Article Text

Abstract
Objectives The goal of this study was to explore the incidence of overtransfusion in trauma patients requiring massive transfusion protocol (MTP) activation and identify modifiable risk factors. We hypothesized that overtransfusion is common after MTP activation.
Methods Patients admitted to a level I trauma center from July 2016 to December 2019 and who required MTP activation were selected. The primary outcome was overtransfusion, defined as a hemoglobin (Hg) ≥11 g/dL at 24 hours (±2 hours). A Cox regression model was used to identify independent risk factors for overtransfusion.
Results 140 patients met inclusion criteria. The median age was 39.0 years, with the majority (74.3%) being male. The median (IQR) Injury Severity Score (ISS) was 24.0 (58.0) and 38.4% had a penetrating mechanism. The median (IQR) admission Hg was 12.6 (11.7) g/dL. Overall, 71.4% of patients were overtransfused by the conclusion of MTP, 43.6% 24 hours later, and 29.5% at discharge. Overtransfusion did not correlate with the number of units of blood transfused nor with the duration of MTP. Overtransfused patients at 24 hours after the conclusion of MTP were significantly more likely to present with a penetrating injury (52.5% vs. 27.3%, p=0.003) and have a significantly lower ISS (median (IQR) 18.5 (44.0) vs. 26.0 (58.0), p=0.035.) In a Cox regression model, penetrating mechanism (adjusted HR (AHR): 2.93; adjusted p=0.004) and admission base excess (BE) (AHR: 1.15; adjusted p=0.001) were the only variables independently associated with overtransfusion.
Conclusions Overtransfusion of trauma patients requiring MTP activation is highly common, leading to overutilization of a limited resource. Penetrating trauma and BE may be modifiable risk factors that can help limit overtransfusion. Overtransfusion should be tracked as a data point by blood banks and trauma centers and be further studied as a potential quality metric for the resuscitation of massively transfused trauma patients.
Level of evidence III.
- blood transfusion
- quality improvement
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Although massive transfusion protocols may improve survival in trauma patients, their use may lead to overtransfusion practices, the extent of which remains largely understudied.
WHAT THIS STUDY ADDS
By defining autotransfusion as a hemoglobin level of 11 g/dL, we found that among trauma patients requiring massive transfusion protocol, over 7 out of 10 were overtransfused by the conclusion of the protocol, over 4 out of 10 by 24 hours later, and approximately 3 out of 10 at discharge.
Penetrating mechanism and high base deficit were independently associated with overtransfusion at 24 hours after the conclusion of the massive transfusion protocol.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Overtransfusion should be tracked as a data point by blood banks and trauma centers and be further studied as a potential quality metric for the resuscitation of massively transfused trauma patients.
Introduction
The introduction of massive transfusion protocols (MTPs) by trauma centers for the initial resuscitation of exanguinating trauma patients has resulted in achieving early delivery of balanced resuscitation with blood products,1 2 which in turn has led to improved survival of this high risk for mortality patient population.3 4 Early delivery of the MTP coolers is considered a quality metric, as every minute delay increases substantially the odds for mortality.5 Although the life-saving impact of their use in this setting is undeniable, transfusion of blood products may be associated with adverse reactions, ranging from volume overload, to hemolysis, infections, immunosuppression, and even death.6–8 In fact, each unit of blood delivered to massively transfused trauma patients in the first 24 hours independently increase the risk of infectious complications by 7.6%.9 Among trauma patients who receive over 10 units of blood within the first 24 hours, those who are overtransfused have comparable mortality with those who are undertransfused.10 Despite this, upwards of one-third of patients presenting with major trauma receive a potentially avoidable blood transfusion.11 12 Limiting unnecessary transfusions is important to avoid exposing an already at high-risk patient population, to additional, life-threatening risks, and to minimize overutilization of available resources.
