Article Text

Abstract
Background Aggressive crystalloid resuscitation increases morbidity and mortality in exsanguinating patients. Polytrauma patients with severe tissue injury and subsequent inflammatory response without major blood loss also need resuscitation. This study investigated crystalloid and blood product resuscitation in non-exsanguinating polytrauma patients and studied possible adverse outcomes.
Methods A 6.5-year prospective cohort study included consecutive trauma patients admitted to a Level 1 Trauma Center intensive care unit (ICU) who survived 48 hours. Demographics, physiologic and resuscitation parameters in first 24 hours, Denver Multiple Organ Failure scores, adult respiratory distress syndrome (ARDS) data and infectious complications were prospectively collected. Patients were divided in 5 L crystalloid volume subgroups (0–5, 5–10, 10–15 and >15 L) to make clinically relevant comparisons. Data are presented as median (IQR); p value <0.05 was considered significant.
Results 367 patients (70% men) were included with median age of 46 (28–61) years, median Injury Severity Score was 29 (22–35) and 95% sustained blunt injuries. 17% developed multiple organ dysfunction syndrome (MODS), 4% ARDS and 14% died. Increasing injury severity, acidosis and coagulopathy were associated with more crystalloid administration. Increasing crystalloid volumes were associated with more blood products, increased ventilator days, ICU length of stay, hospital length of stay, MODS, infectious complications and mortality rates. Urgent laparotomy was found to be the most important independent predictor for crystalloid resuscitation in multinominal regression analysis. Further, fresh frozen plasma (FFP) <8 hours was less likely to be administered in patients >5 L compared with the group 0–5 L. With increasing crystalloid volume, the adjusted odds of MODS, ARDS and infectious complications increased 3–4-fold, although not statistically significant. Mortality increased 6-fold in patients who received >15 L crystalloids (p=0.03).
Discussion Polytrauma patients received large amounts of crystalloids with few FFPs <24 hours. In patients with <10 L crystalloids, <24-hour mortality and MODS rates were not influenced by crystalloid resuscitation. Mortality increased 6-fold in patients who received >15 L crystalloids ≤24 hours. Efforts should be made to balance resuscitation with modest crystalloids and sufficient amount of FFPs.
Level of evidence Level 3.
Study type Population-based cohort study.
- resuscitation
- multiple trauma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Aggressive resuscitation with crystalloid fluids has long been the basis of early management of hemorrhagic shock. In the 1990s, reports on delayed fluid resuscitation for hypotensive patients with penetrating torso injuries were published.1 A decade later, it became apparent that liberal crystalloid administration was associated with adverse clinical outcomes in the blunt trauma population.2 3 Several retrospective studies have investigated the role of crystalloid resuscitation in hemorrhagic shock and triggered a shift toward a reduced crystalloid volume and an increase in blood component products in resuscitation of patients with hemorrhagic shock.4–9
Severely injured patients who experience blood loss without imminent exsanguination also experience tissue injury with accompanying acidosis and coagulopathy, which triggers a systemic inflammatory response.10 The endothelium activated by exposure to inflammatory cytokines becomes more porous, allowing mediators of tissue damage to gain access to the intercellular space causing tissue edema.11 These patients also need to be adequately resuscitated even though they have only mild/moderate blood loss (class II–III shock according to Advanced Trauma Life Support (ATLS)12 with initial hemoglobin levels often close to normal. Several resuscitation fluids other than normal saline or Ringer’s lactate have been investigated such as hypertonic saline and colloids with disappointing results.9 13 Further, Inaba et al14 have shown a decade ago that plasma administration in non-massively transfused trauma patients was associated with a substantial increase in multiple organ dysfunction syndrome (MODS) and adult respiratory distress syndrome (ARDS) with no improvement in survival. Other studies, however, have shown a beneficial effect of fresh frozen plasma (FFP) that may be related to the restoration of injured endothelium. In animal studies, FFP was found to improve endothelial integrity with decreased endothelial cell hyperpermeability and inflammation.15–17
To date, it remains largely unclear what the best resuscitation options are in patients who are severely injured, but do not expire from severe blood loss. Although these patients do not immediately need packed red blood cells, they are in need of volume resuscitation. Since too much crystalloids are detrimental, other fluids need to be considered. Therefore, we conducted a prospective cohort study investigating resuscitation methods and possible adverse outcomes in these non-exsanguinating, polytrauma patients.
