Article Text

Statistics from Altmetric.com
Case description
A middle-aged woman with a history of right breast lobular carcinoma in situ who underwent bilateral mastectomy in 2000 and implant revision on March 3, 2022 presented to our hospital after 4 hours of postprandial nausea and vomiting. Specifically, she developed sudden-onset nausea and high-volume, non-bloody, non-bilious emesis after eating dinner. She also had obstipation and worsening abdominal distention. Her labs were significant for a white cell count of 13.8 x109/L. Her CT scan demonstrated dilated loops of proximal to mid-small bowel measuring up to 2.9 cm. A loop of bowel was identified to be extending into the lesser sac through the foramen of Winslow, and there was an abrupt transition point as the small bowel entered and exited the foramen of Winslow (figure 1A,B). These findings were concerning for an internal hernia through the foramen of Winslow (figure 2).
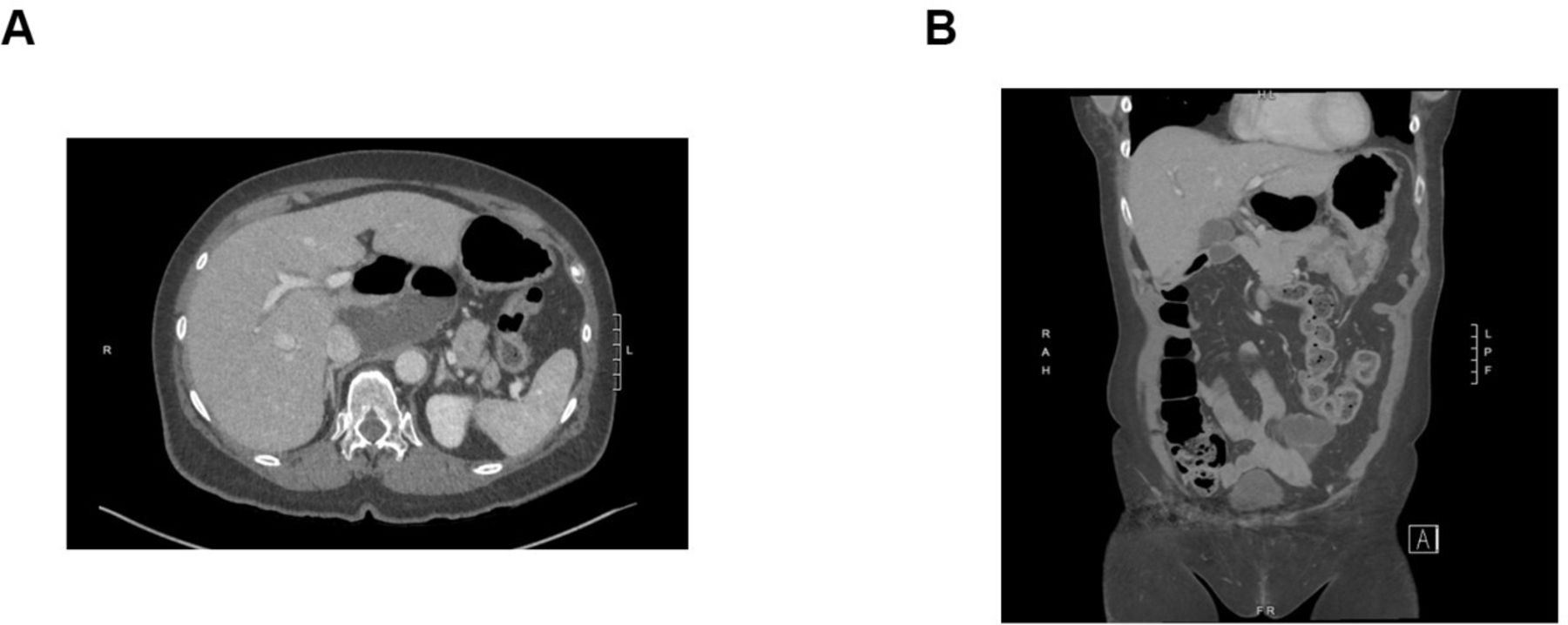
(A) Axial section through the upper abdomen showing the dilated small bowel. (B) Coronal section demonstrating the dilated small bowel and the hernia through the foramen of Winslow.

A diagram of the foramen of Winslow hernia in this patient.