MTP coolers allow the trauma team to have readily available and at hand blood products which they administer based on their interpretation of the patient’s physiologic status, estimated blood loss, laboratory parameters, and a multitude of other factors that are taken collectively into account to assess hemodynamic and perfusion targets.13 14 Despite the availability of these factors, the decision to terminate additional transfusion of blood products remains largely subjective, as no one parameter can decisively guide clinicians to cease transfusions. This, in combination with the availability and easy accessibility of blood products provided with the MTP, may lead to overtransfusions with all the possible consequences, not only due to the adverse impact on outcomes, but also due to the increased cost and wastage of this limited resource.
The goal of this study was to explore the incidence of overtransfusion in trauma patients requiring MTP activation at a mature trauma center and identify modifiable risk factors. We hypothesized that overtransfusion is common after MTP activation.
Study design and methods
The trauma registry was queried for patients admitted to our level I trauma center from July 2016 to December 2019 and who required MTP activation. Patients who died within 24 hours from admission, those who did not receive any blood products from the MTP coolers, those with MTP duration that exceeded 24 hours, and those with unavailable hemoglobin (Hg) value at 24 hours (±2 hours) after the conclusion of the MTP activation were excluded.
MTP at our center is activated at the discretion of the trauma surgeon. While awaiting the MTP coolers, the trauma team has access to uncrossmatched packed red blood cells (pRBCs) stored in a refrigerator in the emergency department (ED). The MTP coolers are delivered within 10 minutes from the time they are requested and they contain 12 units of pRBCs, 12 units of plasma, and 1 unit of pheresis platelets at room temperature. Up to 4 units of low-titer, group O whole blood (LTOWB) may be included, depending on availability and would replace an equal number of pRBCs. A unit of thawed cryoprecipitate is delivered within 30 minutes from delivery of the MTP coolers. The conclusion of the MTP activation is clinician dependent and is based on the time that the coolers are returned to the blood bank.
Demographics (age, gender) and injury characteristics (mechanism (blunt vs. penetrating), Injury Severity Score (ISS), Abbreviated Injury Scale (AIS) score for body regions head, chest, abdomen, and extremities), along with admission vital signs (ED systolic blood pressure (SBP), Shock Index (defined as admission heart rate divided by admission SBP), Glasgow Coma Scale score), ED disposition (operating room (OR), interventional radiology (IR), intensive care unit, or other), and MTP logistical data (time to delivery and duration) were tabulated on an Excel spreadsheet. Laboratory values for Hg, platelet count, pH, base excess (BE), lactate, and international normalized ratio (INR) were collected for four different phases of hospitalization: admission (first available values), at the conclusion of MTP activation (within 2 hours from return of the MTP coolers to the blood bank), 24 hours after conclusion of MTP activation (±2 hours), and at discharge (day of discharge from hospital). Point-of-care Hg values were not accounted for. At our county, the prehospital personnel have no access to blood products. Therefore, the admission Hg reflects the level prior to any blood product transfusion, as admission labs are universally obtained on all trauma patients within a very short period of time after arrival to the ED. For calculation and depiction purposes, all Hg values were rounded to their nearest integer values. Additional data points included use of any vasopressor during MTP and at its conclusion. Lastly, all transfusion data were collected and included:
Transfusion of uncrossmatched pRBC units that are available in the ED refrigerator, used in the time period between MTP activation and delivery of the coolers.
Transfusion of pRBCs, LTOWB, plasma, pheresis platelets, and cryoprecipitate included in the MTP cooler. Each unit of LTOWB was considered equal to a unit of pRBC for calculation purposes.
Transfusion of pRBCs, plasma, pheresis platelets, and cryoprecipitate during the remainder hospital stay, after the conclusion of MTP.
