Article Text

Abstract
Background Organism susceptibilities for trauma-associated pneumonia (TAP) differ from those in other patient populations, including the critically ill. The purpose of this study was to identify common organisms and their susceptibilities in the respiratory isolates of trauma patients diagnosed with pneumonia within the first 7 days of hospital admission, and to create a TAP-specific disease-state antibiogram to guide empiric antibiotic therapy in this patient population.
Methods This study was a retrospective review of adult trauma patients with pneumonia admitted between September 1, 2015 and August 31, 2018. Patients included were diagnosed with and treated for pneumonia, with respiratory cultures drawn within the first 7 hospital-days; both culture-positive and culture-negative patients were included. Subgroup antibiograms were made for diagnosis made on days 1–3, 4–5, and 6–7.
Results There were 131 patients included with a median age of 45; 85% were male, and 31% were illicit drug users. Most patients (63%) had ventilator-associated pneumonia, and most respiratory samples (77%) were obtained via bronchoalveolar lavage. Cultures were positive in 109 patients and negative in 22. There were 144 total isolates; 54% were Gram-negative bacteria. The most common Gram-negative pathogens were Haemophilus influenzae (16%) and Klebsiella pneumoniae (15%). The most common Gram-positive pathogen was Staphylococcus aureus; methicillin-resistant S. aureus (MRSA) constituted 8% of all isolates. With culture-negative patients counted as susceptible, ceftriaxone monotherapy and ceftriaxone+vancomycin susceptibilities were 85% and 94%, respectively. Susceptibilities to cefazolin, ampicillin/sulbactam, cefepime, piperacillin/tazobactam, and levofloxacin were 49%, 69%, 91%, 90%, and 92%, respectively. Illicit drug use and day of pneumonia diagnosis did not appreciably affect antibiotic susceptibilities.
Conclusions For TAP diagnosed within the first 7 days of hospital admission, ceftriaxone monotherapy is adequate as empiric therapy, including in ventilated patients. The addition of vancomycin can be considered in patients with MRSA risk factors or who are critically ill.
Level of evidence Level III, prognostic and epidemiological.
- pneumonia
- epidemiology
- infections
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Among the various infectious complications that trauma patients may experience, pneumonia is one of the leading causes.1 Although Infectious Diseases Society of America (IDSA) and American Thoracic Society guidelines2 3 make recommendations for the treatment of patients with community-acquired (CAP), hospital-acquired (HAP), and ventilator-associated pneumonia (VAP), they do not address specific populations, including trauma patients who may have unique attributes and bacteriology.
Trauma patients are often younger and with fewer pre-existing comorbidities than other patient populations in the hospital. Therefore, in pneumonias that develop early in the course of their hospital admissions, the causative organisms may be composed of fewer drug-resistant bacteria. Previous studies have found that trauma patients who develop pneumonia have better outcomes,4 5 and have fewer drug-resistant pathogens,6 7 as compared with surgical intensive care unit or medical intensive care unit patients. Because of these differences, it may be reasonable to treat trauma patients with different empiric antibiotic regimens.
The purpose of this study is to examine the susceptibilities of respiratory isolates in trauma patients with pneumonia diagnosed within the first 7 days of admission and create an antibiogram specific to trauma patients with pneumonia to help guide empiric antibiotic therapy in this patient population. The second goal was to determine if it is feasible to adequately treat pathogens with empiric antibiotics that do not have activity against Pseudomonas aeruginosa or methicillin-resistant Staphylococcus aureus (MRSA) to improve antibiotic stewardship.
Patients and methods
Study design and outcome measures
In this retrospective electronic chart review conducted at a level I trauma center, trauma patients ≥18 years of age diagnosed with and treated for pneumonia within the first 7 days of hospital admission were evaluated. A list of trauma patients admitted between September 1, 2015 and August 31, 2018 classified as having pneumonia by the trauma registry was cross-referenced with a list of all patients with sputum, quantitative bronchoalveolar lavage (BAL), or endotracheal cultures drawn during this time period. Trauma patients >18 years of age diagnosed with and treated for pneumonia as documented in physician notes with BAL, endotracheal, or sputum samples drawn within the first 7 days of admission were included. Both culture-positive and culture-negative patients were included. Patients who were transferred to the study hospital after more than 24 hours of admission at an outside hospital were excluded.