The foramen of Winslow, also known as epiploic foramen, allows communication between the greater and lesser peritoneal cavities. Anatomically, it is defined by the free border of the hepatoduodenal ligament anteriorly, the inferior vena cava covered by the peritoneum posteriorly, the caudate lobe superiorly, and the first portion of the duodenum and the hepatic artery inferiorly (figure 2). Under normal circumstances, the foramen of Winslow remains closed as a result of the intra-abdominal pressure that does not allow the viscera to herniate, although in rare circumstances abdominal contents can herniate through. Foramen of Winslow hernias make up less than 1% of all hernias. The non-specific abdominal symptoms associated with this type of hernia as well as its rarity make the diagnosis difficult without axial imaging.
What would you do next?
Diagnostic laparoscopy and reduction of hernia
Diagnostic laparoscopy, reduction of hernia, and hernia repair
Exploratory laparotomy and reduction of hernia
Exploratory laparotomy, reduction of hernia, and hernia repair
What we did and why
B. Diagnostic laparoscopy, reduction of hernia, and hernia repair
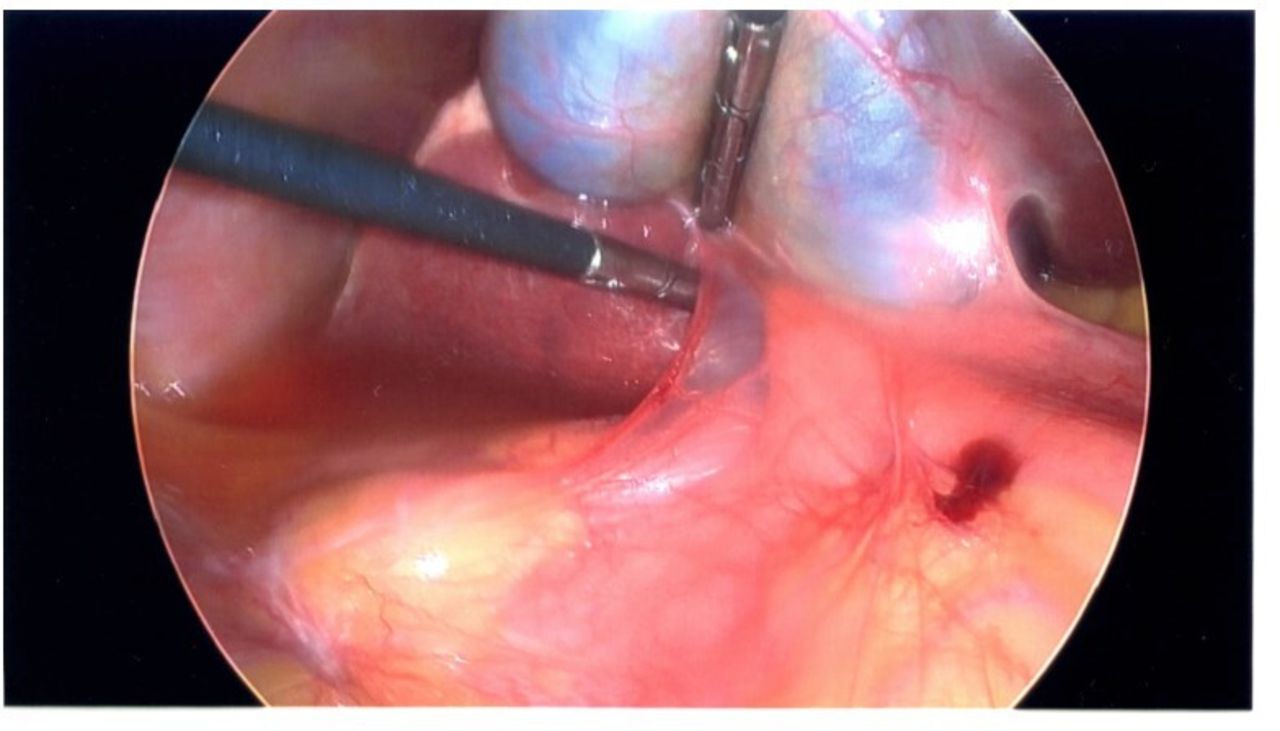
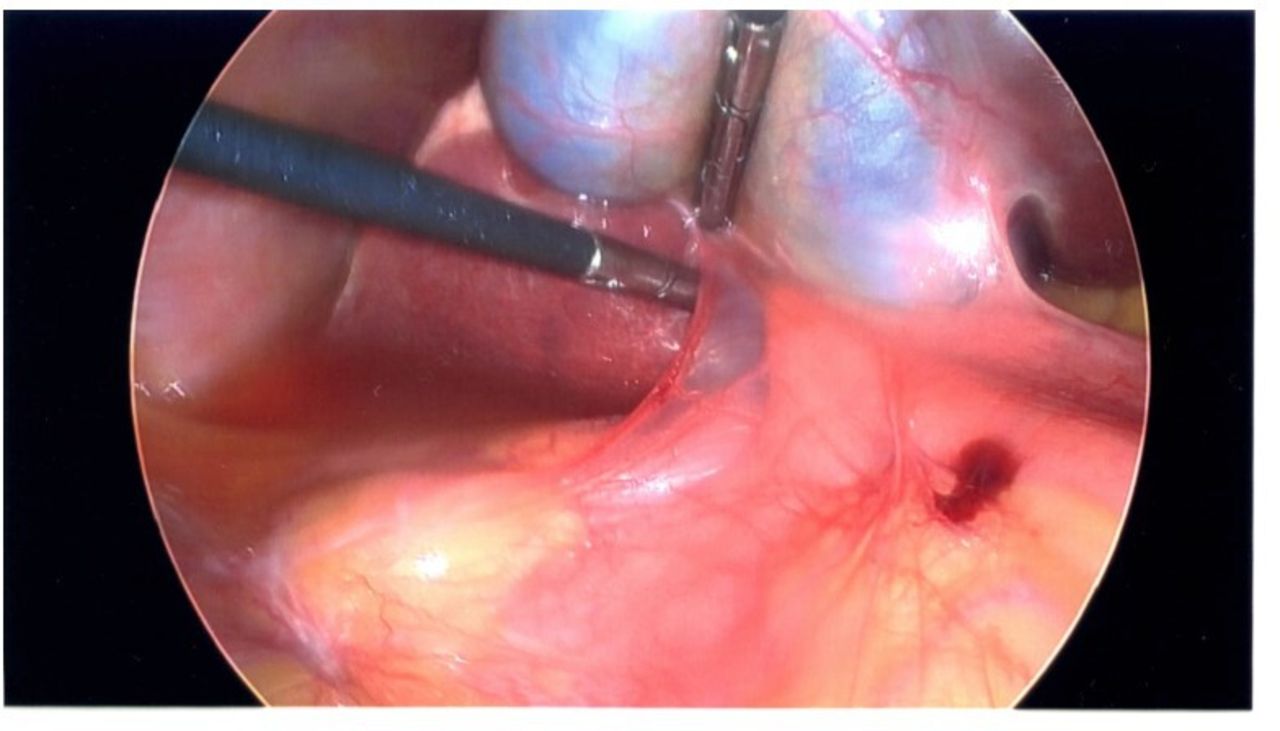
After placing a nasogastric tube in the emergency department, we chose to perform a diagnostic laparoscopy to evaluate the likely hernia. We entered the abdomen via the Palmer’s point and placed a Veress needle. After performing the saline drop test, we insufflated the abdomen to 15 mm Hg. We entered the abdomen infraumbilically with a 5 mm Optiview port and confirmed that our needle entry was atraumatic. We placed two additional 5 mm ports in the right upper quadrant. We then identified an internal hernia through the foramen of Winslow. The