The primary outcome was overtransfusion, defined as a Hg ≥11 g/dL at 24 hours (±2 hours) after the conclusion of MTP activation. Secondary outcomes were overtransfusion (Hg ≥11 g/dL) at the conclusion of MTP and at discharge. We used the cut-off of 11 g/dL as we thought that it was significantly higher than 8 g/dL that is targeted for critically ill patients who are hemodynamically normal and who do not experience ongoing bleeding. At the same time, this level allows for additional transfusions over the level of 8 g/dL in the case of uncertainty with quantifying adequate resuscitation after control of bleeding. This definition was based on an Hg value, rather than on physiologic or other parameters. Our intention was to evaluate overtransfusion as a clinical event, rather than as a predictor of mortality. The largely variable mortality rate based on an Hg value in our cohort did not follow a certain trend and did not allow for identification of a reliable inflection point to help define overtransfusion based on this outcome (online supplemental appendix 1). In addition, the n for values of Hg >12 g/dL decreased substantially, not allowing for a meaningful statistical analysis (for example, there was only one patient with an Hg of 15 g/dL and three with an Hg of 16 g/dL). Lastly, when we compared mortality of patients with various cut-offs of Hg, we found no statistical difference for Hg values of 10, 11, and 12 g/dL (online supplemental appendix 2). We therefore selected an Hg value of 11 g/dL to define overtransfusion as the most clinically relevant and most meaningful for statistical analysis purposes.
Supplemental material
Supplemental material
