Article Text

Abstract
Background Little is known about long-term functional outcomes of trauma patients in low-income and middle-income countries. In sub-Saharan Africa most studies of injury only collect data through emergency department disposition or hospital discharge, and methods of collecting long-term data are subject to significant bias. With the recent increase in access to mobile telephone technology, we hypothesized that structured, telephone-administered interviews now offer a feasible means to collect data about the long-term functional outcomes of trauma patients in urban Ethiopia.
Methods We piloted a telephone-administered interview tool based on the Glasgow Outcome Scale-Extended. Using departmental logbooks, 400 consecutive patients presenting to two public referral hospitals were identified retrospectively. Demographics, injury data, and telephone numbers were collected from medical records. When a telephone number was available, patients or their surrogates were contacted and interviewed 6 months after their injuries.
Results We were able to contact 47% of subjects or their surrogates, and 97% of those contacted were able and willing to complete an interview. At 6-month follow-up, 22% of subjects had significant persistent functional disability. Many injuries had an ongoing financial impact, with 17% of subjects losing or changing jobs, 18% earning less than they had before their injuries, and 16% requiring ongoing injury-related medical care. Lack of documented telephone numbers and difficulty contacting subjects at recorded telephone numbers were the major obstacles to data collection. Language barriers and respondents’ refusal to participate in the study were not significant limitations.
Discussion In urban Ethiopia, many trauma patients have persistent disability 6 months after their injuries. Telephone-administered interviews offer a promising method of collecting data about the long-term trauma outcomes, including functional status and the financial impact of injury. These data are invaluable for capacity building, quality improvement efforts, and advocacy for injury prevention and trauma care.
Level of evidence III, retrospective cohort study.
- global trauma
- outcomes
- injury
- functional status
- Africa
- research methods
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Injury accounts for over 5 million deaths per year worldwide and 11% of all disability-adjusted life years, and sub-Saharan Africa (SSA) is disproportionally affected.1 2 In SSA, it is difficult to estimate the true burden of trauma because of inadequate surveillance data.3–5 To address this problem, the WHO Guidelines for Essential Trauma Care stress the importance of improved injury surveillance in low-income and middle-income countries (LMIC).6 These data are essential to determine the true burden of injury, evaluate the quality of care being provided, identify targets for performance improvement and systems strengthening, and inform advocacy and injury prevention strategies.7–9
Most studies of injury in Ethiopia and elsewhere in SSA only collect data through emergency department disposition or hospital discharge.10 11 Attempts to describe long-term disability after injury in resource-poor settings are complicated by weak healthcare infrastructure and lack of regular follow-up, although several community-based surveys have suggested that many trauma patients do experience significant long-term disability.12 13 Although little has been published about clinical outcomes of trauma patients in Ethiopia, one study showed that routine delays in both emergent and elective operations resulted in significant preventable death and disability.14
Recent expansion of mobile telephone technology offers a novel opportunity for improved follow-up. The number of mobile telephone subscriptions in Ethiopia has increased rapidly from 400 000 in 2005 to 42 million in 2015, compared with only 1 million land lines.15 Currently, there is nearly one mobile telephone subscription for every two people in Ethiopia. Several previous studies have demonstrated the utility of telephone-administered interviews to collect outcomes data in SSA.16 17 Potential challenges include inaccurately documented telephone numbers, inability to contact patients, language barriers, and patients’ unwillingness to participate in telephone-administered interviews.
We hypothesized that telephone-administered interviews are a feasible method of collecting data about the long-term functional outcomes of trauma patients in urban Ethiopia. The specific objectives of this study were (1) to assess the feasibility of telephone-administered interviews as means of collecting follow-up data in this context; (2) to pilot a telephone-administered interview tool for collecting data about long-term functional outcomes after injury; and (3) to collect preliminary data about patients’ long-term functional outcomes after hospital encounters due to injury.