bowel appeared to enter just lateral to the gall bladder. There were some adhesions seen from the gall bladder to the duodenum. The bowel in the hernia appeared viable and we were able to gently reduce the hernia. Once the hernia was reduced we were able to identify the defect, as shown in figure 3. Previously, literature regarding the closure of hernia through the foramen of Winslow is mixed; however, we opted to close it as there were two clear areas that could be reapproximated to close the defect. To facilitate closure of the defect, we placed a 12 mm port within the mid-upper abdomen. We sutured the adhesive tissue just lateral to the gall bladder to the tissue just below it to attempt to close the defect using a 3-0 -locking vicryl suture. We suctioned out the reactive ascites. We closed the 12 mm port with a 0 braided absorbable suture via a laparoscopic suture passer. The skin was closed with absorbable suture. The nasogastric tube was removed. The patient was able to tolerate oral intake on postoperative day 0 and was discharged that very same day.
{kind=link}
{kind=link}
{kind=link}
Intraoperative image. Laparoscopic instrument demonstrating the location of the internal hernia where the bowel was reduced out of.
Overall, this case demonstrated lessons on diagnosis and management of a rare internal hernia.
Ethics statements
Patient consent for publication
Footnotes
Contributors ALT is the first author and was responsible for drafting the article. ALT and JMG are both surgical residents who were involved in the case and provided critical revisions. DS is the senior author and the attending surgeon who contributed to patient care and decision-making and was responsible for project oversight.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.