A forward linear regression model was used to identify correlations between the number of pRBC units transfused and duration of MTP with overtransfusion. Overtransfused patients (Hg ≥11 g/dL at 24 hours after MTP conclusion) were then compared with their non-overtransfused counterparts. Proportions were compared using Χ2 or Fisher’s exact test and means were compared using t-test or Mann-Whitney test. A p less than 0.050 was considered statistically significant. A Cox regression model including all variables different between the two cohorts at a p level of <0.2 was used to identify independent risk factors for overtransfusion. Data were analyzed using the IBM SPSS Statistics for Windows, V.25.0 (IBM Corp).
Results
During the 42-month study period, 240 trauma patients required MTP activation. Of those, 28 did not require any blood products, and the remaining 72 died within less than 24 hours, with the vast majority (97.2%) not having a repeat Hg. Therefore, after applying our exclusion criteria, 140 patients were left for analysis. The median (IQR) age was 39.0 (83.0) years, with the majority (N=104 or 74.3%) being male. The median (IQR) ISS was 24.0 (58.0), and 38.4% (n=53) suffered a penetrating mechanism of injury. The median (IQR) admission Hg was 12.6 (11.7) g/dL, whereas the median (IQR) pH was 7.28 (0.73), BE was −8.0 (32.0), and lactate was 4.0 (23.4) mg/dL.
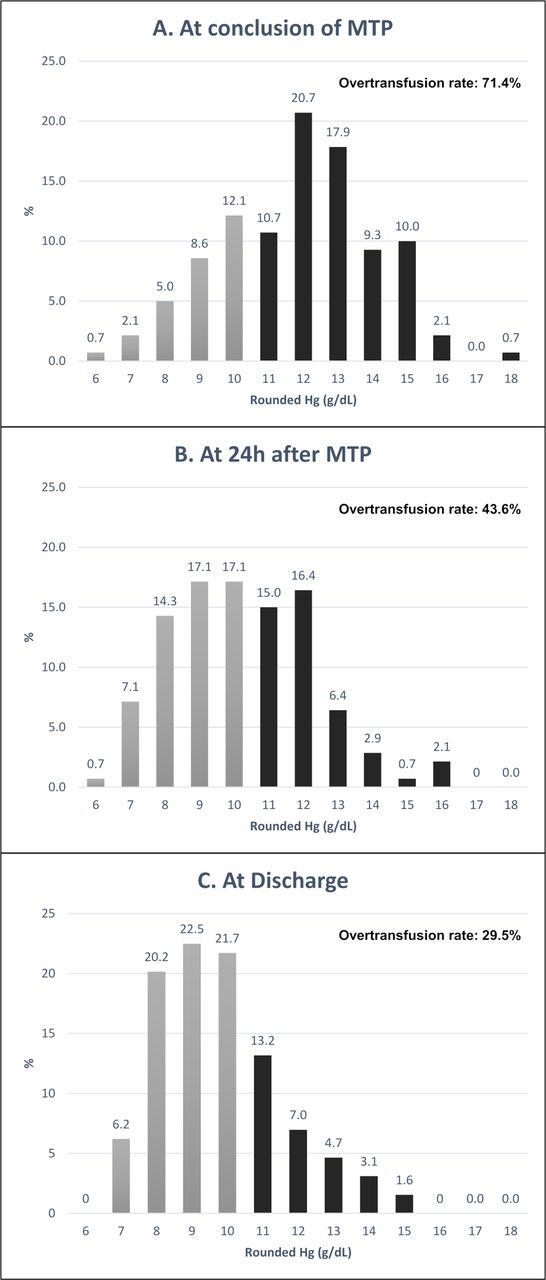
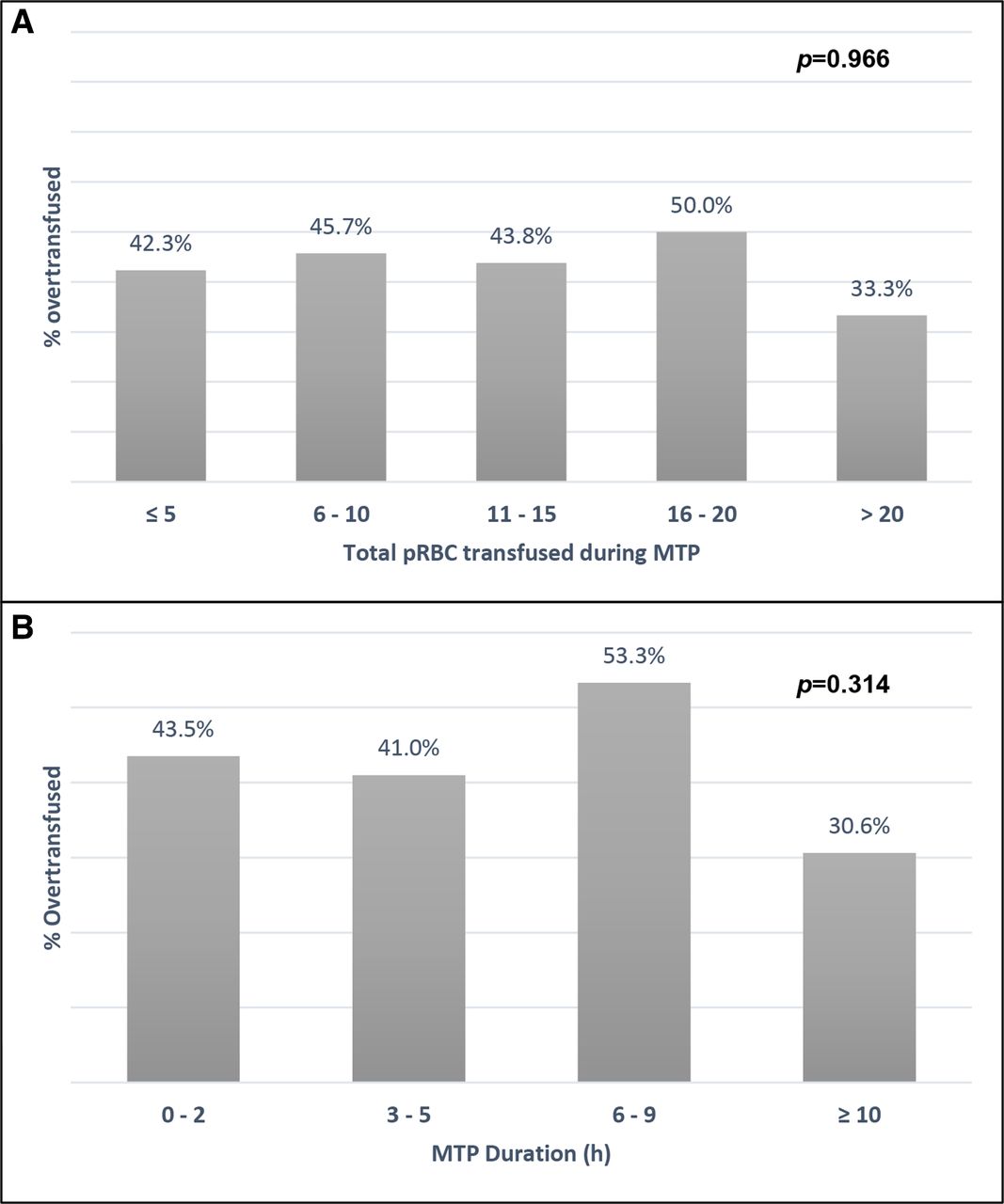
Figure 1 depicts the proportion of patients with rounded Hg levels between 6 and 18 g/dL at the time of MTP conclusion, 24 hours later, and at discharge. Overall, 71.4% of patients were found to be overtransfused by the conclusion of MTP, 43.6% 24 hours later, and 29.5% at discharge. Figure 2 depicts the proportion of overtransfused patients based on the number of pRBCs transfused during the MTP phase and the duration of MTP activation. None of these two variables correlated with overtransfusion in a linear regression model (R2 <0.001 and 0.009, respectively, and p=0.882 and p=0.274, respectively).
