Article Text

Abstract
Background Guidelines concerning outpatient management of patients during the coronavirus pandemic required minimized face-to-face follow-up and increased remote care. In response, we established a virtual fracture clinic (VFC) review for emergency department (ED) patients with musculoskeletal injuries, meaning patients are reviewed ‘virtually’ the next workday by a multidisciplinary team, instead of routine referral for face-to-face fracture clinic review. Patients wait at home and are contacted afterwards to discuss treatment. Based on VFC review, patients with minor injuries are discharged, while for other patients an extensive treatment plan is documented using injury-specific care pathways. Additionally, we established an ED orthopedic trauma fast-track to reduce waiting time. This study aimed to evaluate the extent to which our workflow supported adherence to national coronavirus-related guidelines and effects on ED waiting time.
Methods A closed-loop audit was performed during two 4-week periods using predefined standards: (1) all eligible ED orthopedic trauma patients are referred for VFC review; (2) reached afterwards; and follow-up is (3) patient initiated, or (4) performed remotely, whenever possible. Total ED waiting time, time to review, time for review, and time after review were assessed during both audit periods and compared with previous measurements.
Results During both audits, the majority of eligible ED patients were referred for VFC review (1st: n=162 (88.0%); 2nd: n=302 (98.4%)), and reached afterwards (1st: 98.1%; 2nd: 99.0%). Of all referred patients, 17.9% and 13.6% were discharged ‘virtually’ during first and second audits, respectively, while 45.0% and 41.1% of scheduled follow-up appointments were remote. Median total ED waiting time was reduced (1st: −36 minutes (p<0.001); 2nd: −33 minutes (p<0.001)). During the second audit, median ED time to review was reduced by −13 minutes (p<0.001), as well as time for review: −10 minutes (p=0.019).
Discussion In line with national guidelines, our VFC review allowed time-effective review and triage of the majority of ED orthopedic trauma patients, supporting patient-initiated and remote follow-up, whenever possible. ED waiting time was reduced after implementing the VFC review and orthopedic trauma fast-track.
Level of evidence IV.
- COVID-19
- quality improvement
- fractures
- bone
- orthopedics
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request to the corresponding author. This includes deidentified data of the waiting time measurements.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The COVID-19 pandemic was declared on 11 March 2020.1 The guidelines that were implemented for the outpatient management of patients as a result of this pandemic2 3 required considerable and pragmatic revisions of established treatment protocols in orthopedic trauma. This included patient-initiated follow-up to be the default, as well as minimizing the number of face-to-face appointments using telecommunication or video communication.2 3
The guidelines also prescribed that an attending physician should assess the medical indication and necessity of follow-up appointments, and indicate if these appointments should be conducted remotely or face to face.2 However, this was not routine prior to the pandemic, since the majority of emergency department (ED) orthopedic trauma patients were typically referred to a fracture clinic for further face-to-face review within a few days after their initial ED visit. After this appointment, a physician (often a junior resident) would then decide if and when a subsequent appointment was scheduled using local protocols.
The virtual fracture clinic (VFC) model was first established in 2011 in an effort to streamline outpatient management of orthopedic trauma patients. The VFC model concerns all ED patients with musculoskeletal injuries who do not require acute admission. It consists of two main parts.4 5 First, direct discharge from the ED of patients with simple stable injuries. This is supported by removable orthoses, a discharge leaflet and a telephone helpline. Second, all other patients with musculoskeletal injuries are discharged to home and referred for a VFC review on the next day. This is in contrast to the routine referral of all ED patients for face-to-face review at the fracture clinic. During the VFC review on the next workday, all patients are reviewed ‘virtually’. That is, the patient waits at home while a multidisciplinary team led by an orthopedic consultant evaluates their case and outlines his or her treatment. The possible outcomes of the VFC review include ‘virtual’ discharge (ie, no additional follow-up appointments), or follow-up in a nurse-led clinic or subspecialty clinic. All patients are contacted by telephone after VFC review to discuss their treatment and to schedule the corresponding appointments if applicable.4 5
Prior to the COVID-19 pandemic, our hospital had already implemented the first part of the VFC model, that is, direct discharge from the ED of patients with simple stable injuries. During the first month of the coronavirus pandemic, our hospital accelerated the implementation of the second part of the VFC model, that is, the VFC review, since we anticipated the VFC review to provide an opportunity to effectively adhere to the aforementioned coronavirus-related guidelines.2 3 That is, if a proportion of the patients can be discharged ‘virtually’, and a complete treatment plan is outlined during VFC review for all patients, this might reduce the number of unnecessary and untimely (face-to-face) follow-up appointments. Additionally, to further alleviate the increasing workload for our ED staff, and to minimize ED waiting time for orthopedic trauma patients, an orthopedic trauma fast-track pathway was implemented in the ED. This involved the use of fast-track rooms adjacent to the ED and a dedicated fast-track team.