Methods
Study setting
Ethiopia is a low-income country in East Africa with a population of 90 million, and 37% of the population lives on less than $1.25/day.18 Ethiopia ranks 169 out of 177 on the United Nations Human Development Index, with an annual per capita expenditure on health of $16.19 Addis Ababa is the nation’s capital and largest city, with 3.3 million residents. Amharic is the official working language of the Ethiopian government and the most commonly spoken language in Addis Ababa, although over 80 languages are spoken throughout Ethiopia. Tikur Anbessa Specialized Hospital (TASH) and Menelik II Specialized Hospital (MSH) are public teaching hospitals in Addis Ababa. Both hospitals are affiliated with Addis Ababa University and serve as centers of trauma expertise, seeing a large number of trauma victims from both Addis Ababa and other regions of Ethiopia.
Study design
We conducted a pilot prospective cohort study to determine the feasibility of implementing a novel method of collecting data about the long-term functional outcomes of trauma patients in urban Ethiopia. At each of TASH and MSH, we compiled a list of 200 consecutive patients presenting to the emergency departments with acute injuries, for a total sample size of 400 subjects. At TASH, subjects were identified using an institutional trauma registry. At MSH, subjects were identified using the emergency department registration logbook because an institutional trauma registry did not exist there at that time. For each subject, we performed a retrospective review of emergency department clinical charts and trauma registry data to extract demographics, injury data, and telephone numbers. Those who had missing clinical charts were excluded. Injury severity was quantified using the Kampala Trauma Score (KTS), a simple injury scoring system that incorporates age, systolic blood pressure, respiratory rate, neurologic status, and number of serious injuries.20 KTS has been shown to correlate well with injury severity in resource-poor settings.21–23
When telephone numbers were available, we made up to three attempts to contact a respondent (either the subject or a surrogate, such as a relative, friend, or other caretaker if the subject was unable to respond himself) 6 months after the time of injury. When respondents were successfully contacted, we requested informed consent and interviewed the respondent about the subject’s current functional status using a standardized interview tool based on the Glasgow Outcome Scale-Extended (GOSE), a well-validated and widely used metric of functional status.24 25 GOSE assigns a score of 1 to 8, with scores of 7 to 8 representing good recovery.25 GOSE was originally designed for patients who had sustained neurologic trauma, but has since been implemented with a wide variety of trauma patients.26–28 Its administration via telephone has been studied in other countries with good validity.29 Whereas its use in SSA has not been well studied, it has been used to measure functional outcomes among trauma patients in other LMIC.30
A structured interview tool based on GOSE was developed for telephone use in Ethiopia for this study. The interview tool also included exploratory questions addressing subjects’ preinjury and postinjury work status and income and follow-up medical care (online supplementary appendix 1). Interviews were composed of 10 to 20 questions, depending on the responses. The interview tool and a verbal informed consent document were translated to Amharic and back-translated to English by medical professionals and were revised to ensure accuracy. The interview tool was piloted with 20 subjects and further revised to ensure clarity.
Supplemental material
Statistical analysis
Data were tabulated in a FileMaker Pro V.13 database and imported into Stata V.13 for analysis. We used Student’s t-test, Fisher’s exact test, χ2 analysis, and multivariable logistic regression to compare subjects who were and were not successfully interviewed, and to compare those who did and did not make a good recovery. P values <0.05 were considered statistically significant.
