Article Text

Abstract
Background Unplanned intensive care unit (ICU) readmission—ICU bounce back (ICUbb)—is associated with worse outcomes. Patients not requiring organ system support or intensive nursing are deemed ‘ICU discharge ready’ and transfer orders are placed. However, actual transfer only occurs when an appropriate, non-ICU bed is available. This is dependent on inherent system inefficiencies resulting in a naturally controlled experiment between when patients actually transfer: Early (<24 hours) or Delayed (>24 hours) transfers, after order placement. This study leverages that natural experiment to determine if additional ICU time is protective against ICUbb. We hypothesize that Delayed transfer is protective against ICUbb.
Methods Using a retrospective, cohort design, we queried a trauma research repository and electronic medical record during a 10-year period to capture traumatized patients admitted to the ICU. Patients were categorized into Early (<24 hours) or Unintended-Delayed (>24 hours) groups based on actual transfer time after order placement. Patient characteristics (age, Charlson Comorbidity Index (CCI)) and Injury Severity Score (ISS) were analyzed. Univariate and multivariate analyses were performed to compare ICUbb rates among Early and Unintended-Delayed groups.
Results Of the 2004 patients who met the criteria, 1690 fell into the Early group, and 314 fell into the Delayed. The Early group was younger (mean age 52±23 vs. 55±22 years), had fewer comorbidities (median CCI score 1 (0, 3) vs. 2 (1, 3)), and was less injured (median ISS 17 (10–22) vs. 17 (13–25)), all p<0.05. Overall, 113 (5.6%) patients experienced ICUbb: Early 109 (6.5%) versus Unintended-Delay 4 (1.3%), p<0.05. By regression analysis, age, CCI, and ISS were independently associated with ICUbb while Delayed transfer was protective.
Discussion Despite higher age, CCI score, and ISS, the Unintended-Delayed group experienced fewer ICUbb. After controlling for age, CCI and ISS, Delayed transfer reduced ICUbb risk by 78%. Specific care elements affording this protection remain to be elucidated.
Level of evidence Level III.
Study type Therapeutic study.
- multiple trauma
- intensive care units
- patient readmission
- quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Unplanned intensive care unit (ICU) readmission after ICU discharge—that is, ICU bounce back (ICUbb)—is associated with worse outcomes, including higher mortality.1–5 It is not the ICUbb per se that is responsible for worse outcomes, rather ICUbb serves as a marker of clinical deterioration post-ICU discharge, and it is this clinical deterioration necessitating ICUbb that is responsible for the worse outcomes. This leads to the question of whether aggressive care provided in the immediate post-ICU discharge period could reduce rates of clinical deterioration, thus ICUbb, and ultimately improve clinical outcomes.
Research addressing this question is limited. Most studies focus on the role of a ‘step-down’ or ‘intermediate care’ unit for patients immediately post-ICU discharge prior to transition to ‘floor’ status.6–19 These studies demonstrate mixed results, varying from modest improvement of,7–10 no improvement in,11–14 19 and even worsening of outcomes,15 and many show increased cost.6 16 17 The majority of these studies, however, were performed on medical patients or mixed medical/surgical population with low incidence of trauma patients.7–10 12 14–16 19 Of the larger studies that included surgical ICU patients, some focused on perioperative ICU care for elective surgical patients,18 and others excluded ICUs caring for trauma patients.19 There have been two studies that have focused on unplanned ICU admissions among trauma patients. Rubano et al4 included all patients with unplanned ICU admissions whereas Fakhry et al5 focused exclusively on ICU readmissions or bounce backs (bb). Both those studies demonstrated that total burden of injury and specific injury patterns play a significant role in unplanned ICU admissions, including bb. No large-scale study, to our knowledge, has focused on evaluating the impact of post-ICU discharge care on ICUbb rates and clinical outcomes among trauma patients. The current study, using an innovative design that leverages the inefficiency of the ICU discharge process, aims at answering whether aggressive care in the immediate post-ICU discharge period can reduce the rates of ICUbb and improve clinical outcomes.
Patients not requiring organ system support or intensive nursing are deemed ‘ICU discharge ready’ and transfer orders are placed. However, actual ICU discharge or transfer occurs only when an appropriate, non-ICU, staffed bed is available. This results in a naturally controlled experiment between Early (discharged <24 hours) and Delayed (discharged >24 hours) patients after ICU discharge order placement. To evaluate the impact of care immediately after ICU discharge, we compared the ICUbb rates of the Early and Delayed groups. We hypothesize that ICUbb rates will be lower in the Delayed group.
