Article Text

Abstract
Background Traumatic tension pneumothoraces (TPT) are among the most serious causes of death in traumatic injuries, requiring immediate treatment with a needle thoracostomy (NT). Improperly placed NT insertion into the pleural cavity may fail to treat a life-threatening TPT. This study aimed to assess the accuracy of prehospital NT placements by paramedics in adult trauma patients.
Methods A retrospective chart review was performed on 84 consecutive trauma patients who had received NT by prehospital personnel. The primary outcome was the accuracy of NT placement by prehospital personnel. Comparisons of various variables were conducted between those who survived and those who died, and proper versus improper needle insertion separately.
Results Proper NT placement into the pleural cavity was noted in 27.4% of adult trauma patients. In addition, more than 19% of the procedures performed by the prehospital providers appeared to have not been medically indicated.
Discussion Long-term strategies may be needed to improve the capabilities and performance of prehospital providers’ capabilities in this delicate life-saving procedure.
Level of evidence IV.
- computed tomography
- thoracotomy
- pneumothorax
Data availability statement
Data are available upon reasonable request. Data are available as deidentified data upon request. Please contact the corresponding author at michaelneeki@gmail.com.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Thoracic trauma accounts for 35% of trauma-related mortality in the USA, with the most common being blunt chest trauma from motor vehicle collisions.1 Among the most serious injuries found in thoracic trauma are pneumothorax and hemothorax. In a recent study, 10.5% of adults with blunt trauma were discovered to have a pneumothorax.2 In penetrating trauma, the incidence of pneumothorax may be as high as 40%.3 While rare, a tension pneumothorax (TPT) can cause traumatic cardiac arrest. The actual incidence of TPT is difficult to ascertain, as it relies on clinical suspicion. Sharma and Jindal3 noted the postmortem discovery of undiagnosed TPT to be 3.8%. Additionally, in ventilated patients, simple pneumothorax can develop into TPT unless timely diagnosed and treated. TPT in ventilated patients can have serious complications, with mortality reaching 91%.4
Suspected TPT in the prehospital setting requires immediate treatment by prehospital medical personnel with emergent chest decompression. The American College of Surgeons’ (ACS) most recent recommendations include performing a needle thoracostomy (NT) by paramedics to decompress a suspected TPT until a tube thoracostomy (TT) is performed.5 The procedure is within the accepted scope of practice for paramedics.6 Although there is no standardized national protocol, the majority of emergency medical service (EMS) agencies have protocols on the management of suspected TPT.7
Field experience with prehospital NT had revealed mixed results. Although the number of prehospital NTs performed tends to vary by practice environment, studies have shown that the incidence ranges from 0.2% to 1.7%.8 9 Furthermore, the rate of complications after prehospital NT placement requiring intervention has been low.10 Eckstein and Suyehara8 reported less than 2% of prehospital NTs had a complication requiring intervention, with the most common complication being iatrogenic pneumothorax. However, the procedure’s effectiveness has been questioned, with high failure rates being reported. Axtman and colleagues11 noted that prehospital NTs were successfully placed in only 5.7% of attempts. Similar rates were found when clinical criteria were used, with only 5% showing objective improvement in field vital signs and 7% having subjective improvement of their dyspnea.8
Improperly placed NT insertion into the pleural cavity may fail to treat a life-threatening TPT. Prior studies suggested that ineffective treatment of an existing TPT may be caused by insufficient angiocatheter length, inaccurate angiocatheter placement, or a blockage of the angiocatheter such as from blood clots or kinks.12 This study aims to review the accuracy of prehospital NT placements by paramedics in adult trauma patients, which is verified through a CT scan during the initial trauma evaluation at a regional trauma center.