Results
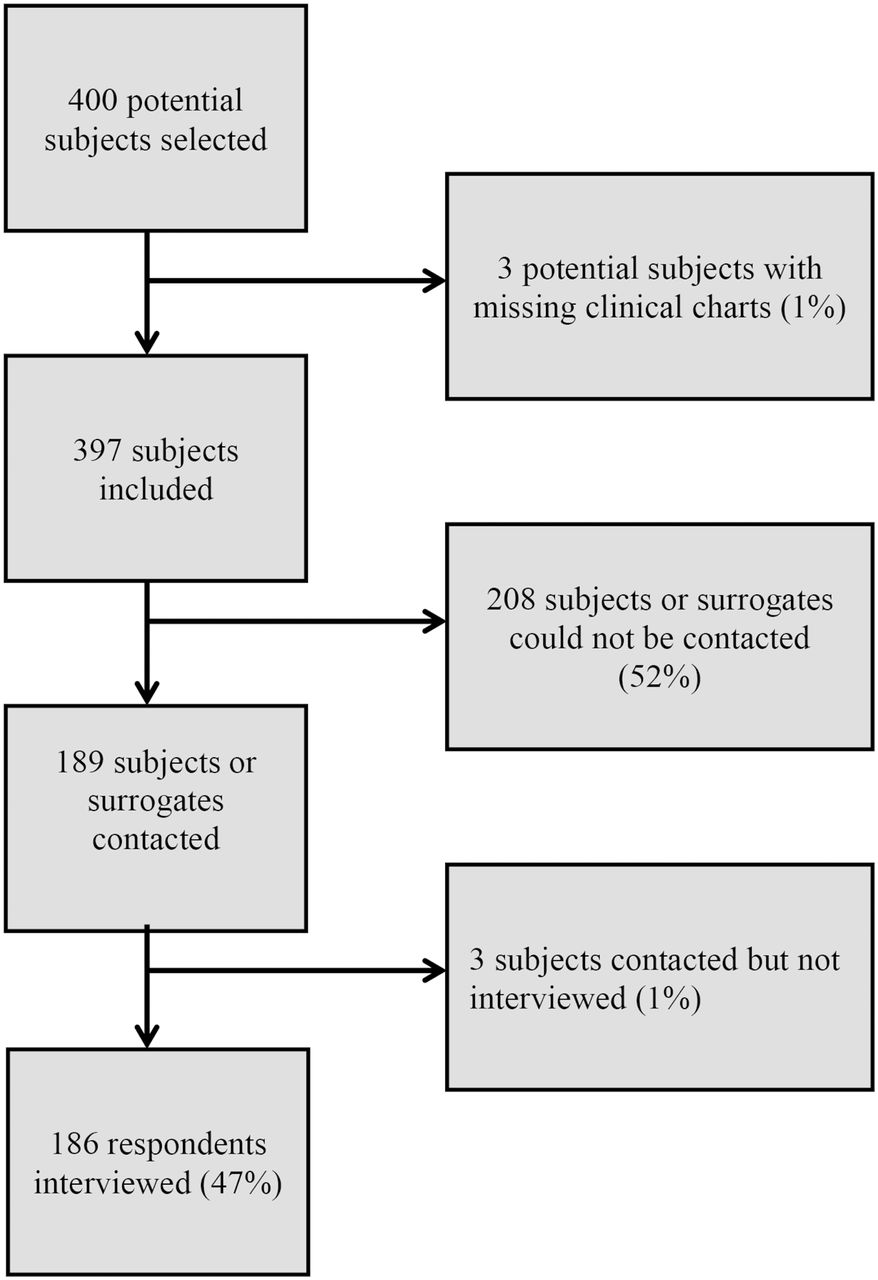
Of 400 subjects identified from hospital records, we were able to locate hospital charts and retrospectively extract demographic and injury data and telephone numbers for 397. We were able to establish contact with the subject or a surrogate as a potential respondent for 189 (47%) of those 397 subjects (figure 1). Of the 208 subjects for whom we were unable to contact a potential respondent, our data clerks recorded a reason 131 times (63%). Of those, 92 (70%) did not have a valid telephone number on file, 37 (28%) had a telephone line that was out of service or was not answered on three attempts, and 2 (2%) had a telephone number that was answered by someone who did not know the current condition of the subject or how to contact them.

Flow diagram of subjects included in the study. Subjects include all those for whom retrospective data extraction from clinical charts was performed; respondents include only those who completed a telephone-administered follow-up interview.