Methods
This is a single-center, retrospective, cohort study performed at the University of Vermont. The University of Vermont Medical Center is an academic, rural, American College of Surgeons-verified Level I Trauma Center serving a population of approximately 1 million in the surrounding rural and suburban areas encompassing most of Vermont and northeastern New York. Trauma patients requiring ICU-level care are admitted to an open surgical ICU and, once deemed ready for ICU discharge, are transferred to the floor. The decision for admission to and discharge from the ICU is made by the attending surgeon. While protocols aid in decision-making, the patient’s disposition is chosen by the attending surgeon based on clinical assessment of the patient. There is no intermediate care or step-down unit.
All injured patients presenting to the emergency department (ED) and admitted to the hospital during the 10-year study period ending March 2018 were identified from the Trauma Research Repository (Digital Innovation, V5-Forest Hill, Maryland). Clinical data of these patients were obtained from the repository and Jeffords Institute for Quality Database (Epic Electronic Health Records, Epic Systems, Verona, Wisconsin). Clinical data obtained included patient demographics (age, gender), comorbidities and calculated Charlson Comorbidity Index (CCI),20–22 injury characteristics (Abbreviated Injury Scale (AIS) for each body region and calculated overall Injury Severity Score (ISS)), and outcomes (ICU and hospital lengths of stay, mortality). Patients triaged from the ED to non-ICU locations, those initially admitted to the ICU and died without ever being transferred out, and those with missing data, including timestamps for ICU discharge orders and/or actual ICU discharge, were excluded. The time the first order for ICU discharge was placed was obtained and compared with the time the actual ICU discharge (transfer) occurred. This allowed for the categorization of patients as (1) Early transfer—patients with actual ICU discharge occurring <24 hours after placement of discharge orders, and (2) Delayed transfer—patients with actual ICU discharge occurring >24 hours after order placement. Patient and injury characteristics and the rates of ICUbb were compared between the groups. For patients experiencing ICUbb, details of the bb including reason and timing were recorded. Patients experiencing multiple bb were included only once. All data were stored in Microsoft Excel (Redmond, Washington), and analyses were performed using Stata V.15 (StataCorp, College Station, Texas).
Statistical analyses were performed using a combination of methods with statistical significance defined as p<0.05. Differences in age were determined using unpaired t-tests and proportional distribution differences were tested with χ2. The remainder of univariate analyses were performed using non-parametric tests, such as Wilcoxon rank-sum test. A multivariate logistic regression model was constructed to identify factors independently associated with ICUbb and mortality. Age-based subgroup analysis was performed to evaluate which age groups, if any, benefited the most from additional care. Finally, the number needed to treat for any benefit of care was calculated.
Results
During the 10-year period, 11 417 patients were identified. Of those, 9413 were excluded (non-ICU admission: 7303; incomplete records or death in the ICU on initial admission: 850; and missing timestamps: 1260) and the remaining 2004 patients who were admitted from the ED to the ICU and discharged alive from the ICU at least once formed the study population.
Patient and injury characteristics of the study population, as well as comparisons between patients who experienced ICUbb (ICUbb+) and those who did not (ICUbb–), are presented in table 1. A total of 113 (5.6%) from the overall study population of 2004 experienced ICUbb. Patients experiencing ICUbb were older, carried a higher comorbidity burden (higher CCI), and were more severely injured (higher ISS), p<0.05 for all (table 1). Additionally, ICUbb patients were more likely to have experienced significant injuries (defined as AIS score >2) to the spine and external soft tissues, p<0.05 for both (table 1). The median time to ICUbb was 2 days (IQR 1, 4). Respiratory deterioration was by far the most common reason for ICUbb accounting for 70 (62%) of all bb. The other reasons for bb were: altered mental status 18 (16%); cardiac instability 8 (7%); sepsis 5 (4%); cerebrovascular accident 4 (3.5%); alcohol withdrawal 2 (2%); hemorrhage 2 (2%); and others 4 (3.5%). Outcomes of patients experiencing ICUbb were worse in terms of longer ICU and hospital lengths of stay and increased mortality, p<0.05 for all (table 1). In the logistic regression analysis, along with age and ISS, ICUbb was an independent predictor of mortality with an OR of 6.73 and 95% CI of 3.80 to 11.91, p<0.05 (table 2).