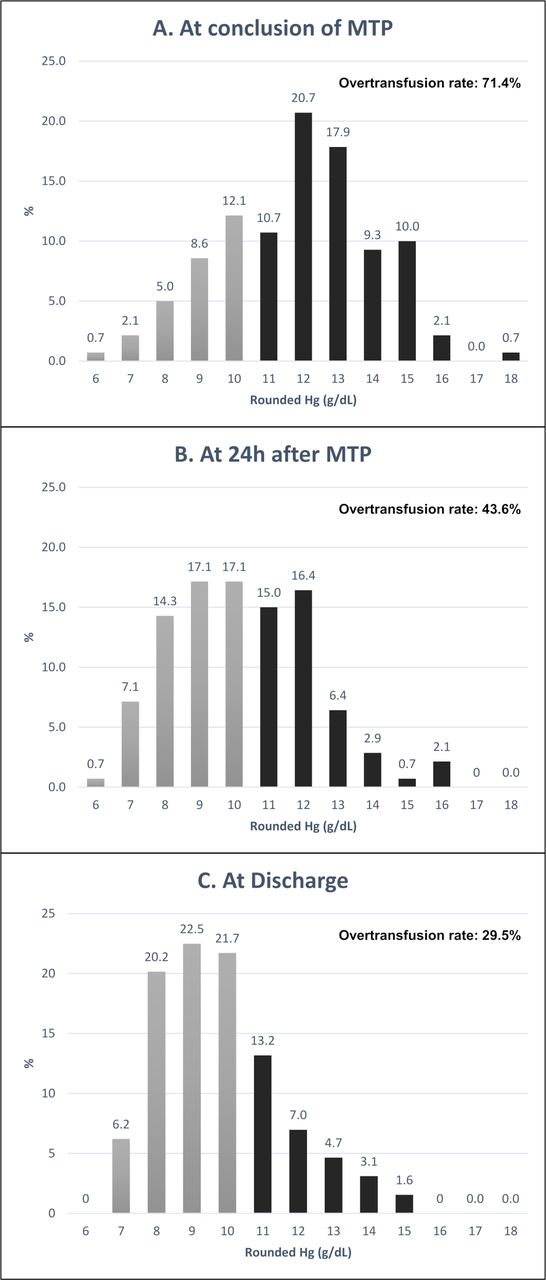
Proportion of patients with rounded hemoglobin (Hg) levels between 6 and 18 g/dL and rate of overtransfusion (Hg ≥11 g/dL) at three phases of hospitalization: (A) at the conclusion of the massive transfusion protocol (MTP), (B) 24 hours after the conclusion of MTP, and (C) at discharge.

{kind=link}
{kind=link}
Proportion of overtransfused patients (Hg ≥11 g/dL) at 24 hours after the conclusion of the massive transfusion protocol (MTP) based (A) on the total number of packed red blood cells (pRBCs) transfused during the MTP phase and (B) on the duration of MTP in hours. Hg, hemoglobin.