Materials and methods
Study setting
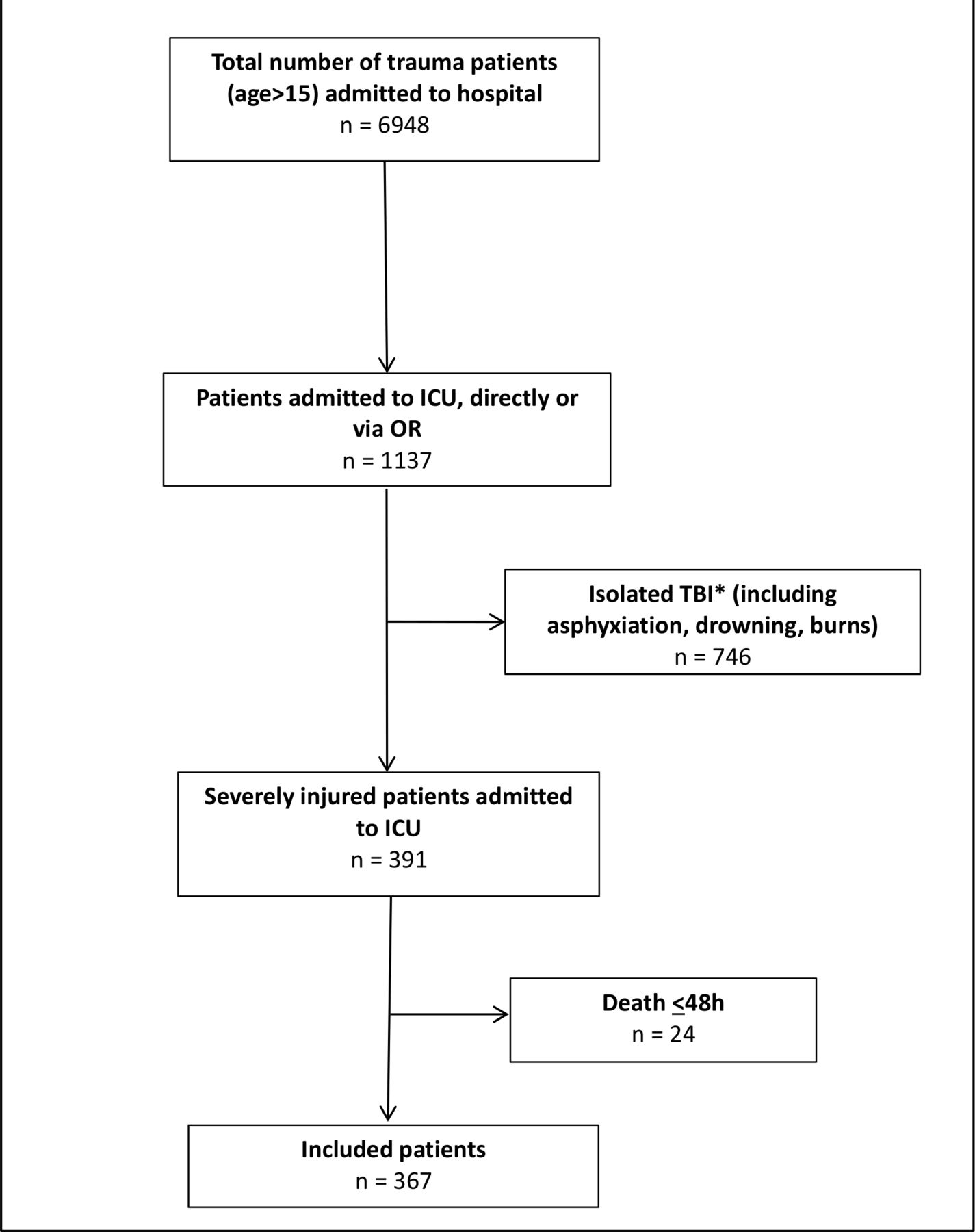
The study was conducted at an urban major (Level 1) trauma center. From November 2013, a 6.5-year prospective population-based cohort study was undertaken to investigate outcomes in severely injured patients admitted to the intensive care unit (ICU) of the University Medical Center Utrecht. Detailed characteristics of the hospital and catchment area were previously described.18 All consecutive severely injured trauma patients >15 years of age who were admitted to ICU either directly from the emergency department (ED) or postoperatively after urgent surgery and survived >48 hours were included. Patients with isolated injury to the brain (Abbreviated Injury Score (AIS) head 3 or more and AIS 2 or less in other regions), asphyxiation, drowning and burns were excluded because of a possible different physiologic response to severe trauma and a significantly different mortality and morbidity profile.19 20 A flowchart of patient inclusion is shown in figure 1.