Patient demographics, comorbidities, injury burden and patterns, and hospital outcomes of the study population (all patients) and comparisons of patient cohorts experiencing ICUbb (ICUbb+) to those that did not (ICUbb−)
OR with 95% CIs of factors that are independently associated with mortality
Of the 2004 patients that comprised the study population, 1690 (84%) fell into the Early group and 314 (16%) into the Delayed group. Patient and injury characteristics of Early and Delayed cohorts are presented in table 3. The median time of actual discharge was 3.88 hours (IQR 2.42, 6.37) for the Early group and 43.84 hours (IQR 29.05, 77.62) for the Delayed group. The Delayed group was older, with a higher comorbidity burden (higher CCI), and more severely injured (higher ISS), p<0.05 for all (table 3). Despite these ‘negative’ characteristics that are independently predictive of ICUbb (table 4), the ICUbb rate of the Delayed group at 1.3% was significantly lower than that of the Early group at 6.5%, p<0.05 (table 3), and Delay in ICU discharge was independently protective against ICUbb with an OR of 0.16 and 95% CI of 0.06 to 0.44, p<0.05 (table 4). Mortality of the Delayed group was lower than the Early group (2.2% vs. 3.9%, table 3) though this did not reach statistical significance (p>0.05). When Delay was used in the mortality regression model, Delay trended towards decreased mortality with OR of 0.48 but the 95% CI (0.214 to 1.064) crossed unity, and hence it was not statistically significant (p=0.07).
Presentation demographics, comorbidities, injury burden, and outcome data of the Early vs. Delayed cohorts
Logistic regression models evaluating the OR of ICUbb based on age, ISS, CCI score, and Delayed ICU transfer
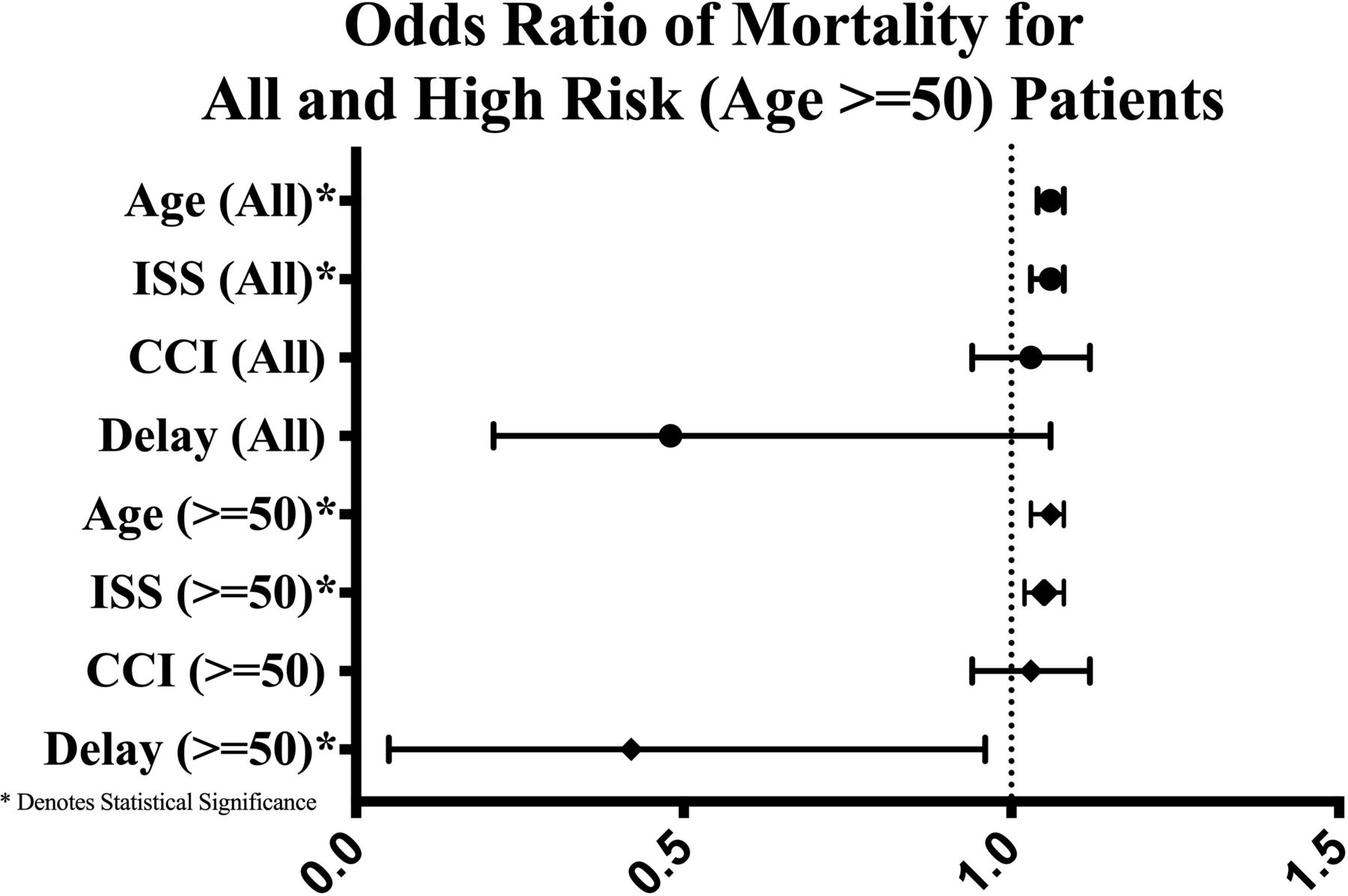
To identify the age group(s) with the highest mortality risk that may benefit the most from additional care, we evaluated age against mortality. There was an inflection point at age 50, after which mortality abruptly rises (figure 1). Based on those data, we performed a subgroup analysis for patients aged ≥50 years. We evaluated the independent risk of mortality from ICUbb, as well as the independent protective effect of Delay against ICUbb rates and mortality. In that subgroup analysis, the mortality rate of patients in the Delayed transfer group was significantly lower than in the Early group (2.9% vs. 6.6%, p<0.05). Using logistic regression, as compared with the entire study