Overall, 61 patients (43.6%) were overtransfused at 24 hours after the conclusion of the MTP phase. Age, gender, and ED admission vital signs were similar between overtransfused and non-overtransfused patients (table 1.) Overtransfused patients, however, were significantly more likely to present with a penetrating injury (52.5% vs. 27.3%, p=0.003) and have a significantly lower ISS (median (IQR) 18.5 (44.0) vs. 26.0 (58.0), p=0.035). There was no difference in the proportion of patients requiring emergency operative or radiology-guided intervention. However, when comparing blunt and penetrating trauma patients, those with a penetrating injury were significantly more likely to require emergent operative intervention (38 of 53 or 71.7% for penetrating and 32 of 85 or 37.6% for blunt, p=0.002.) A total of 42 patients (30.0%) required vasopressors prior to the delivery of the MTP coolers and this proportion was similar between the two groups (table 1.) The median (IQR) time from activating MTP to the delivery of the coolers was 10.0 (28.0) minutes, whereas the median (IQR) duration of MTP activation was 5.4 (23.0) hours.
Comparison of baseline demographics and injury characteristics between overtransfused and non-overtransfused patients
Table 2 outlines the laboratory values for the two cohorts at various phases of hospitalization. Overtransfused patients had a significantly higher median (IQR) Hg at admission compared with non-overtransfused patients (12.8 (11.7) vs. 12.0 (9.4), p=0.017.) The BE tended to be lower for overtransfused patients, however, the difference did not reach statistical significance (−6.0 (25.0) vs. −9.0 (32.0), p=0.053). At the conclusion of MTP, overtransfused patients had, as expected based on our definition, a significantly higher Hg (13.4 (8.1) vs. 10.5 (8.1), p<0.001) and a significantly lower INR (1.3 (2.2) vs. 1.4 (1.9), p=0.010). Otherwise, the platelet count, pH, BE, and lactate were similar. At 24 hours after the conclusion of the MTP phase, overtransfused patients had a significantly higher median (IQR) platelet count (122.0 (301.0) vs. 109.0 (272.0), p=0.040), but all other examined laboratory parameters were similar. At discharge, overtransfused patients had a significantly higher median (IQR) Hg (10.3 (8.8) vs. 8.9 (6.4), p<0.001).
Comparison of laboratory values between overtransfused and non-overtransfused patients at four different phases of hospitalization
With respect to the number of blood products transfused, there were no statistically significant differences between the two groups. Both received a similar number of pRBCs, plasma, platelets, and cryoprecipitate, independent of the phase of hospitalization/resuscitation. Overtransfused patients tended to receive a lower median (IQR) number of pRBCs after the conclusion of the MTP phase and during the remainder of their hospital stay, but this difference did not reach statistical significance (0.0 (40.0) vs. 3.0 (43.0), p=0.052) (table 3.) The proportion of patients who received massive transfusion, defined as 10 or more units of pRBCs within 24 hours was 26.4% (n=37 of 140), and was similar between the two cohorts (29.5% vs. 24.1%, p=0.468). The overall mortality was 15.0%: 11.5% for overtransfused patients and 17.7% for non-overtransfused (p=0.305).
Comparison of transfused blood products between overtransfused and non-overtransfused patients
In a Cox regression model including all variables with a p<0.2 (ie, gender, mechanism (blunt vs. penetrating), ISS, AIS chest, AIS abdomen, AIS extremities, admission Hg, admission lactate, and admission BE), penetrating mechanism (adjusted HR: 2.93; 95% CI: 1.42 to 6.07; adjusted p=0.004) and admission BE (adjusted HR: 1.15; 95% CI: 1.06 to 1.25; adjusted p=0.001) were the only variables independently associated with overtransfusion at 24 hours after conclusion of the MTP phase of resuscitation. Given our finding that patients with penetrating injury were significantly more likely to require emergent operative intervention, we ran an additional Cox regression model and forced the variable ‘ED disposition to the OR’ into the model. We found again that the same two variables (ie, penetrating injury and BE) remained predictors of overtransfusion, and ED disposition to the OR was not.