Flowchart of included patients. *Isolated traumatic brain injury (TBI) was defined as Abbreviated Injury Score (AIS) head >3 and AIS <2 or less in other regions.
Data collection
All data were prospectively collected on arrival in ED and on a daily basis in ICU by the authors (KvW, LL) and included patient demographics, Injury Severity Score (ISS), shock and resuscitation parameters. Both crystalloid (normal saline and/or Ringer’s lactate) and blood product (packed red blood cells (PRBCs), FFP and platelets (PLT)) administration was recorded in the first 24 hours following admission. This included resuscitation fluids that were administered in the operating room (OR) provided surgery was performed within first 24 hours. Resuscitation protocol has not changed during the studied period other than that initial crystalloid resuscitation changed from 2 L to 1 L in 2018 according to the updated ATLS 10th edition.12
Further, patients were divided in 5 L volume subgroups to be able to make clinically relevant comparisons (0–5 L, 5–10 L, 10–15 L and >15 L crystalloids <24 hours). These subgroups were chosen in analogy to a previous Glue Grant Database study investigating crystalloid resuscitation in trauma patients.7 By hospital protocol, class III and IV shock criteria according to ATLS,12 and/or base deficit (BD) >6 mmol/L in ED with signs of blood loss were indications to start blood product transfusion in a 1:1:1 ratio. Resuscitation goals were normalization of tissue perfusion (acidosis) and coagulopathy.
Denver Multiple Organ Failure (MOF) scores and ARDS Berlin criteria were registered daily up until 28 days or discharge from ICU. Primary outcome was the relation between crystalloid resuscitation ≤24 hours and mortality. Secondary outcome was the relation between crystalloid resuscitation and complications such as MODS, ARDS and infectious complications.
Definitions
MODS was defined by Denver MOF scores of greater than 3, occurring more than 48 hours after injury.21 Denver MOF score was chosen over Sequential Organ Failure Assessment to avoid difficulties by including the Glasgow Coma Scale (GCS) in the organ failure score. GCS can be challenging to obtain in trauma patients in ICU because they are often sedated and intubated for extended periods. This could negatively influence the central nervous system organ failure score.20
ARDS was defined by the Berlin criteria based on degree of hypoxemia and presence of bilateral diffuse pulmonary infiltrates (without evidence of heart failure) on chest X-ray or CT scan.22 In addition, infectious complications were registered. Definitions and type of infectious complications that were registered have been previously described.23
Urgent laparotomy was defined as a laparotomy that was performed in patients who were transported from ED directly (or via CT scan) to OR.
Exsanguination was defined as having the most extreme form of hemorrhage, with an initial blood loss of >40% (class IV shock according to ATLS) and ongoing bleeding that, if not surgically controlled, will lead to death.24 Non-exsanguinating patients were defined as having an estimated blood loss based on clinical signs and symptoms of less than 40% (class I to III shock according to ATLS).12 Non-exsanguination was used as opposite of exsanguination in order to define a group of patients who are in need of volume resuscitation but do not necessarily need large volumes of PRBCs based on blood loss.