Patients and methods
This is a retrospective chart review with prospective observational study. Informed consent was waived and data were reported in an aggregated format. No patients’ data were identified in this article. The Arrowhead Regional Medical Center (ARMC) is a 456-bed acute care teaching facility and the only ACS-verified level II trauma center located in San Bernardino County (SBC), California. The ARMC emergency department (ED) is one of the busiest in the state of California with more than 100 000 visits and over 3000 adult trauma cases annually.13
This study analyzed consecutive patients from January 1, 2018 to September 30, 2020 who were identified by paramedics as having a life-threatening TPT and underwent NT placement in the prehospital setting. The indications for NT placement as defined by the Inland Counties Emergency Medical Agency included any of the following clinical findings: progressively worsening dyspnea/cyanosis, decreased or diminished breath sounds on the affected side, hypotension, increased agitation, distended neck veins, or tracheal deviations away from the affected side.14 Patients who survived the initial phase of the trauma evaluation in the ED were included in the study. These patients received subsequent CT scans as part of trauma care. As per the study protocol, the prehospital angiocatheters were kept in the original position until patients completed their CT scans, with the aim of assessing the accuracy of NT placement by prehospital personnel. Two groups were analyzed in this study: (1) proper NT insertion into the pleural cavity confirmed by CT and (2) improper NT insertion as noted by CT to be outside the pleural cavity. In cases where the angiocatheters were dislodged, the path can be identified by careful review of both coronal and sagittal images of each CT scan. Chest wall thickness (CWT) was measured for each patient at the second intercostal space of the midclavicular line (ICS-MCL), the fourth intercostal space of the anterior axillary line (ICS-AAL), and the fourth intercostal space of the midaxillary line (ICS-MAL). The measurements were obtained on CT scans by two independent reviewers. Additional data points included age, gender, Injury Severity Score (ISS), mechanism of injury, days in an intensive care unit (ICU), discharge status, chest tube placement, transport method, and body mass index (BMI).
All statistical analyses were conducted using the SAS software for Windows 9.4 (Cary, NC, USA). Descriptive statistics were presented as mean and standard deviations (SD) for continuous variables, along with frequencies and proportions for categorical variables. χ2 tests were conducted to assess the association between categorical variables and survival status and NT insertion status (proper vs. improper) separately. Independent t-tests were conducted to assess whether the continuous variables were different between the survival status and NT insertion status (proper vs. improper) separately. All statistics were two-sided. A p value <0.05 was considered statistically significant.