Among 189 potential respondents who we contacted, only 3 did not complete an interview (2%). One potential respondent did not consent to participate in the study, one potential respondent from the Somali region of Ethiopia was unable to participate due to language barrier, and one potential respondent consented to participate in the study but did not complete the interview.
Excluding these three potential respondents, we were able to complete interviews with 186 respondents. The respondent was the subject on 104 occasions (56%) and a surrogate on the remaining 82 occasions (44%). Interviews lasted a mean of 5.9 min (SD 1.5), and only one interview lasted longer than 10 min.
Subject demographics and injury data are summarized in table 1. Most subjects were male (84%). The mean age was 32.8 years (SD 14.8). Subjects included residents of 7 of Ethiopia’s 11 regions, with the majority from Addis Ababa (74%) and most others from Oromiya (18%) and Amhara (5%). Regarding injury types, 41% of the subjects suffered isolated soft tissue injuries, 28% suffered injuries to the extremities or bony pelvis, 28% suffered injuries to the head or spine, and 6% suffered thoracoabdominal injuries. Only 4% of the subjects had multiple injury types. We were able to calculate KTS to quantify injury severity for 342 subjects (86%), and the majority of subjects had mild injury severity (95%). Comparing subjects who we were able to contact and complete an interview with those who we were not, there were no significant differences in age, sex, region of residence, injury type, or injury severity.
Demographics and injury characteristics of study subjects
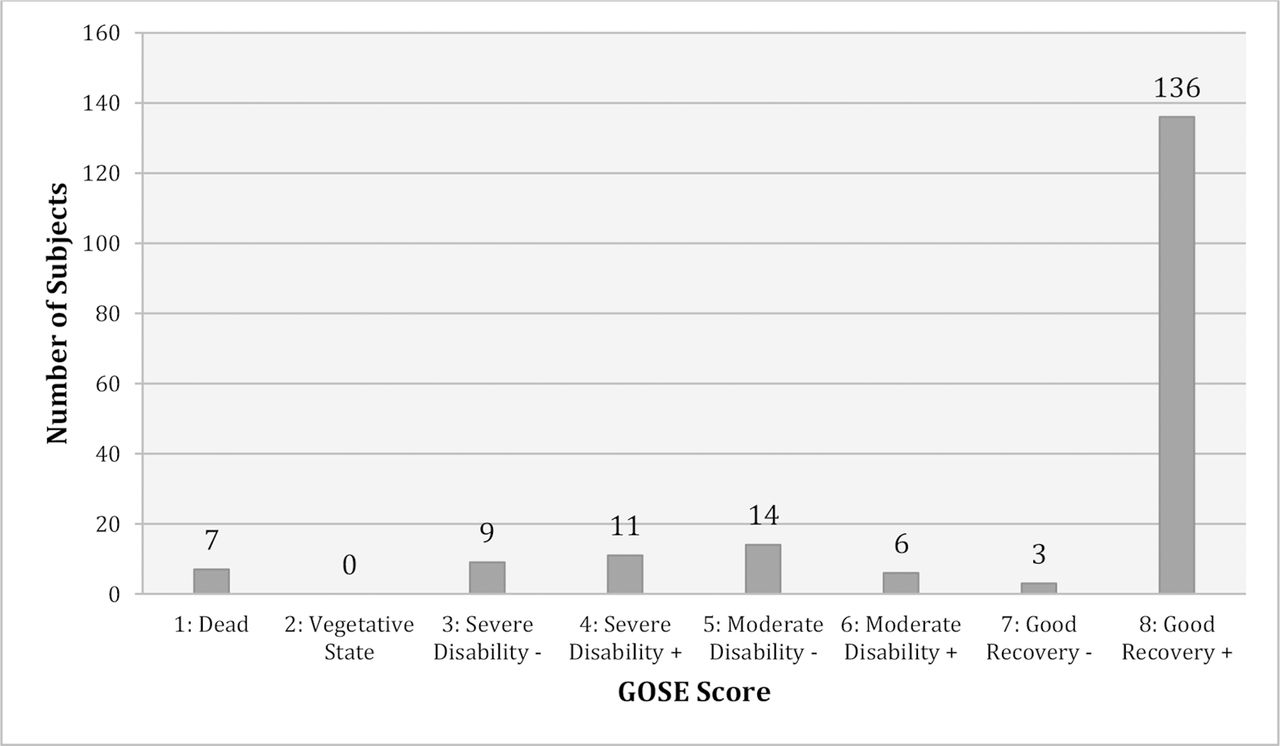
Figure 2 represents the long-term functional outcome of subjects. At 6 months, 139 subjects (75%) had made a good recovery (GOSE score 7–8). Seven subjects (4%) had died since their injuries. The remaining 22% had a significant degree of disability 6 months after discharge, including 20 subjects (11%) with moderate disability (GOSE score 5–6) and 20 subjects (11%) with severe disability (GOSE score 2–4). Subjects who made a good recovery were significantly more likely to have suffered isolated soft tissue injuries (87% vs. 65%, p<0.01) and to have had a mild injury severity (80% vs. 17%, p<0.01). Subjects with injuries to the head or spine were significantly less likely to make a good recovery (57% vs. 81%, p<0.01).