Statistical analysis
Data were analyzed using IBM SPSS Statistics, V.25.0. Graphs were prepared with GraphPad Prism V.8.3.0 (San Diego, CA, USA). Results are presented as median and IQR. Comparison of variables was done using Kruskal-Wallis test or Pearson χ2 test in dichotomous data. Variables with univariate statistical significance were included in a multinominal logistic regression analysis. These variables were analyzed to identify independent risk factors for the predefined groups of crystalloid resuscitation and presented as ORs and 95% CIs. Statistical significance was defined as p value <0.05.
Results
Demographics
In total, 367 patients (70% male) with a median age of 46 (28–61) years who were admitted to ICU and survived 48 hours were included. Ninety-six percent of injuries were caused by a blunt mechanism and median ISS was 29 (22–35) with most severe injuries located in the brain (AIS head 3 (1–3)) and chest (AIS chest 3 (2–4)). Eighty-six patients (23%) underwent an urgent laparotomy (table 1). Physiological parameters of patients who underwent a laparotomy and injuries found during urgent laparotomy are described in online supplemental table S1.
Supplemental material
Demographics
Median first measured systolic blood pressure (SBP) in ED was 120 (100–140) mm Hg, and 70 patients (19%) had a SBP <90 mm Hg on arrival in ED. First measured hemoglobin (Hb) in ED was 8.0 (7.2–8.9) mmol/L and in ICU 7.6 (6.8–8.3) mmol/L. First measured BD in ED was 3.0 (0.0–6.0) mmol/L and in ICU 3.8 (1.8–6.0) mmol/L. Patients received 7.4 (5.0–10.2) L of crystalloids <24 hours. Further, they received 1 (0–5) U PRBCs <24 hours, 0 (0–5) U FFP <24 hours and 0 (0–1) U PLT <24 hours.
There was no difference in the amount of administered crystalloids <24 hours nor in blood products ≤24 hours between years within the studied period (2013–2020). Thirty-seven (10%) patients received massive transfusion (≥10 PRBCs <24 hours, table 1). Median ISS in these massively transfused patients was 34 (27–41). SBP in ED was 84 (75–112) mm Hg, 22 (59%) of them presented with SBP <90 mm Hg and 21 (57%) patients underwent an urgent laparotomy. Initial Hb was 6.8 (5.5–7.6) mmol/L, BD 9.5 (4.0–14.3) mmol/L and prothrombin time (PT) 17.9 (16.1–21.1) s, confirming this group was severely injured with deranged physiology (online supplemental table S2).
Supplemental material
Patients stayed 6 (2–11) days on the ventilator, 7 (3–14) days in ICU and 21 (13–32) days in hospital. No patient developed abdominal compartment syndrome, Sixty-two (17%) patients developed MODS. The majority of individual organ failure was pulmonary and cardiac. Hepatic failure (5 patients) and renal failure (10 patients) were rare (online supplemental figure S1). Sixteen (4%) patients developed ARDS and 165 (45%) patients developed infectious complications (table 1).
Supplemental material
In this cohort, 51 (14%) patients died; 35 (69%) patients died of traumatic brain injury (TBI), 7 (14%) died of respiratory insufficiency, 2 (4%) of cardiac origin, 2 (4%) of MODS, 2 (4%) of sepsis, 1 (2%) of ARDS, 1 (2%) of hypoxia and 1 (2%) due to ischemia.
Injury severity across different crystalloid volume groups
Nineteen patients stayed in ICU less than 24 hours, so crystalloid and blood product were not measured for full 24 hours. Therefore, they were excluded from further analysis regarding resuscitation. All other patients (n=348) were divided into four different crystalloid volume groups; 86 patients received 0–5 L <24 hours, 168 patients received 5–10 L <24 hours, 75 patients received 10–15 L <24 hours and 19 patients received >15 L ≤24 hours. Distribution of injury severity across different crystalloid volume groups and dose-dependent effect of crystalloid resuscitation on morbidity and mortality are shown in table 2. An increase in injury severity, acidosis and coagulopathy was associated with an increase in crystalloid volume. With increasing crystalloid resuscitation, patients received more units of PRBCs and FFP (p<0.001). Figure 2 shows the relation between different groups of crystalloid volume <24 hours and administration of PRBCs and FFP in operating room (OR), <8 hours and ≤24 hours. Patients who received the largest amount of crystalloids (>15 L ≤24 hours) showed PRBC:FFP ratio >1 in all measured time points.