Results
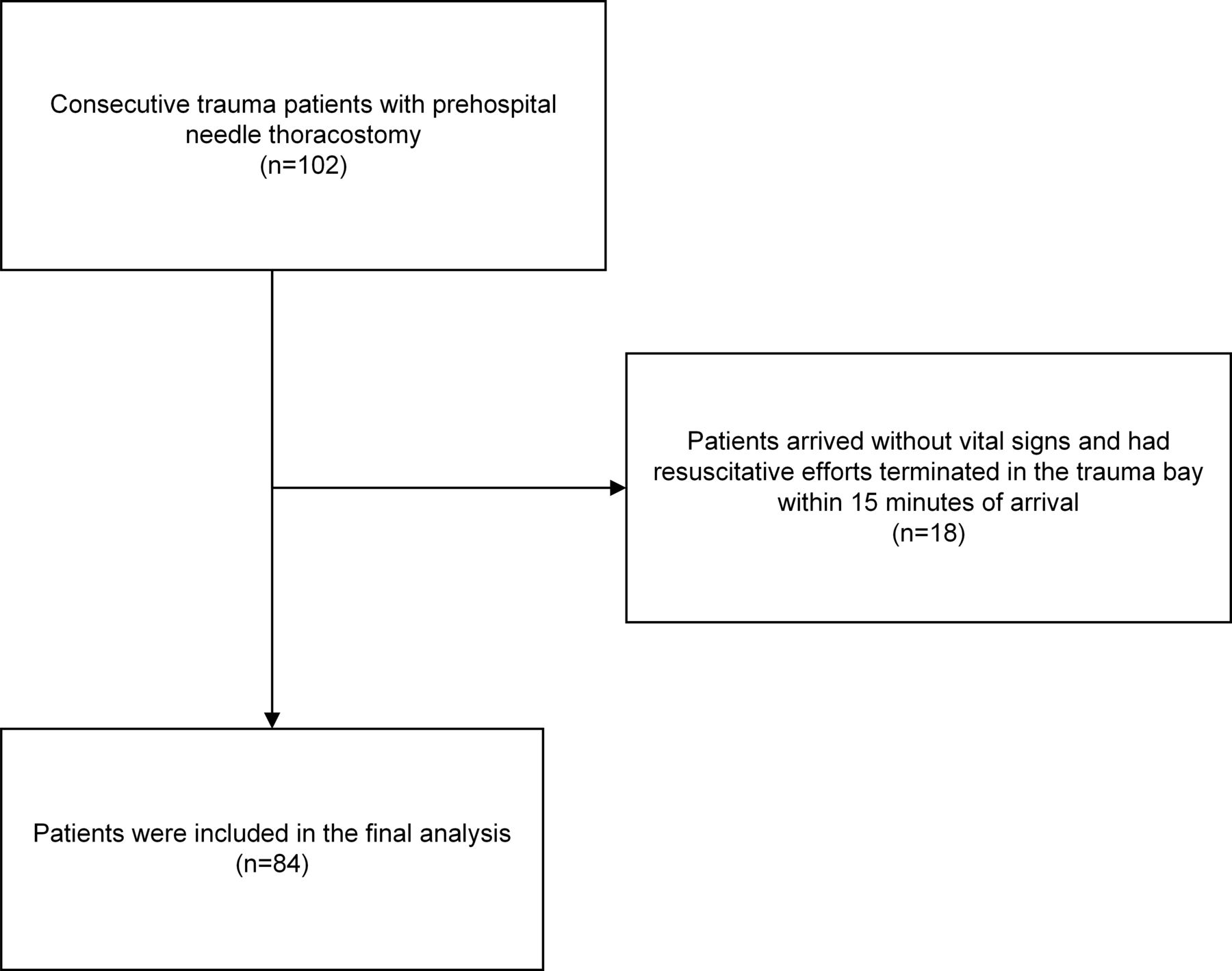
Among the original 102 patients included in the analysis, 18 were excluded as they presented to the hospital with no vital signs and were declared dead on arrival. As a result, a total of 84 patients were included in the final analysis. Figure 1 presents the patients’ flow chart.

Patients’ flow chart.
Among the final 84 patients, majority were male (n=78, 92.9%), sustained blunt trauma (n=58, 69.1%), had a TT (n=68, 81%), and arrived through ground transport (n=48, 57.1%). The average age was 38.6 (SD=16.04) years, the average BMI was 29.1 (SD=5.36) kg/m2, and the average ISS was 28.69 (SD=10.69). Proper NT insertion into the pleural cavity was identified in 27.4% (n=23) of the patients. Only 81.0% (n=64) of the patients required a subsequent TT. Five patients sustained iatrogenic injuries from the attempted NT. One patient had splenic insertion; two had hepatic insertion; two had subdiaphragmatic insertion; and one had anterior mediastinum placement. The median hospital length of stay was 7 days, and the median ICU stay was 5 days. The overall mortality rate was 15.5% (n=13). Table 1 presents the detailed summary of these 84 patients.
Patients’ demographic summary
Comparisons of variables between the survival status were conducted and the results of the analysis are presented in Table 2. Overall, patients who did not survive hospital discharge were older (average age 52 vs. 36.14, p=0.0008). There was no statistically significant difference in other variables between survival status (all p>0.05).
Comparison of variables between survival status
Comparisons of variables between NT procedures (proper vs. improper insertion) were conducted and the results of the analysis are presented in table 3. Overall, air transport was associated with a higher likelihood of proper insertion than ground transportation (p=0.0405). There was no statistically significant difference in other variables between insertion status (all p>0.05). As expected, patients with thicker chest wall had a higher likelihood of a failed NT. Among the 61 patients with failed NT, more than 20% had CWT ≥70 mm at the second ICS-MCL (13 of 61, 21.3%; results not shown in table 3), fourth ICS-MAL (16 of 61, 26.2%; results not shown in table 3), and fourth ICS-AAL (14 of 61, 30.0%; results not shown in table 3).
Comparison of variables for CT findings
There are 18 patients who arrived at the hospital without vital signs and had resuscitative efforts terminated in the trauma bay within 15 minutes of arrival without undergoing any imaging studies. The average age in this group was 33.4 (SD=14.2) years; the average BMI was 29.1 (SD=3.85) kg/m2; and the average ISS was 36.8 (SD=5.93). Majority of these patients were male (n=16, 88.9%), arrived via ground transport (n=16, 88.9%), sustained blunt trauma (n=12, 66.7%), and had a TT performed on hospital arrival (n=12, 66.7%). The actual cause of death attributable to improper NT insertion is difficult to quantify in these cases.