The aim of the current study was to evaluate whether implementation of a VFC review supported our adherence to the guidelines for the outpatient management of patients during the coronavirus pandemic. Additionally, we evaluated the compliance to our new workflow (ie, both VFC review and ED fast-track pathway), and its effects on waiting time in the ED, by performing a closed-loop audit.
Methods
The Standards for Quality Improvement Reporting Excellence checklist was used while writing this article.6
Design
This was a closed-loop audit performed in a level 2 trauma center and teaching hospital in Amsterdam, the Netherlands.
Workflow
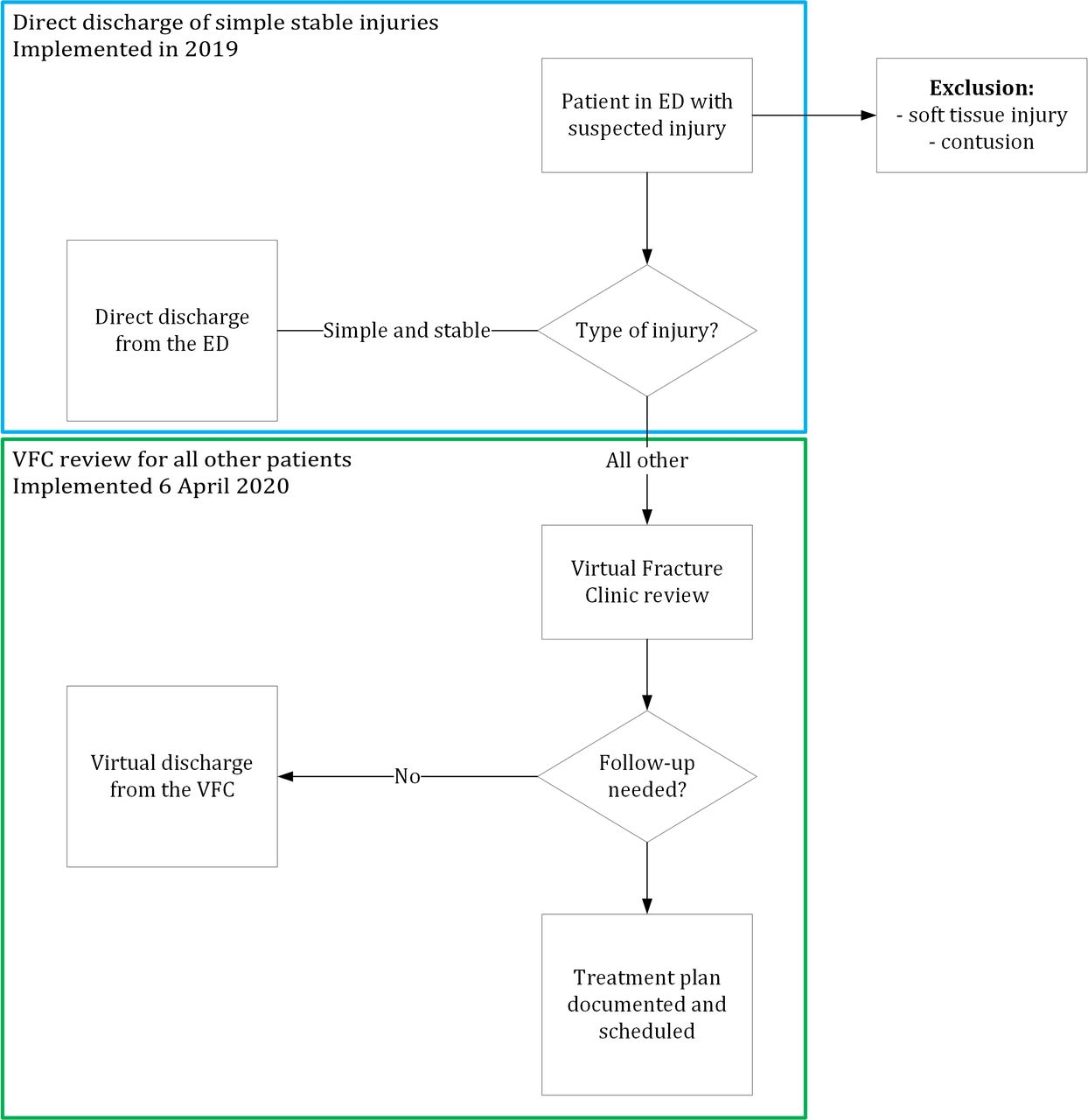
Table 1 and figure 1 provide information on the differences in workflow before and after implementing a VFC review and ED orthopedic trauma fast-track pathway. These changes were prepared during 3 weeks in March 2020 and implemented on April 6, 2020.