population, the impact of ICUbb on mortality was stronger in the ≥50 years subgroup (OR 7.48, 95% CI 4.14 to 13.50). Additionally, the protective effect of Delayed transfer against ICUbb was similar (OR 0.18, 95% CI 0.06 to 0.5). However, the protective effect against mortality was stronger and statistically significant (OR 0.42, 95% CI 0.18 to 0.99), p<0.05 for all (figure 2).

Mortality in trauma patients admitted to the intensive care unit grouped by age showing a significant increase with age beginning in the 6th decade of life.
{kind=link}
{kind=link}
Forest plot of the OR for mortality based on age, Charlson Comorbidity Index (CCI), Injury Severity Score (ISS), Delayed intensive care unit (ICU) discharge for all patients (circle) and for the high mortality risk subset (age ≥50, diamond). *Represents statistical significance with p<0.05.
Based on these results, the number needed to treat—additional ICU patient-days—to prevent a single ICUbb and prevent a single death is 21 and 54, respectively. For the high-risk group (age ≥50), the numbers were 15 additional ICU patient-days to prevent a single ICUbb and 30 additional ICU patient-days to prevent one death.
Discussion
ICUbb represents clinical deterioration post-ICU discharge, and outcomes of patients experiencing ICUbb are worse, including significantly higher mortality rates.1–5 This raises the question whether aggressive care provided in the immediate post-ICU discharge period could prevent clinical deterioration, thus reducing rates of ICUbb, and potentially improving outcomes. Almost all studies addressing this question have evaluated the impact of ‘step-down’ or ‘intermediate-care’ units on patient outcomes.6–19 The results of these studies have been mixed in terms of impact on clinical outcomes and costs. However, none of these studies were focused exclusively on injured patients and their unique care requirements. It is well known that injury pattern and overall injury burden have a major impact on the rates of ICUbb among trauma patients.4 5 The current study focuses exclusively on injured patients directly admitted to the ICU from the ED. It uses an innovative design that leverages the inadvertent naturally controlled experiment created by the inefficiency of the ICU discharge process to answer the question whether aggressive care provided in the immediate post-ICU discharge period can prevent clinical deterioration, thus reduce ICUbb rates and improve outcomes.