Discussion
A TPT is a potential cause of traumatic cardiac arrest, requiring immediate recognition and treatment by prehospital medical personnel with needle decompression. To be effective, the provider must successfully place the angiocatheter into the pleural cavity without injuring any surrounding neurovascular structures. The main factors that contribute to failure include improper anatomic location for insertion, improper angiocatheter length for the desired location, and CWT that exceeds the available catheter length.12 15
There has been debate about the specific site and length of the angiocatheter for NT. The three locations recommended are the second ICS-MCL, the fourth/fifth ICS-AAL, and the fourth/fifth ICS-MAL. In a systematic review and meta-analysis, Laan et al16 examined the CWT of these three recommended sites. They noted that the chest wall was thinnest at the fourth/fifth ICS-AAL (34.33 mm) compared with the second ICS-MCL (42.79 mm) and the fourth/fifth ICS-MAL (39.85 mm). Correspondingly, they noted the failure rate was also lowest at the fourth/fifth ICS-AAL (13%) compared with the other two sites (38% and 31%, respectively). As a result, they concluded that the fourth/fifth ICS-AAL may be a better option in patients with a suspected thicker chest wall or in patients in which a prior NT attempt had failed.16 Furthermore, Leatherman and colleagues17 noted that the fifth ICS-AAL was most stable for combat casualty transport. However, this was a cadaveric study involving a select BMI of 24 kg/m2, which does not represent our patient population.17
In addition to identifying the proper location, an appropriate needle length is also crucial for a successful catheter placement. Givens and colleagues18 challenged the previous recommendations of a 5 cm angiocatheter. Using CT measurements, they noted that a 5 cm catheter at the second ICS-MCL would fail in 25% of cases due to insufficient length. They therefore recommended that longer catheters should be considered, especially in women.18 Their findings were consistent with other researchers who reported failure rates of using a 5 cm angiocatheter to be as high as 94% and recommended using an 8 cm angiocatheter for NT.11 19 ATLS recently updated their recommendations to include placement of a 5 cm to 8 cm angiocatheter in the fourth/fifth ICS-MAL.5 The Tactical Combat Casualty Care guidelines also recommended placement of a 3.25 inch (8.25 cm) angiocatheter in either the fifth ICS-MAL or the second ICS-MCL.20 All EMS agencies within the ARMC serving region involved in this study use the 14 gauge or 16 gauge, 3.25 inch (8.25 cm) needle.
Based on the presented evidence, our study supports the recommendation of using the longer angiocatheter for NT for suspected TPT in all patient care settings. The second ICS-MCL was the preferred site for NT by prehospital personnel in 81 of 84 (96%) patients. At this site, 63% of patients had CWT >50 mm (see figure 2), which would render the shorter 5 cm angiocatheter ineffective. About 20% of patients had CWT ≥70 mm, which leaves little room for error even with the longer 8.25 cm catheter. Only 23 (27.4%) patients had the NT properly inserted into the pleural cavity based on CT findings. Although there was no statistically significant difference in mortality (91.3% vs. 82.0%, p=0.4994) between proper and improper insertion, the proper insertion group was associated with higher likelihood of survival to discharge, reinforcing the importance of appropriate application of NT in managing suspected traumatic TPT.