Patient demographics and baseline data were collected to describe the patient population. Antimicrobial regimens prior to initiation of antibiotics for pneumonia and results of respiratory cultures were also collected. Cultures collected via BAL—both BAL and mini-BAL—were quantitative, with cultures obtained via this method counted as positive only if there was growth of >105 organisms. If multiple respiratory samples were drawn for the same patient, only the first was used in the creation of the disease-state antibiogram. Susceptibilities were based on susceptibilities as reported by the microbiology lab. For certain pathogens, susceptibilities were not reported for every antibiotic but were interpreted based on national susceptibilities and Clinical Laboratory Standards Institute guidelines, for inherently resistant or inherently susceptible drug-organism pairs. For ampicillin/sulbactam, Streptococcus sp, Haemophilus influenzae, and Pasteurella multocida were presumed sensitive, and Serratia marcescens and Enterobacter sp were presumed resistant.8–11 For cefazolin, Streptococcus sp, H. influenzae, P. multocida, S. marcescens, and Enterobacter sp were presumed resistant.8–11 For ceftriaxone, H. influenzae and P. multocida were presumed sensitive.8–11 For cefepime, H. influenzae and P. multocida were presumed sensitive.8–11 For piperacillin/tazobactam, Streptococcus sp, H. influenzae, and P. multocida were presumed sensitive.8-11 For meropenem, H. influenzae and P. multocida were presumed sensitive.8–11 H. influenzae was also presumed sensitive to levofloxacin.8 9 12