Virtual fracture clinic (VFC) model. Blue square: direct discharge of patients with simple stable injuries from the ED. Green square: VFC review of all other patients. ED, emergency department.
Changes to existing workflow
In our hospital, the following four categories of ED orthopedic trauma patients are generally encountered and determine what steps are required by the ED staff before patients leave the ED: (1) patients requiring immediate admission to the ward (eg, for surgery or for social care reasons); (2) patients requiring scheduled operative treatment (ie, not immediately, but within the coming days/week); (3) conservatively treated patients requiring follow-up; (4) conservatively treated patients who do not require further follow-up (ie, direct discharge from the ED).
Prechange workflow
If immediate admission to the ward was required, the on-call orthopedic consultant was contacted by the ED staff to admit the patient. If scheduled operative treatment was deemed necessary, the orthopedic consultant was contacted as well, and management was decided and discussed in the ED. For these patients, follow-up appointments were scheduled postoperatively. Conservatively treated patients requiring follow-up were routinely referred to our fracture clinic for face-to-face review and definitive management within approximately 1 week. For these patients, if necessary, any further follow-up appointments were scheduled after each subsequent follow-up appointment. Conservatively treated patients with injuries that did not require follow-up were discharged directly from the ED (figure 1).
New workflow
If immediate admission to the ward was required, workflow did not change. If scheduled operative treatment was deemed necessary, patients were immobilized, discharged to home, and referred for VFC review on the next workday. Conservatively treated patients requiring follow-up were also discharged to home and referred for VFC review, instead of the routine referral of these patients to our fracture clinic for face-to-face review. For patients with injuries that did not require follow-up, workflow did not change.
During the VFC review a multidisciplinary team evaluated the cases of all referrals. Possible outcomes of the VFC review were: (1) ‘virtual’ discharge for patients with relatively minor injuries; (2) conservative treatment, requiring follow-up; and (3) scheduled surgery within one to several days.
In its original UK version, the VFC team either ‘virtually’ discharges patients or refers patients to a nurse-led clinic or subspecialty clinic for further treatment, where further follow-up appointments are scheduled after each subsequent follow-up appointment, that is, a complete treatment plan is not documented.4 5 However, our aim was to outline an extensive and complete supervised treatment plan during the VFC review as well, since this was in line with national guidelines for the management of orthopedic trauma patients during the coronavirus pandemic (ie, to assess the necessity and indication of all follow-up appointments by an attending physician).2 To this end, we integrated all our treatment protocols as care pathways into our electronic patient record system. Our trauma team had reached consensus on these pathways by organizing consensus meetings shortly after national measures took effect in March 2020, using the national guidelines for the outpatient treatment of patients during the coronavirus pandemic, which required minimized face-to-face consultations and remote care whenever possible.
During VFC review, if necessary, the VFC team could make individual changes for each patient. This resulted in the documentation of an extensive, individual and supervised treatment plan for all patients who were not discharged ‘virtually’, including an overview of the characteristics of all appointments; for example, date, mode (face-to-face or remote review), radiological imaging (yes/no), instructions (eg, specific assessments required and if or when supervision should be sought). If necessary, this treatment plan was updated based on the course of events throughout the patient’s treatment.
After evaluation of all referrals was completed, patients were contacted by telephone to discuss and to reach agreement on their treatment plan. If applicable, admission and surgery was scheduled as well. If unable to reach the patient, a voice mail was recorded and a letter was sent to the patient and their general practitioner (GP).
An additional change was the implementation of an orthopedic trauma fast-track pathway to minimize waiting time in the ED. If deemed eligible for fast-track review and treatment by the triaging ED nurse, patients with suspected musculoskeletal injuries took place in a special fast-track waiting room. These patients were reviewed and treated by a dedicated fast-track team in one of four ‘fast-track’ rooms adjacent to the ED. These rooms were used specifically for the rapid review and treatment of patients with suspected musculoskeletal injuries.