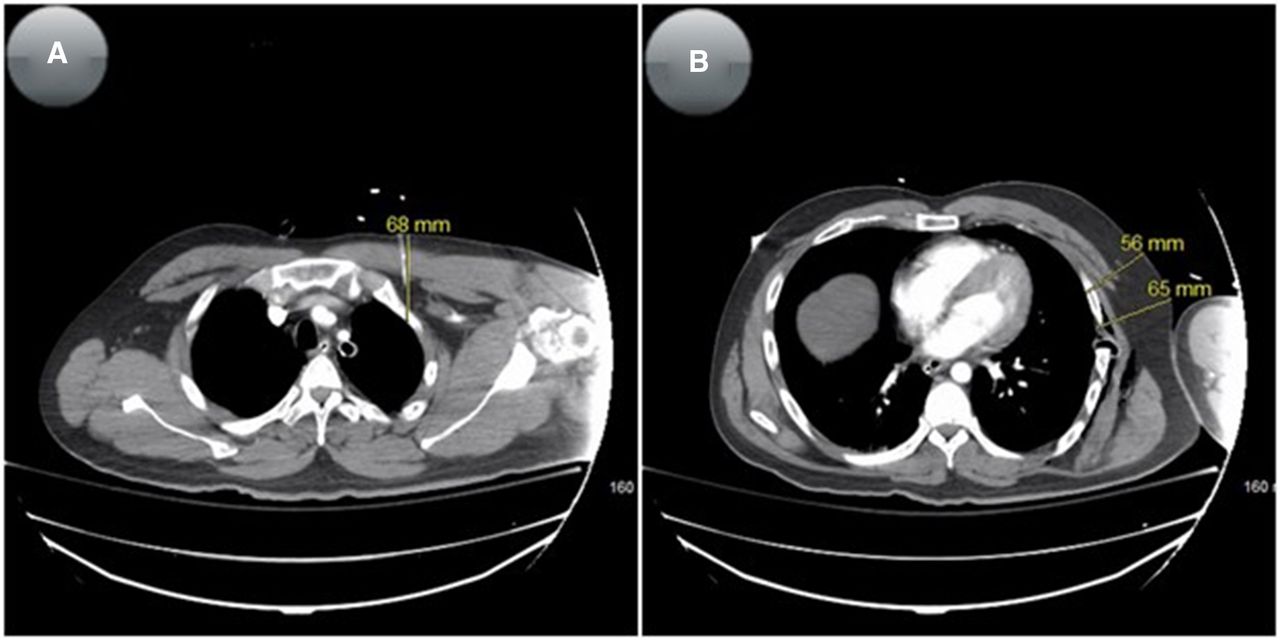
Examples of chest wall thickness measurements in the second intercostal space of the midclavicular line (A), fourth intercostal space of the anterior axillary line (B), and fourth intercostal space of the midaxillary line (B).
Similar to prior studies, factors contributing to failed NT placement are multiple and some of these cases are demonstrated in figure 3. These findings suggest that enhanced training of prehospital personnel using techniques such as simulation or cadaver laboratories should be considered to improve outcome. Grabo et al21 noted that paramedics had a higher success rate of performing NT when trained with a cadaver (75%) as compared with traditional slides and lectures (35%). Additionally, the recent advancement in simulation models and techniques has drastically improved training in medically invasive techniques.22 Continuous and constructive performance feedback is needed from the agencies’ medical directors, regional trauma services, and when indicated from coroners.

Examples of improper needle thoracostomy placements with the needle angled downward (A), upward (B), and too lateral (C).
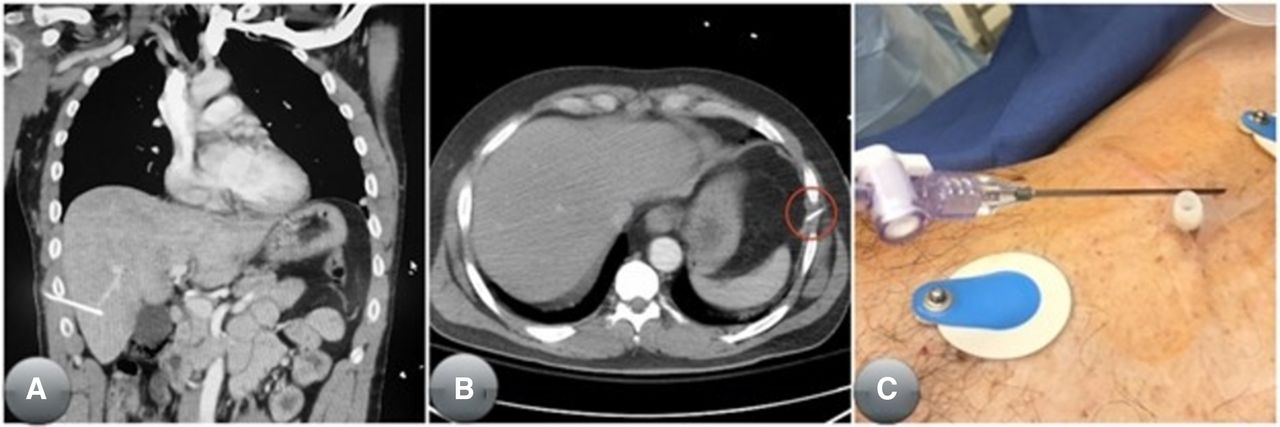
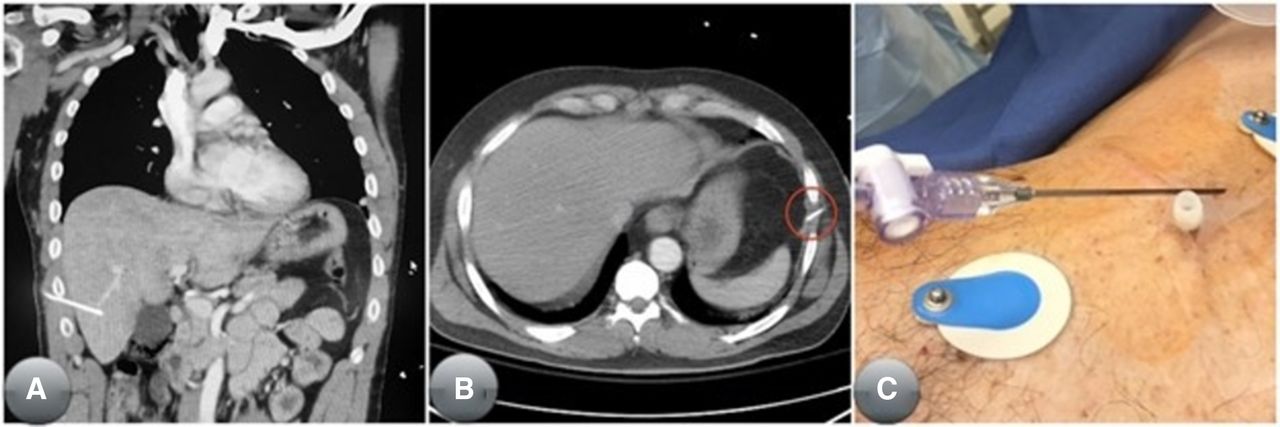
The appropriateness of NT placement is more difficult to assess especially in a dynamically changing situation such as trauma in the prehospital setting. For the current study, 16 (22.5%) patients did not receive a TT during the trauma resuscitation, indicating that no pneumothorax or hemothorax was discovered on CT. The CT findings suggest that these 16 patients did not need NT in the prehospital setting. The actual rate may be potentially higher as it is impossible to determine if the pneumothorax discovered on CT was iatrogenically caused once NT has been performed. Even when appropriately indicated, there are potential serious complications with NT, including life-threatening hemorrhages.23 Additionally, the subsequent TT for any iatrogenic pneumothorax places the patient in unnecessary