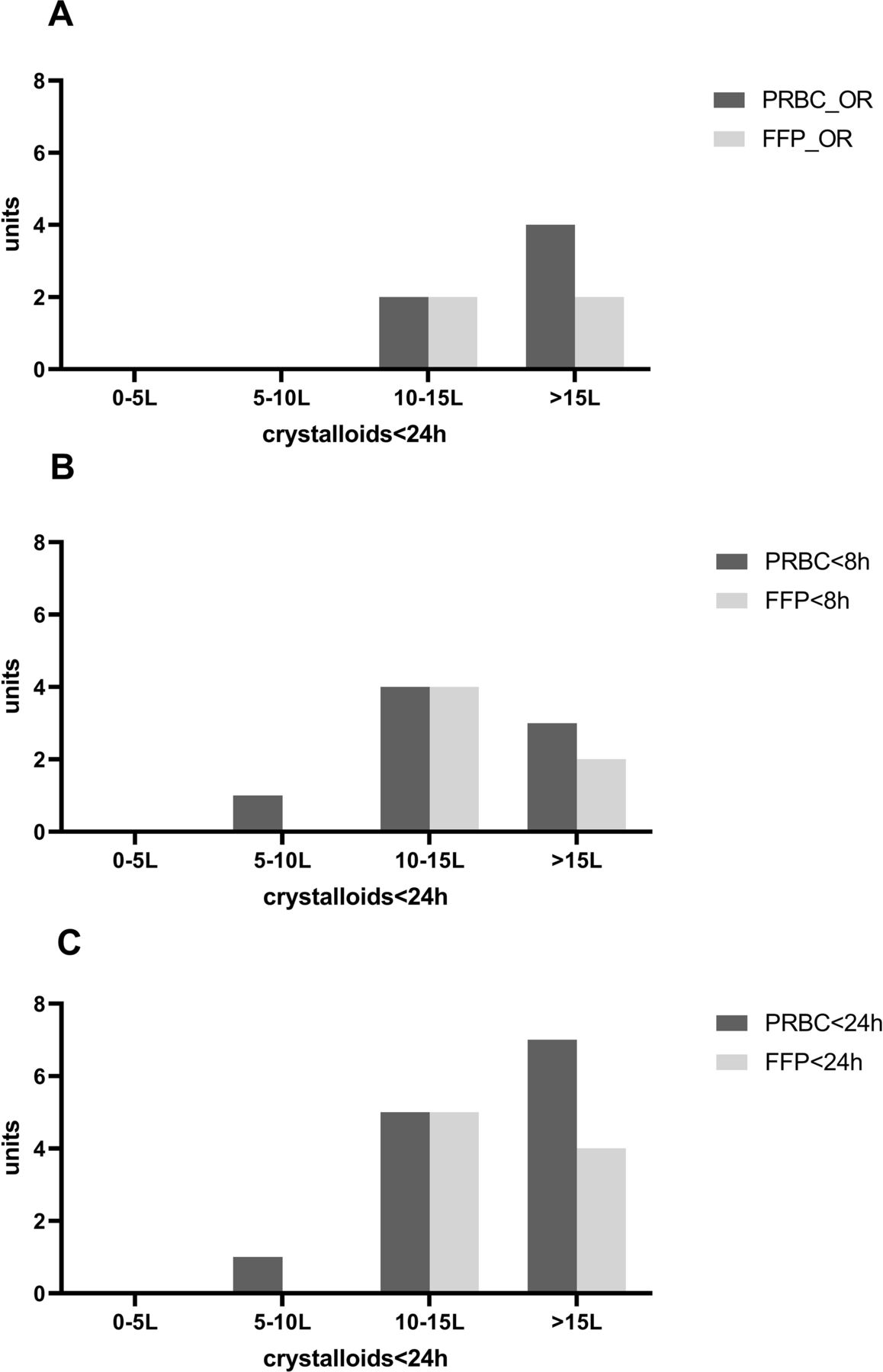
Blood products related to crystalloid administration ≤24 hours. FFP, fresh frozen plasma; OR, operating room; PRBC, packed red blood cell.