For ceftriaxone, susceptibilities were calculated using both ‘best-case’ and ‘worst-case’ scenarios. In the worst-case scenario, every organism harboring inducible chromosomal ampC beta-lactamases was presumed resistant to ceftriaxone, even if the organism was reported as susceptible. In the best-case scenario, if the organism was reported as susceptible to ceftriaxone, it was counted as susceptible. Specifically, these organisms were S. marcescens, Providencia sp, Morganella morganii, Citrobacter sp, and Enterobacter sp.13
For culture-negative patients, they were included in the antibiogram as being susceptible to ceftriaxone, cefepime, piperacillin/tazobactam, meropenem, and levofloxacin based on previous studies of patients with culture-negative healthcare-associated pneumonia. These studies have found that culture-negative patients treated with traditional CAP therapy have similar outcomes as those treated with broad-spectrum agents.14
Subgroup antibiograms were made for patients with and without illicit drug use, and patients with pneumonia diagnosis made on hospital days 1–3, 4–5, and 6–7.
Statistical analysis
Means and SDs were recorded for continuous variables. Counts, percents, and modes were recorded for categorical variables.
Results
After cross-referencing a list of all trauma patients diagnosed within the study’s 3-year timespan with a list of all patients who had cultures drawn within that time, a list of 325 patients was obtained. A total of 131 patients were included, with the most common exclusions occurring as a result of pneumonia developing after 7 days (figure 1).
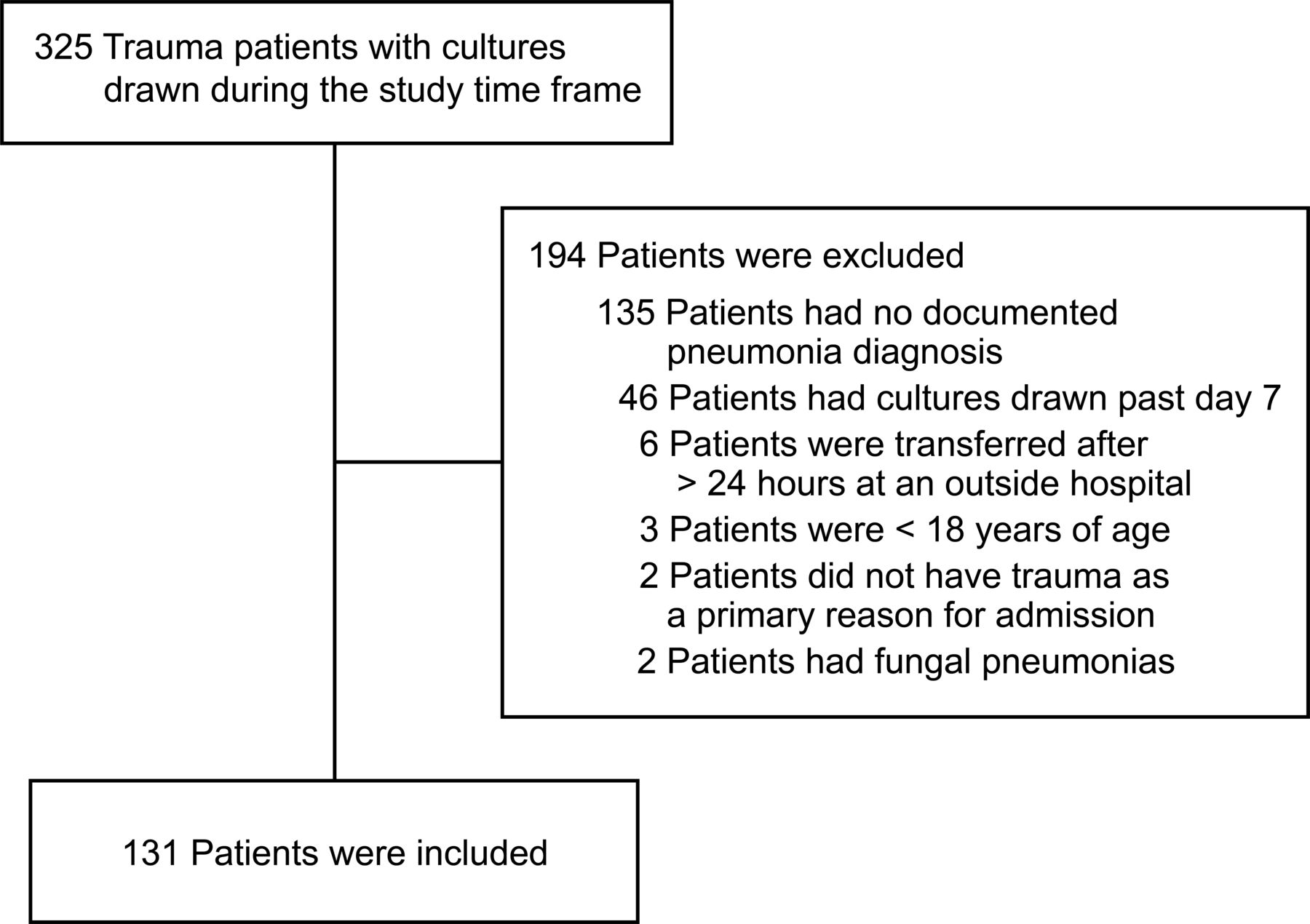
Patient flow diagram.
Baseline characteristics are shown in table 1. Briefly, patients had a median age of 45, and were mostly males. Patients had few comorbidities overall, although 31% were illicit drug users by urine toxicology screen or patient report. Head Abbreviated Injury Scale (AIS) and chest AIS had bimodal distributions, with most patients having scores of either 0 or 3 or more. Glasgow Coma Scale (GCS) also had a bimodal distribution, with most patients having GCS score of either 3 or 14 or 15. The majority of pneumonias were categorized as VAP, with median time to diagnosis of 4 days from admission.
Patient and injury characteristics
The majority of respiratory samples were obtained via BAL (table 2). Cultures were positive in 109 patients (83%) and negative in 22. There were 144 total isolates; 54% were Gram-negative bacteria. The most common Gram-negative pathogens were H. influenzae and Klebsiella pneumoniae. The most common Gram-positive pathogen was S. aureus. MRSA and P. aeruginosa constituted 8% and 5% of all isolates, respectively.
Characteristics of respiratory samples
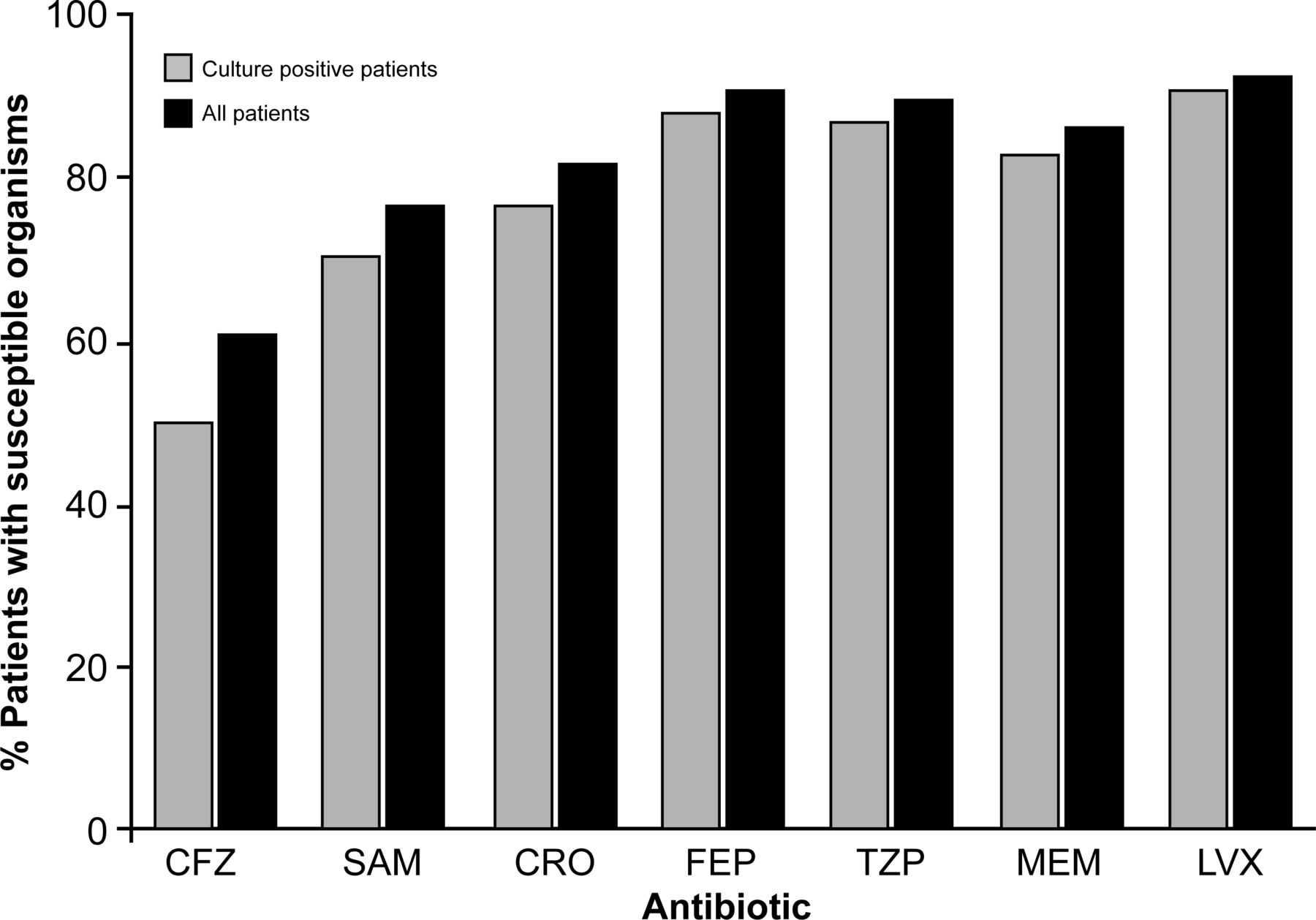
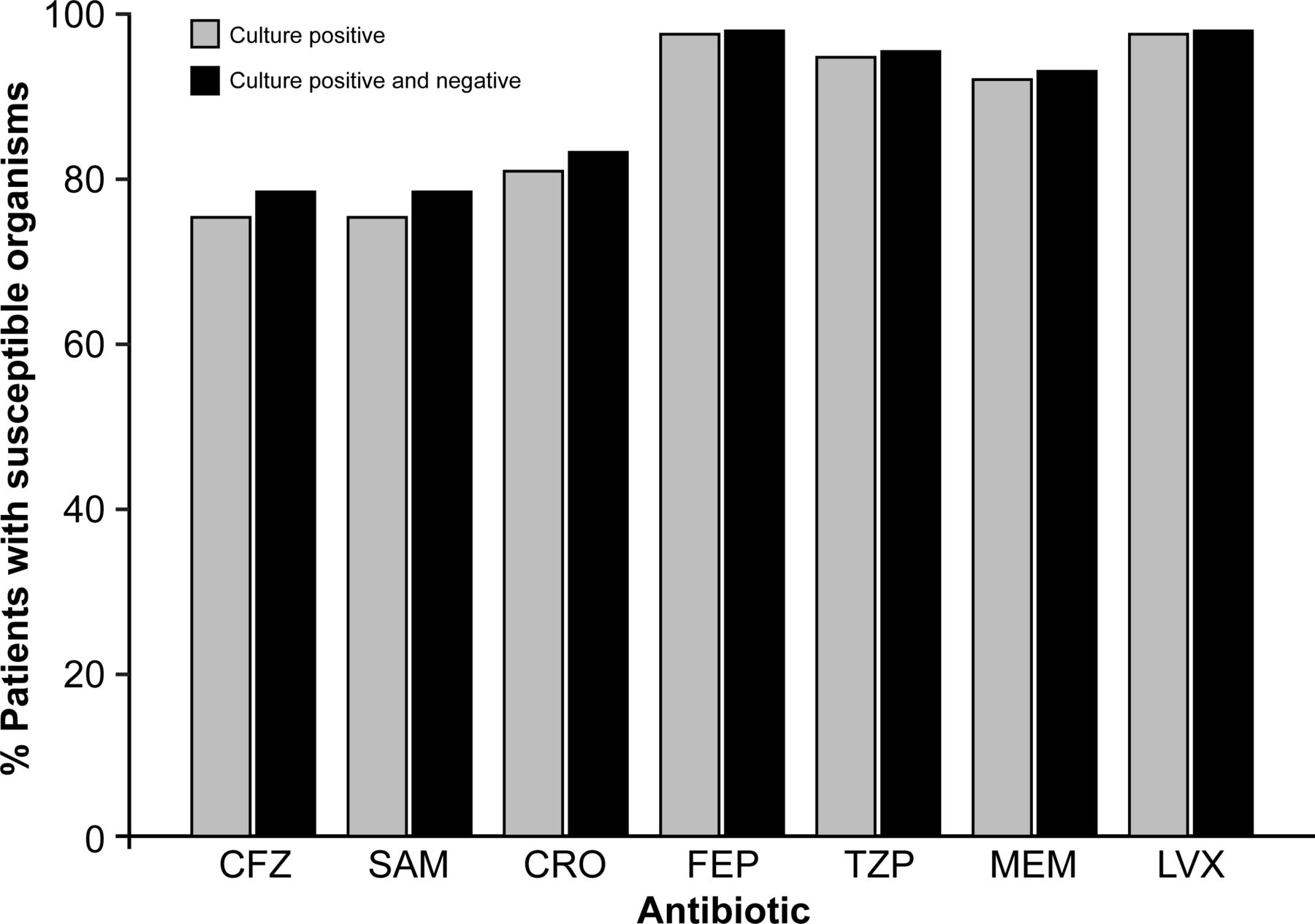