{kind=link}
{kind=link}
Six-month functional outcome of subjects, quantified by GOSE score. GOSE, Glasgow Outcome Scale-Extended.
Of the 90% of the respondents who provided information about employment, 17% had lost or changed jobs after their injuries. Of the 85% of the respondents who provided information about income, 18% earned less than they did before their injuries. The majority of subjects (169, 90%) had at least one follow-up visit after their injury, although few had four or more follow-up visits (19, 10%). Information on ongoing medical care was provided by 90% of respondents, 16% of whom required ongoing injury-related medical care. In unadjusted comparisons, those who made a good recovery by GOSE criteria were significantly more likely to continue working in the same job than those with worse recovery (97% vs. 35%, p<0.01), to continue to earn a similar salary than those with worse recovery (95% vs. 35%, p<0.01), and to no longer need medical care (96% vs. 36%, p<0.01).
Discussion
In this study, 25% of trauma patients treated in urban Ethiopian emergency departments had died or had persistent functional disability at 6 months. Additionally, 17% had lost or changed jobs and 18% had a decrease in wages after being injured. Poor long-term functional outcomes were associated with more severe injuries and injuries to the head and spine, as we expected. However, 20% of subjects with mild injury severity and 13% of those with isolated soft tissue injuries had not made a good recovery 6 months after their injuries, demonstrating that even mild injuries may be associated with significant long-term morbidity and socioeconomic consequences in this context. Improved trauma care and rehabilitation services in Ethiopia may reduce the long-term burden of injury and mitigate its socioeconomic impact.