Discussion
In this case series of trauma patients requiring activation of MTP and surviving beyond 24 hours, we found that over 7 out of 10 patients were overtransfused by the conclusion of the MTP phase of resuscitation. This proportion of overtransfused patients remained substantial at 24 hours after the conclusion of the MTP and at discharge, with over 4 out of 10 and almost 3 out of 10 patients having an Hg of 11 g/dL or higher at these respective phases of hospitalization. Overtransfusion did not correlate with the number of pRBC units transfused during the MTP phase nor with the duration of MTP. Overtransfused patients were significantly more likely to have a penetrating injury and a lower overall injury severity, however, they achieved similar endpoints of resuscitation with their non-overtransfused counterparts based on laboratory values and received a similar amount of blood products, during similar MTP duration. Penetrating mechanism and admission BE were independently predictive of overtransfusion. These findings highlight the high incidence of overtransfusion in patients requiring MTP activation and identify possible modifiable risk factors that may be considered to avoid this undesirable outcome.
Best transfusion practices have been proposed by the AABB and indicate avoiding an Hg level above 7 g/dL to 8 g/dL, depending on the patient population examined.15 This is a result of high-level evidence suggesting that targeting higher levels of Hg does not necessarily result in improved outcomes. In fact, it may result in a higher risk of infections and other adverse events. This guidance, however, is relevant only to critically ill patients who have overcome the initial period of resuscitation,16 or to patients undergoing elective or urgent surgical procedures, mostly orthopedic17 and cardiac.18 Similar guidance based on Hg cannot be applied to actively bleeding trauma patients. Hg levels in these patients may be inaccurate. Even serial Hg levels obtained within minutes in the trauma bay cannot predict the need for surgical intervention to control bleeding.19 20 Therefore, trauma surgeons rely on different parameters in their decision, not only to initiate, but also to terminate transfusion of blood products in the acute phase. The lack, however, of reliable indicators either used solely or combined to facilitate these decisions introduces a certain degree of subjectivity, and therefore, variability in the resuscitative effort. This is reflected in the high incidence of potentially avoidable blood transfusions in trauma patients presenting to the ED. In one study, this incidence exceeded 36%.12 This, in combination with the readily available blood products in the MTP coolers, may contribute further to these unnecessary transfusions, either to reflexively respond to an episode of hemodynamic change or to address ongoing blood loss that is difficult to quantify. In our study, over 70% of patients requiring MTP activation were overtransfused, as determined by the Hg level by the end of the MTP. There is scarcity of data to compare this incidence with. However, in addition to the above-mentioned factors, one could consider the availability and immediate access to a high number of units delivered with each MTP cooler at our institution (ie, 12 pRBCs, 12 plasma, 1 pheresis platelets, and 1 cryoprecipitate.) As we have no comparison group of patients who received coolers with a lower number of blood products, it is impossible to ascertain the validity of this statement. Due to a recent critical blood shortage, however, we had to implement changes to our MTP and are now including only 6 units of pRBCs, 6 units of plasma, and 1 unit of pheresis platelets. We will plan on evaluating overtransfusion with the decreased number of units in MTP with historical controls to determine the appropriate number of units that will ensure similar outcomes with the lowest risk of overtransfusion.
We found that penetrating trauma was independently associated with overtransfusion. In our attempt to explain this, we compared the disposition of patients from the ED to the OR and we found that those who suffered a penetrating mechanism were significantly more likely to be taken emergently to the OR, as compared with blunt trauma patients. Although ED disposition to the OR was not a factor independently associated with overtransfusion, this may have been a result of relatively small numbers. Penetrating trauma patients are significantly more likely to suffer a vascular injury and therefore, to require more blood products. In addition, the resuscitation of these patients in the OR is typically transferred to the anesthesiologists, who may overestimate the blood loss, either due to miscommunication between surgeon and anesthesiologist, or simply due to inability to adequately and precisely quantify the blood loss that had occurred prior to admission to the OR or during the surgery. Nonetheless, this finding should be taken into consideration when resuscitating penetrating trauma patients to minimize the incidence of unnecessary transfusion of blood products.