The antibiogram for all organisms is shown in figure 2. With culture-negative patients included, cefazolin and ampicillin/sulbactam had activity in 57% and 74% of all patients, respectively; the other antibiotics had better activity. As the only agent without activity against Pseudomonas spp, among culture-positive patients only, ceftriaxone was active in 74% of all pneumonias in the worst-case scenario and 83% in the best-case scenario; among all patients including those who were culture negative, ceftriaxone was active in 79% of patients in the worst-case scenario and 85% of patients in the best-case scenario. The combination of vancomycin and ceftriaxone had activity against 87% of all patients in the worst-case scenario and 94% of all patients in the best-case scenario. As BAL samples are the most reliable method of obtaining cultures, a separate analysis of susceptibilities was done for only patients with cultures obtained via quantitative BAL. The antibiogram for this subgroup only is shown in figure 3, and had similar susceptibilities as compared with the overall patient population.
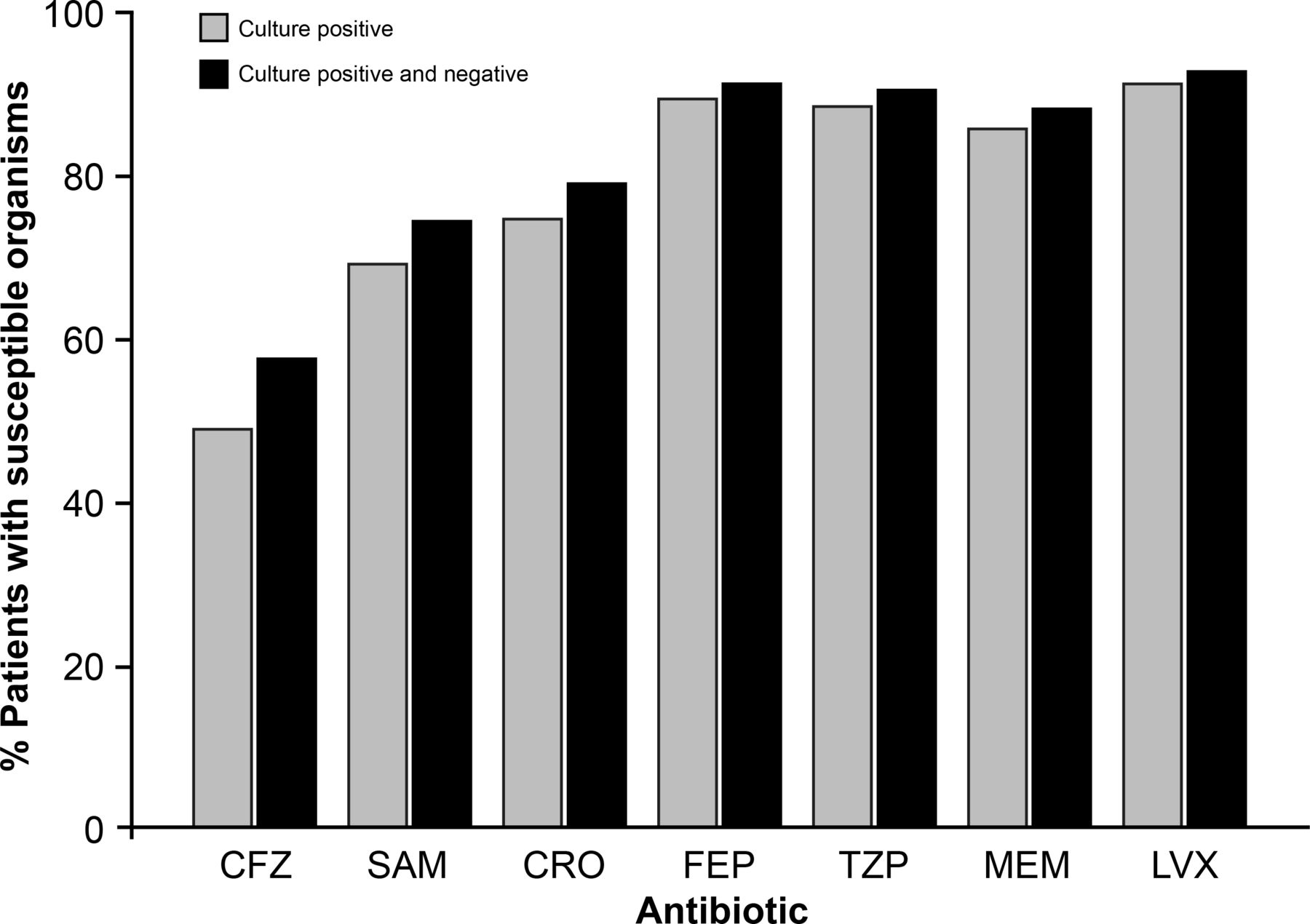
Antibiogram for all included patients. CFZ, cefazolin; CRO, ceftriaxone; FEP, cefepime; LVX, levofloxacin; MEM, meropenem; SAM, ampicillin/sulbactam; TZP, piperacillin/tazobactam.
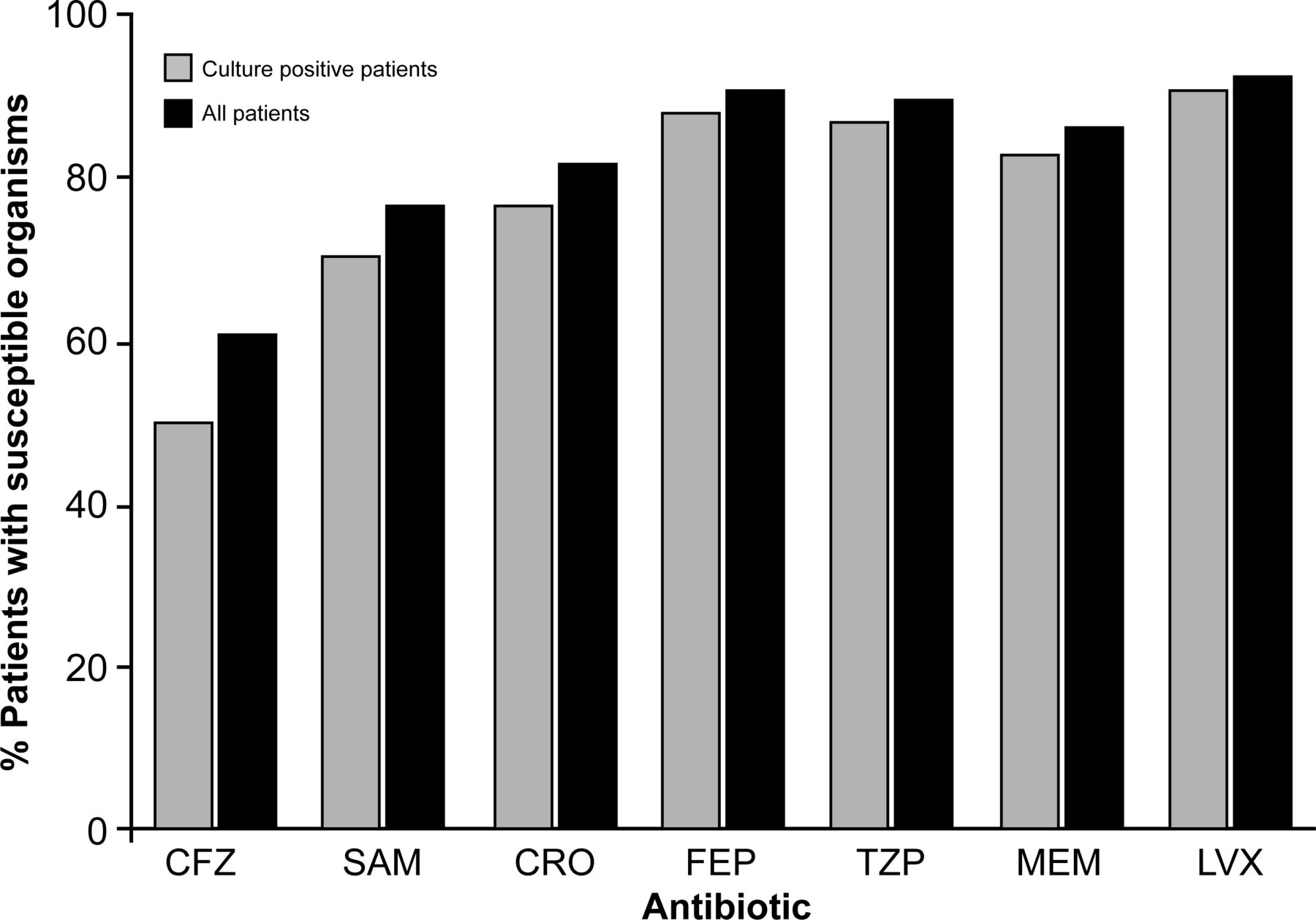
Antibiogram for only bronchoalveolar lavage (BAL) sampled patients. CFZ, cefazolin; CRO, ceftriaxone; FEP, cefepime; LVX, levofloxacin; MEM, meropenem; SAM, ampicillin/sulbactam; TZP, piperacillin/tazobactam.