Very little has been previously published about long-term functional outcomes of trauma patients in SSA. Although the implementation of trauma registries has improved injury surveillance in LMIC, very few collect data on disability.11 Many studies describing trauma in LMIC only collect short-term outcomes including disposition from the emergency department, length of stay, and hospital mortality.31–33 The few hospital-based studies that have addressed post-traumatic disability in LMIC have assessed patients at the time of discharge, using a variety of metrics including the Glasgow Outcome Scale in Jamaica,30 the Barthel Index and Musculoskeletal Function Assessment index in Malaysia,34 and the Mock Trauma Disability Scale and Language Independent Functional Evaluation score in Ghana.35
Although little has been published about the long-term impact of injury in LMIC, several community-based surveys have suggested that trauma results in long-term disability that places a substantial burden on victims and their communities. For example, Mock et al 12 found that in 7% of households surveyed in Ghana someone had suffered an injury resulting in loss of normal activity in the past year, that injuries resulted in over a month of disability on average, and that injuries frequently required family members to take time off from their usual activities to assist the injured person. Moshiro et al 36 found that in Tanzania there were 33 injuries per 1000 persons per year, with 27% of trauma victims with disability lasting longer than 30 days. Juillard et al 13 found that in Nigeria there were 42 road traffic injuries per 1000 persons in the previous year, with 29% of injuries resulting in prolonged disability, 20% of victims missing over 1 month of work, and another 14% unable to return to work altogether. These findings are similar in scope to the rates of persistent disability in 22% and decreased earnings in 18% that are reported here. Previous studies have suggested that difficulty accessing appropriate care and inadequate physical therapy and rehabilitation services contribute to long-term physical disability and emotional distress after injuries in LMIC.35 37 38
This pilot study demonstrates that structured, GOSE-based, telephone-administered interviews offer a promising method of collecting data about the long-term functional outcomes of trauma patients in urban Ethiopia. It is novel in its ability to evaluate long-term functional outcomes of a cohort of trauma patients in SSA, and unique in compiling data from a hospital-based cohort of nearly 200 subjects. Language barriers and patient refusal to participate in the study were not significant barriers to interview administration, as we had feared they might be.
The major barrier to this methodology in our setting was our inability to contact a potential respondent for slightly over half of our subjects. The retrospective method of subject selection in this study limited our ability to investigate this issue, although we think that often we were unable to contact a potential respondent because the telephone numbers recorded in our clinical charts were those of emergency contacts or the acquaintance or bystander who brought the patient to the emergency department and not of the patients themselves. It is also possible that we missed some potential respondents who did not answer telephone calls from numbers that they did not recognize. In the future, researchers using telephone-administered follow-up interviews in similar settings should notify potential subjects prior to hospital discharge and ensure that reliable telephone numbers have been recorded.
Our research methodology has several promising applications. It offers a means of collecting data to inform efforts to expand capacity and improve the quality of trauma care in LMIC. Comparing functional outcomes over time will also allow providers to assess the impact of their efforts. This methodology can also be used to determine which types of injury result in the most disability to inform injury prevention strategies. Finally, by more accurately determining the long-term impact of injuries in LMIC, we can advocate for resources for injury prevention and trauma care commensurate with the true burden of injury. An important next step in using telephone-administered interviews to collect long-term data about trauma patients in SSA is the formal validation of GOSE and the telephone-administered interview methodology in this setting.
Conclusion
This pilot study found a substantial burden of long-term functional disability and associated socioeconomic consequences 6 months after injury in urban Ethiopia. These consequences of injury often go under-reported and underestimated in LMIC. Telephone-administered interviews using an interview tool based on GOSE offer a promising method of collecting data about the long-term functional outcomes and the socioeconomic impact of injury experienced by trauma victims in LMIC. These data are invaluable for capacity building, quality improvement efforts, and advocacy for injury prevention and trauma care.
Acknowledgments
We gratefully thank Dr Gerard O’Reilly of Monash University for his help conceptualizing an early version of this study.
References
Footnotes
Presented at This research was presented at the 4th World Trauma Congress in San Diego, California, on September 28, 2018.
Contributors All authors meet the ICMJE criteria for authorship. ADL, CJJ, and RAD participated in the conception and design of the study. ADL, NS, AA, and AZ participated in the acquisition of data. All authors participated in the analysis and interpretation of data. ADL drafted the article. NS, AA, AZ, CJJ, and RAD participated in the critical revision of the article. All authors approved of the final version of the article.
Funding This project was supported by the NIH Fogarty International Center (Grant #R25TW009338) under the Global Health Equity Scholars Consortium.
Competing interests None declared.
Patient consent Informed consent for telephone-administered interviews was obtained verbally at the time of interview.
Ethics approval The study protocol was reviewed and approved by the Institutional Review Board at Addis Ababa University and the Committee on Human Research at the University of California, San Francisco.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement There are no additional unpublished data from the study which are available to share.