Our definition of overtransfusion may appear arbitrary, as it is based on an Hg value, and does not take into account any other clinical manifestations or parameters. Our goal was to depict the incidence of overtransfusion and characterize it as a clinical event of overutilization of resources, rather than associate it with outcomes. In fact, associating overtransfusion with outcomes may be problematic. In our cohort, for example, 14 out of 19 deaths (73.6%) were attributed to a severe traumatic brain injury and not to volume overload or transfusion-related complication. Zielinski et al examined overtransfusion in a mixed population of trauma and non-trauma patients and found that an Hg value over 12 g/dL was associated with a significantly higher mortality.10 Their study, however, included only patients who received 10 or more units of blood in the first 24 hours, and the majority of them were non-trauma patients. In addition, in their trauma subcohort, over 40% of deaths were directly related to a traumatic brain injury, rather than overtransfusion. Due to these differences, we elected not to define overtransfusion as an Hg value of 12 g/dL. Rather, we defined it based on what made most clinical sense as it was not our intention to examine overtransfusion as a predictor for mortality. In addition, we found no statistically significant difference in mortality between overtransfused and non-overtransfused patients, whether we used 11, or 10, or 12 g/dL as a cut-off (online supplemental appendix 2).
This study raises a host of questions, related not only to the clinical impact of overtransfusion, but also to the underlying causes, the associated costs, and the impact on the availability of this limited resource. As desirable as it is to have immediate access to blood products to use for the resuscitation of exanguinating trauma patients, at the same time, equally desirable is to avoid harming patients and wasting resources. The processes surrounding availability and utilization of MTPs have matured enough during the last two decades, and continuing to explore ways to improve their implementation and efficacy is a natural progression, especially given their substantial impact on improving outcomes. Given the high incidence of overtransfusion in our study population, tracking this outcome to allow for further exploration of its impact and identification of factors associated with it may be prudent. Overtransfusion may in fact be examined as a potential quality metric for the resuscitation of trauma patients requiring MTP activation.
This study is limited by its retrospective nature and the inherent bias associated with it. More specifically, it was not possible to correlate the timing of transfused blood products with the physiologic status of the patient nor with the timing of hemostasis achieved either by surgical or by other means. We relied exclusively on laboratory parameters and the use of vasopressors as a reflection of the resuscitation status. Interventions to address acidosis, coagulopathy, and other common problems encountered during the resuscitation of massively transfused patients were not taken into account. The definition of overtransfusion we used was based on an Hg cut-off, which may or may not reflect clinically meaningful overtransfusion, especially for patients with ongoing requirement for blood products. We did not examine the possible negative impact of overtransfusion, such as immunosuppression and increased risk of infection, volume overload, transfusion-associated lung injury, etc. By excluding patients who died within 24 hours, we may have also missed deaths related to massive overload from overtransfusion. Selection bias may have resulted from the fact that MTP activation is based on the trauma surgeon’s discretion. Resuscitation practices among trauma surgeons may differ, as they may differ between anesthesiologists who primarily take on that role in the OR and IR suites. The duration of MTP activation may not necessarily reflect the amount of time that these patients were receiving blood products, as the MTP coolers may have remained at the bedside for an undetermined amount of time without being actively used. Despite these limitations, however, this study brings to light an under-reported consequence of MTPs resulting from readily available blood products in combination with the lack of reliable endpoints of resuscitation in trauma patients and raise the need for further research to identify opportunities for improvement and for limiting overutilization of blood products.
In conclusion, overtransfusion of trauma patients requiring MTP activation is highly common, leading to overutilization of a limited resource. Penetrating trauma and BE may be modifiable risk factors that can help limit overtransfusion. Overtransfusion should be tracked as a data point by blood banks and trauma centers and be further studied as a potential quality metric for the resuscitation of massively transfused trauma patients.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This was a retrospective study that was approved by the Cedars-Sinai Medical Center Review Board (ID# Pro00056699), and for which informed consent was waived.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at This work was presented as a poster at the 79th Annual Meeting of the American Association for the Surgery of Trauma and the Clinical Congress of Acute Care Surgery in Waikoloa, Hawaii, USA in September 2020.
Contributors Study design—GB and RH. Data collection—RH and WGL. Data analysis—GB and RH. Data interpretation—YMH, SHP, GB, EBK and DRM. Article writing—GB and RH. Critical revisions—YMH, SHP, DRM and EBK. Guarantor—GB.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.