Distribution of injury severity across different crystalloid volume groups and dose-dependent effect of crystalloid resuscitation on morbidity and mortality
Increasing crystalloid volume was associated with an increase in ventilator days, ICU length of stay, hospital length of stay, MODS, infectious complications and mortality rates. The relation between crystalloid volume and ARDS did not reach statistical significance likely due to low ARDS incidence (table 2).
Multinominal logistic regression analysis was performed to identify possible predictors for different crystalloid volume groups. Also, 0–5 L crystalloid resuscitation was used as reference group. Urgent laparotomy was found to be the single most important independent predictor for crystalloid resuscitation. Further, BD in ED only was a predictor in larger crystalloid volume groups (10–15 L and >15 L, table 3). Interestingly, the odds of FFP <8 hours was lower than 1, demonstrating FFP <8 hours was less likely to be administered compared with the reference group.
Multinominal logistic regression analysis identifying possible predictors for different crystalloid volume groups
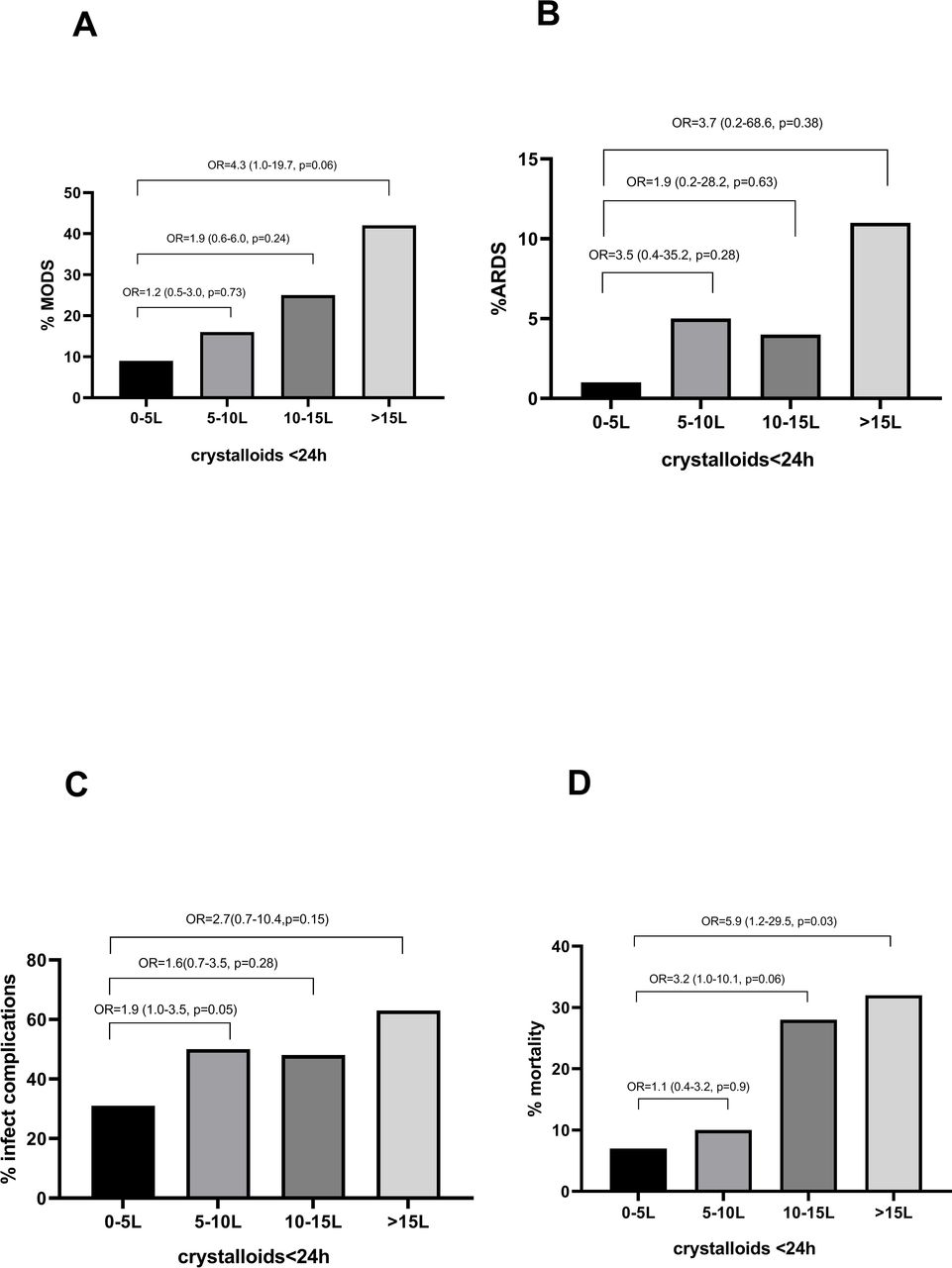
To avoid confounding from injury and physiologic derangement, injury severity, hemoglobin and BD in ED, urgent laparotomy, PRBCs ≤8 hours and ≤24 hours, and FFP ≤8 hours and ≤24 hours were controlled for in the multinominal logistic regression analysis to identify possible independent outcome predictors for different crystalloid volume groups. Adjusted ORs for MODS, ARDS, infectious complications and mortality were calculated and are shown in figure 3. With increasing crystalloid volume, the odds of MODS, ARDS and infectious complications increased threefold to fourfold, although not statistically significant. Mortality increased sixfold in patients who received ≥15 L crystalloids (p=0.03).

{kind=link}
{kind=link}
{kind=link}
Adjusted ORs for the development of (A) MODS, (B) ARDS, (C) infectious complications and (D) mortality across the four crystalloid resuscitation volume groups. ARDS, adult respiratory distress syndrome; MODS, multiple organ dysfunction syndrome.
Discussion
This is the first cohort study in which the relation between crystalloid and blood product resuscitation in severely injured but mostly non-exsanguinating patients was prospectively studied. Patients received 7.4 L of crystalloids, 1 L of PRBCs and no FFP and PLT within the first 24 hours after admission. Despite the large amount of crystalloid resuscitation, no patients developed abdominal compartment syndrome, 17% developed MODS (with low kidney failure rates) and 4% ARDS.