The overall rate of ICUbb in the current study was 5.6% which is consistent to what has been reported by Fakhry et al.5 Increasing age, higher comorbidity burden, and being more injured were independently associated with ICUbb. Despite the low rate, ICUbb was associated with worse clinical outcomes, including significantly higher mortality. The association is also in line with what has been previously reported.1–5 The median time to ICUbb of 2 days, and respiratory deterioration being most frequent reason for ICUbb, too is consistent with existing literature.4 5
The current study is unique in leveraging the inefficiency of the ICU discharge process to answer an important question—can aggressive care provided in the immediate post-ICU discharge period improve outcomes? The ‘Delayed’ group, while considered ICU discharge ready, stayed in the ICU for additional time waiting for an appropriate non-ICU staffed bed. During this waiting period, these patients likely received more aggressive care including higher nurse to patient ratios and other ICU care processes than they would have on the floor had they been transferred when discharge orders were placed. We think that this additional care was directly responsible for the lower rate of ICUbb seen in the Delayed group. It could be argued that the higher rate of ICUbb among the Early group was due to premature ICU discharge. While possible, since our overall rate of unplanned ICU admissions, including ICUbb, is consistent with other reports in the literature and in line with national benchmarks set by Trauma Quality Improvement Project,23 premature discharge as the cause of higher ICUbb among the Early group is likely not the case.
The mortality of the Delayed group, while lower than the Early group, did not reach statistical significance either in the univariate or the multivariate logistic regression analysis. Looking at the entire study population, we think this to be a type II error since the overall mortality was quite low. However, for the age group with the highest risk of mortality, Delay in ICU discharge, a surrogate for more aggressive care post-ICU discharge, was independently protective against both ICUbb and mortality (figure 2). This suggests that the benefit of aggressive post-ICU care is especially beneficial to this high-risk group.
The overall rate of ICUbb in the study was quite low with the result that the numbers needed to treat—additional ICU patient-days—for preventing a single ICUbb are high and for preventing a single mortality higher. Hence, keeping patients in the ICU for additional days to prevent ICUbb and reduce mortality is a very inefficient use of a limited and expensive resource and likely cost prohibitive. While the concept of an ‘intermediate care’ or ‘step-down’ unit where all, or at least patients at high risk of ICUbb and mortality, spend additional days before being transitioned to the floor, is an attractive one, studies evaluating the impact of such units have mixed results with no clear consensus that such units actually improve outcomes, though they do increase cost. We think that the optimal interpretation of these results would be to develop care pathways that can be used on the floor geared towards the patient discharged from the ICU. Two findings from the study—respiratory deterioration was the most common reason for ICUbb and spine injury was more often seen in patients experiencing ICUbb—suggest that these care pathways should be directed towards respiratory care and mobilization. We are in discussion with our respiratory and physical therapists to (A) evaluate a patient within 4 hours of ICU discharge and (B) increase the frequency of respiratory and mobility interventions on all patients discharged from the ICU especially in the critical first 48 hours post-ICU discharge.
The study has significant limitations. First, it is a single institutional study from an institution with no step-down unit, and thus the results may not be generalizable to other institutions with differing ICU/high-intensity unit structure. Second, it is a retrospective study spanning 10 years during which care processes may well have evolved and changed. Additionally, during this time period, the event rate was low making further analysis of the data by time period difficult. However, we needed this long time span to have enough patients for a robust logistic regression analysis. Lastly, the unique design of the study used additional time in the ICU as a surrogate for additional care; however, the exact care elements that may have been responsible for the lower rates of ICUbb and reduced mortality among the Delayed group cannot be determined from this retrospective study.
Conclusion
Despite the limitations cited, this study demonstrates that ICUbb among trauma patients is a low incidence event with high consequences—worse outcomes including mortality. Aggressive care immediately post-ICU discharge reduces the rates of ICUbb, likely reduces mortality in all patients, and does reduce mortality in those patients at highest risk.
References
Footnotes
Twitter @SRanney_MD
Presented at Presented at the 50th Annual Meeting of the Western Trauma Association on February 24, 2020 in Sun Valley, Idaho.
Contributors All listed authors warrant their names on the publications and have made substantial contributions. SER, LP, THL, GCA, and AM contributed to study conception and design. SER, SA, LP, THL, and AM helped with acquiring data. SER, SA, LP, THL, PC, GCA, and AM helped with analysis and interpretation of data. SER, SA, and AM drafted the article. SER, SA, PC, GCA, and AM provided critical revisions.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The University of Vermont Institutional Review Board approved this study (ID 18-0673).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. The authors do not have permission to share the data collected as it contains PHI.