The subgroup antibiogram for illicit drug users is shown in figure 4; the characteristic of illicit drug use did not appreciably affect susceptibilities. The subgroup antibiogram for pneumonia diagnosis on days 6–7 is shown in figure 5; even in patients diagnosed on day 6 or 7, ceftriaxone susceptibilities were no worse than the overall population.

Antiobiogram for illicit drug users. CFZ, cefazolin; CRO, ceftriaxone; FEP, cefepime; LVX, levofloxacin; MEM, meropenem; SAM, ampicillin/sulbactam; TZP, piperacillin/tazobactam.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Antibiogram days 6–7. CFZ, cefazolin; CRO, ceftriaxone; FEP, cefepime; LVX, levofloxacin; MEM, meropenem; SAM, ampicillin/sulbactam; TZP, piperacillin/tazobactam.
Discussion
IDSA antimicrobial stewardship guidelines endorse having disease-specific recommendations for individual disease states, and previous studies have used disease-state antibiograms to guide therapy and improve outcomes in other diseases.15 16 In this retrospective cohort study, the use of a disease-specific antibiogram demonstrates the ability to use ceftriaxone empirically for trauma-associated pneumonia (TAP) diagnosed within the first 7 days of hospital admission without the need for broader agents such as cefepime, piperacillin/tazobactam, or vancomycin. Organisms were sensitive to ceftriaxone 79% of the time in the worst-case scenario and 85% in the best-case scenario. The combination of vancomycin and ceftriaxone was active 87% of the time in all patients in the worst-case