risk of complications, including hepatic, splenic, diaphragmatic, lung, and cardiac injuries.23 This study also observed few cases of iatrogenic injuries from inappropriate placement of NT in the abdominal cavity, spleen, and liver. These are demonstrated in figure 4. Therefore, strategies to minimize medically unnecessary NTs should be explored by EMS regulatory agencies throughout the USA.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Examples of complications from improper needle thoracostomy placements: hepatic penetration (A), subdiaphragmatic placement with potential splenic penetration (B), and advancement of both needle and catheter into the thoracic cavity (C).
The Eastern Association for the Surgery of Trauma (EAST) trial led by Taghavi et al24 recently asserted that prehospital procedures (PHPs) in penetrating trauma patients impart no survival advantage and may be detrimental in urban settings. However, they did not address similar concerns for blunt trauma. Additionally, they admitted that there was an inherent bias as patients receiving PHPs were more severely injured. Furthermore, the EAST article did not specifically examine the time for transport, undoubtedly assuming the time would be minimal in an urban setting. These findings should encourage more thorough research to provide evidence-based recommendations with regard to penetrating trauma in urban settings with short transport time. The geographical location of ARMC is unique as it serves as a major trauma center in SBC, which is the largest geographical county in the USA. Transport time to ARMC may be significantly longer than the average US urban trauma center, and at times requiring air transport. In our study population, 42.9% of these patients arrived by air transport, indicating a longer transport time. Although the EAST trial has a different study composition from our study of nearly 70% blunt trauma, we agree with their suggestion that most prehospital NTs may not be indicated in the urban setting with a short transport time.