When analyzing different volume groups, there was an increased ISS, more deranged physiology, more urgent laparotomies and longer stay on the ventilator in ICU and in hospital with increasing crystalloid volumes. Twenty-seven percent of patients received >10 L of crystalloids ≤24 hours which was accompanied by a twofold to threefold increase in incidence of MODS (although not statistically significant different) and sixfold increase in mortality even after controlling for injury severity, physiologic derangement and blood product administration. These results are in line with others who argued that crystalloids trigger a dose-dependent acute inflammatory response.7 However, it should be noted that in this current study, despite large volumes of crystalloids, the overall MODS and ARDS rates were lower compared with others,25–28 but in line with our previous studies.23 29 30 On the other hand, infectious complication rates were 45% in this study which is comparable with other studies.31
Recently, Hatton et al32 have studied the influence of a positive fluid balance on acute kidney injury (AKI) and discovered that fluid positivity was independently and incrementally associated with AKI development. Again, this in contrast with our population since only 10 patients developed AKI.
One other downside of large amounts of crystalloids is the development of cellular acidosis.2 3 Interestingly, in this study the amelioration of base deficit between ED and ICU was largest in the patient group who received >15 L <24 hours, suggesting that development of hyperchloremic acidosis was not an issue despite large amounts of normal saline and/or Ringer’s lactate.
Too much crystalloids are detrimental, although it remains unclear what is too much. In this study, up to 10 L of crystalloids <24 hours did not seem to increase MODS and mortality whereas 5 L crystalloids <24 hours appeared to be a cut-off point for a doubling in infectious complications and ARDS, although the incidence of ARDS was likely too small to draw any conclusions. Jones et al33 previously also demonstrated that >5 L of crystalloids <24 hours was associated with adverse outcomes, although results are not fully comparable since patients in their study were less severely injured.