scenario and 94% of the time in all patients in the best-case scenario. These results were consistent across the subgroups of illicit drug use and hospital day of pneumonia diagnosis. Balancing the need for adequate empiric activity with the goal of avoiding antibiotic spectrum that is unnecessarily broad, we conclude that ceftriaxone monotherapy is adequate as empiric therapy in TAP. The addition of vancomycin can be considered in patients with MRSA risk factors—defined by the IDSA HAP and VAP guidelines as recent intravenous antibiotic use within the last 90 days or currently residing in an intensive care unit in which there is a high prevalence of healthcare-associated MRSA—or in those who are critically ill, such as those in septic shock in which it would be unacceptable to miss this rare but important pathogen.
Similar to other studies, our patients with TAP were younger with fewer comorbidities, and grew fewer resistant organisms than non-trauma patients with VAP. In Magret et al’s4 study, the most prevalent pathogens in early trauma VAP were Enterobacteriaceae, methicillin-sensitive S. aureus (MSSA), and H. influenzae, whereas patients with early non-trauma VAP more commonly grew P. aeruginosa and MRSA. Similarly, in Agbaht et al’s6 study, patients with early trauma VAP had more MSSA, whereas patients with early non-trauma VAP had more MRSA and P. aeruginosa. Our study also demonstrated H. influenzae and S. aureus as the most common Gram-negative and Gram-positive pathogens.
