injury Severity Score, and Acute Physiology and Chronic Health Evaluation-II scores.24 Timing from initiation of severe ARDS to intervention with ECMO therapy occurred on an average of 1.9 days.
Historically, although not absolute, conditions considered high risk of potential complication with systemic anticoagulation (ie, TBI and hemorrhagic shock) have been considered relative contraindications for ECMO.3 Given the high incidence of these injuries among the severely injury, concern may have limited the initial use of ECMO. Recent study though may have contributed to a greater willingness to use the technology. Heparin-free veno-venous ECMO was demonstrated in a case report in 2012 in trauma patients with severe TBI unable to undergo therapeutic anticoagulation without thromboembolic or circuit complication.25 Similarly, in trauma patients with refractory hypoxemia with concomitant hemorrhagic shock undergoing active massive transfusion, Arlt et al 10 reported 10 patients managed with heparin-free ECMO without any report of thromboembolic or circuit clotting. The mean ECMO duration was 5 days with a reported 60% mortality. At our institution, patients are routinely managed without anticoagulation for up to 72 hours. In our recently published study, trauma patients with both TBI and solid organ injury were placed on ECMO with intravenous heparin guided by thromboelastogram to a reactant time twice the baseline. Although we did experience a number of hemorrhagic complications even at this lower level of anticoagulation (40%), most were minor and none contributed to patient mortality. Complications included epistaxis, gastrointestinal bleeding, puncture site/incisional bleeding, and expanding hematoma.24
This study has some limitations. The strength of the analysis is limited by the retrospective design. Additionally, use of the administrative data from the NIS creates multiple limitations inherent to the database itself. Although the data provide evidence of a trend of decreased mortality and increased ECMO utilization, these do not offer any insight into the mechanism behind these trends. Annual differences in hospital inclusion result in inconsistency of the overall data source, creating the possibility of missing data. Finally, the database lacks detailed clinical data and ICD-9 codes only are available for analysis, precluding differentiation between veno-venous and venoarterial ECMO. Therefore, as a result of these factors, insight into the potential underlying reason for treatment and recognition as to which trauma patients may benefit is limited.
Although the use of ECMO in trauma patients with severe ARDS remains controversial, increasing utilization of ECMO nationwide suggests an increasing acceptance and/or increased availability at trauma centers. Corresponding decreasing mortality rates during the study period seem to validate the use of ECMO as a salvage method in trauma patients. Further prospective research is needed to define ideal patient selection and treatment algorithms, and identify strategies to optimize patient outcomes.
References
Footnotes
Contributors PB, PJH, and GM were responsible for study design. GM was responsible for statistical analysis. All authors participated in the critical analysis of the data and manuscript production and review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.