A few decades ago, restriction of crystalloid fluid volume before hemorrhage control with permissive hypotension was introduced in exsanguinating patients with penetrating trauma.1 Even though outcomes in this population were good, there is still no evidence of these concepts being successfully applied to the management of patients following blunt injury or those with TBI.34
In search for other measures to decrease fluid resuscitation volumes in severe trauma patients, the use of vasopressors has also been described.35 Strong support for the use of this strategy in trauma patients, however, is still lacking.36 Moreover, many of our patients had severe TBI and therefore received inotropes in order to maintain cerebral perfusion pressure.
Few blood products were administered within the first 24 hours in this cohort. Administration of few PRBCs could be explained by the fact that majority of patients, although severely injured, did not have class IV shock and therefore did not need large amounts of PRBCs. It is not fully understood why FFP administration was so low in groups that received large amounts of crystalloids even though PT in ED already was prolonged. In fact, the odds of administered FFP <8 hours was even lower than 1, showing FFP was less likely to be administered compared with the reference group. Patients who received the largest amount of crystalloids had an increased PRBC:FFP ratio. This was true for all measured time points (OR, <8 hours and ≤24 hours). Combined with urgent laparotomy being the strongest predictor for large crystalloid volumes, these data suggest that, in the future, crystalloid resuscitation should at least partially be replaced by FFPs starting in OR and to be continued for at least 24 hours after admission. Possibly, low volumes of FFPs were used by a persistent reluctance to administer larger amounts of FFP in patients who are not bleeding to death, because of its known association with MODS and ARDS. However, data on these adverse effects of FFP are a decade old, and recent animal studies have shown a beneficial effect of FFP in its ability to restore damaged endothelial glycocalyx by inhibition of syndecan-1 shedding (an important component of glycocalyx).17 This might cause a decrease in fluid leakage through the endothelium and the necessity to resuscitate with large amounts of fluids.
One of the limitations of this study is that it was conducted at a single institution in which the clinical treatment and research were conducted by the same clinicians. Another limitation is that no detailed physiological and resuscitation data were collected after 24 hours after admission. Further, since there was no existing definition for non-exsanguination, we have defined non-exsanguination as the opposite of exsanguination which has been previously defined.24 This could lead potentially to comparison issues when relating these data to other studies. In addition, one could argue whether patients who received massive transfusion and/or an urgent laparotomy should be included in the analysis since these patients had potentially major blood loss. The presented data (online supplemental tables S1 and S2), however, showed that the majority of these patients were not exsanguinating (massive transfusion was not synonymous to exsanguination), and that these patients also received large amounts of crystalloids despite blood transfusions. Interestingly, these patients received at least 10 L of crystalloids <24 hours, almost half of which was given between 8 hours and 24 hours (generally while in ICU). Within that same time frame, almost no additional blood products were administered. These are patients in whom the question arises whether they could have profited from less crystalloids and more blood products. Further, these patients functioned as “positive controls” to demonstrate that adequate blood product transfusion was used when necessary. Therefore, we feel that they should be included in analysis regarding the dilemma of crystalloid resuscitation.
In conclusion, in this study of mostly non-exsanguinating polytrauma patients, large amounts of crystalloids with few FFP <24 hours were administered. Mortality increased sixfold in patients who received >15 L crystalloids ≤24 hours. In patients who received less than 10 L crystalloids, mortality and MODS rates were not influenced by the crystalloid resuscitation although infectious complications did increase twofold. This study attempted to show the dilemma of too much crystalloid resuscitation in non-exsanguinating patients, and that other resuscitation options such as FFP might be a good alternative despite previous reports that it is associated with increased complications. Based on the results of this study, we suggest to balance resuscitation by decreasing crystalloid volume to less than 10 L <24 hours and adding FFP if necessary while vigilant on MODS and ARDS development.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KvW, FH and LPHL have contributed to the conception and design of the study. KvW and LPHL have performed acquisition of data. KvW has done the analysis and interpretation of data. KvW has drafted the article. LPHL and FH have revised it critically for important intellectual content. KvW, FH, LPHL have given final approval of the version to be submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The local ethics committee approved this prospective observational study and waived consent (reference number WAG/mb/16/026664).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The dataset supporting the conclusions of this article are available on reasonable request from the corresponding author.