One study to examine susceptibilities in this patient population was a single-center study in patients with trauma VAP looking at causative pathogens’ susceptibilities to ampicillin/sulbactam.17 Resistance to ampicillin/sulbactam between days 3 and 7 was 26% to 50%, and the authors concluded that ampicillin/sulbactam was inadequate as empiric therapy in their patient population. This study demonstrated a rate of activity for ampicillin/sulbactam of only 74% but differs in that additional antibiotic choices were examined to further define optimal therapy.
In another single-center study, the authors also examined pathogens and susceptibilities in trauma patients with pneumonia.18 Overall rates of susceptibility were 74% for ceftriaxone and 84% for ceftriaxone plus vancomycin. When the authors divided groups into early versus late pneumonia, patients with early pneumonia (days 1–5) had susceptibilities of 83% to ceftriaxone and 93% to vancomycin plus ceftriaxone, whereas patients with late pneumonia (beyond day 5) had susceptibilities of 57% to ceftriaxone and 66% to vancomycin plus ceftriaxone. Based on these susceptibilities, the authors recommend at their institution ceftriaxone plus vancomycin for patients with TAP within the first 5 days, and vancomycin plus piperacillin/tazobactam for patients with TAP with pneumonia beyond the first 5 days. Our study examined only early TAP, which we defined as pneumonia diagnosed within the first 7 days. Our susceptibilities for early TAP were similar to those in the study by Becher et al, although we extended early TAP to the first 7 days of hospitalization and found in subgroup analyses that patients who developed pneumonia on days 6–7 had similar susceptibilities to those diagnosed within the first 5 days. Therefore, in contrast to this previous study, we recommend ceftriaxone within the first 7 days, with addition of vancomycin for patients with risk factors. Recognizing that susceptibilities often differ by institution, our study and that by Becher et al conducted at two different institutions with similar findings with regard to susceptibilities are reassuring with regard to wider applicability across the trauma population and reassure that susceptibilities have not changed significantly over time between the two studies.
Data were displayed for ceftriaxone with both best-case and worst-case scenarios, to account for inducible or derepression of AmpC beta-lactamases that are constitutively present although not always expressed in a subset of organisms. When this enzyme is expressed it can destroy ceftriaxone at a rate fast enough to cause resistance. Previous studies have shown resistance development on therapy as high as 19% in Enterobacter spp bacteremia,19 but a review of the literature has shown much lower rates of 0% to 5%13 20 across a variety of organisms and disease states. Although most of the organisms within the study that have AmpC enzymes were Enterobacter spp, the rate of on-therapy susceptibility for these organisms is likely much closer to the best-case scenario than the worst-case scenario and thus our conclusions are based on these data.
One potential limitation of this study was our assertion that culture-negative patients were susceptible to ceftriaxone. Previous data in the Healthcare associated pneumonia (HCAP) literature support similar efficacy to broader spectrum agents in the culture-negative population.14 Additionally, other data sets and IDSA VAP guidelines support discontinuation of all antibiotics in BAL culture-negative patients when pneumonia is suspected, thus indicating that ceftriaxone would not be an unacceptably narrow agent in our patients.3 21
Another limitation is that this is a single-center retrospective study and our bacterial susceptibilities may differ from other institutions secondary to baseline rates of resistance in the community and infection prevention practices after hospitalization. Although local infection patterns should always be considered when selecting empiric therapy, many hospitals do not have disease-state antibiograms specific to TAP and, as mentioned above, this is the second study from a geographical and time-distinct perspective indicating ceftriaxone is a suitable first-line agent for TAP, particularly within the first 7 days. Trauma programs uncomfortable with this approach without local data should use the data here as justification to investigate their own local susceptibilities. Lastly, some patients received antibiotics before cultures were drawn for non-pneumonia reasons. This could have potentially affected culture growth, although these antibiotics were most commonly cefazolin and cefuroxime for prophylaxis related to trauma and surgery. If these drugs did suppress growth of organisms, those organisms would likely also be susceptible to ceftriaxone.
In conclusion, for trauma patients diagnosed with pneumonia within the first 7 days of hospital admission, ceftriaxone monotherapy is adequate as empiric therapy, with the addition of vancomycin for patients with MRSA risk factors or who are critically ill.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Ethics approval
This study obtained approval from the St Joseph’s Hospital and Medical Center’s internal Institutional Review Board with a waiver of informed consent (approval number: PHXA-18-500-261-73-21), and was approved by the Dignity Health Institutional Review Board.
References
Footnotes
Contributors MHT: literature search, study design, data collection, data analysis, data interpretation, writing. JJR, JAW: study design, data analysis, data interpretation, critical review. MDN: study design, data analysis, data interpretation, writing, critical review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.