There is a new school of thought recommending treatment of suspected TPT in prehospital traumatic cardiac arrests with simple thoracostomy (ST) instead of NT.25 ST is a technique similar to TT but involves the release of the TPT using forceps and a gloved finger without placing the chest tube. This protocol was first implemented in the European prehospital arena with promising results. However, small studies in Italy and the UK both involved ST performed only by highly trained air medical personnel.26 27 Dickson and colleagues28 suggested that ST can be performed by specially trained paramedics in ground-based EMS agencies in the USA with good results. Our study suggests that serious considerations should be given to using ST to treat suspected TPT. Based on CWT, about one-fifth of patients would fail NT at all three recommended sites of insertion, even when using the longer 8.25 cm catheter. Additionally, using ST would also decrease the complications associated with improper needle placements. This will represent a major shift in policies regarding the scope of practice for paramedics in the USA and will require a robust educational program with strong oversight.
The diagnosis of a TPT is made solely on clinical suspicion and findings, which may include decreased breath sounds and hypotension. Unfortunately, other traumatic pathologies also present with similar clinical findings, such as hemorrhagic shock with concomitant rib fractures. Point-of-care ultrasound has been shown to have high sensitivity and specificity in diagnosing a pneumothorax when performed by emergency physicians.29 The emergence of smaller portable ultrasound machines may be an opportunity to improve quality of care in the prehospital setting.30 31 Future large-scale research should investigate if prehospital personnel can be appropriately trained to use this modality to improve their recognition of a TPT and decrease the rate of inappropriate NT placement.
The generalizability of findings in the current study may be limited by several factors. First, our sample of 84 patients were from one single level II trauma center, which represents only one geographical location. This might limit the generalization to other geographical locations. A multicenter study with a more inclusive patient population is warranted to confirm our findings. Furthermore, the total number of prehospital NTs cannot be determined as patients who do not achieve return of spontaneous circulation would not be transported to trauma centers. An open channel of communication among the trauma centers, regional EMS agencies, and the local corners would be ideal to assess the true incidence of inappropriate NT placement.
Additionally, this study does not address the difference between transport to trauma centers from police versus ground EMS agencies. Recent studies have noted that patients who sustained penetrating trauma and were transported to trauma centers by law enforcement (LE) had no difference in adjusted in-hospital mortality when compared with penetrating trauma transported by EMS agencies.32 33 For our study population, among the 26 patients who sustained penetrating trauma, 16 were transported by ground with a mortality rate of 25% (n=4), and 10 arrived by air with a mortality rate of 10% (n=1). The recently adopted policy of “scoop and run” by LE in Philadelphia may not translate well to a larger geographical area such as SBC. Tansley and colleagues34 have noted that longer travel time was associated with worse outcomes for victims of penetrating and blunt traumas. Based on the evidence presented in the prior studies, we recommend that the policy of “scoop and run” by either LE or EMS should be selective and encouraged for patients who have sustained penetrating trauma within a reasonable transport time to trauma centers.32–35
Conclusion
The effective placement of an NT is an appropriate intervention for life-threatening TPT. Our results suggest a less than optimal rate of success in proper placement of NT by EMS personnel. The utilization of NT should be limited without a robust program including longitudinal education program and strict supervision to improve the quality of care in the prehospital trauma care.
Data availability statement
Data are available upon reasonable request. Data are available as deidentified data upon request. Please contact the corresponding author at michaelneeki@gmail.com.
Ethics statements
Ethics approval
This study was approved by the Institutional Review Board (IRB approval number 19-28) at Arrowhead Regional Medical Center.
Acknowledgments
We would like to thank Arrowhead Regional Medical Center administrators and trauma committee members for their support to conduct this study. In addition, we would like to extend our heartfelt gratitude to our trauma team members for their relentless support during the study period.
References
Footnotes
Contributors MMN, CC, FD, and NP designed the study, gathered the data, and wrote and revised the article. DS, AN, KH and RB conducted the data analyses and wrote the article. BW and LT wrote and revised the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.