Evaluation
To evaluate the level of compliance to our new workflow, a closed-loop audit was performed during two periods of 4 weeks (figure 2). An audit is a quality improvement process that seeks to improve patient care through the systematic review of care against explicit standards, and the implementation of change.7 It includes setting standards, testing practice against standards (first audit), and correcting practice where it falls short. The loop is then ‘closed’ by a reaudit (second audit) to confirm whether standards are met.8
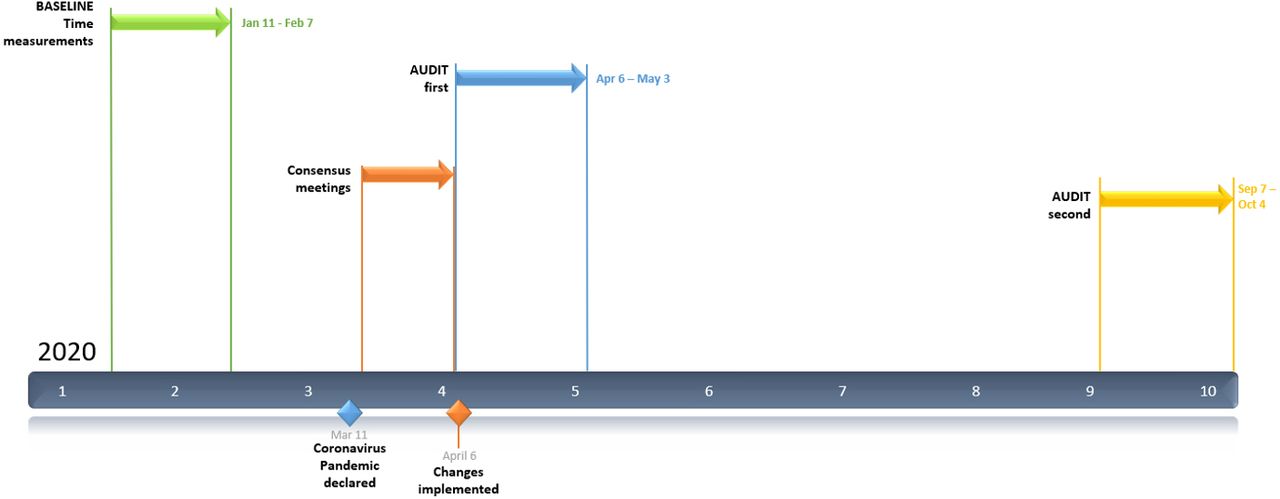
Timeline of relevant dates and audit periods.
Audit
Based on our consensus meetings and the guidelines for outpatient management during the pandemic,2 3 the following audit standards were predefined:
Standard 1: All eligible ED trauma patients should be referred to the VFC, allowing the VFC team to review, triage and outline an extensive treatment plan for all patients.
Standard 2: After VFC review, all patients should be contacted to discuss their individual treatment plan.
Standard 3: If deemed possible by the VFC team, patient-initiated follow-up should be the default.
Standard 4: Follow-up appointments should be delivered by telephone or video if possible.
All ED patients diagnosed with a fracture were considered for the audit. Exclusion criteria were: simple stable injury discharged directly by the ED staff based on protocols that were in place prior to the pandemic (figure 1); acute admission; and follow-up in a different hospital.
The first audit was performed between April 6, 2020 and May 3, 2020 and the second audit between September 7, 2020 and October 4, 2020. To assess the extent to which our audit standards were met during both audit periods (ie, compliance), all patients presenting to our ED with a suspected fracture were reviewed daily.
Waiting times
Prior to the pandemic, that is, in January 2020 (figure 2), two researchers performed stopwatch waiting time measurements of ED patients with a suspected fracture, including measurements on four weekdays and 1 day in the weekend. Patients provided verbal consent on arrival. One patient was followed at a time. Per patient, the total ED waiting time and three subprocesses were recorded (online supplemental table S1). Timestamps of the subprocesses were: (1) time from entering the ED until the patient’s first contact with physician (time to review); (2) time from the patient’s first contact with a physician until the formulation of the final decision and the start of immobilization (time for review and decision-making); and (3) time from the start of immobilization until leaving the ED (time after review). These time measurements served as baseline.
Supplemental material
During both audit periods, time measurements were performed similarly (ie, on four weekdays and 1 day in the weekend, following one patient at a time). To assess the effects of implementing the VFC review and orthopedic trauma fast-track pathway on ED waiting time, we compared the waiting times of the first and second audits to the baseline measurements (ie, those conducted prior to the pandemic), respectively.
Additionally, per patient, the total time needed for VFC review, including contacting the patient by telephone afterwards, was measured during both audit periods.
Statistical analysis
Statistical analysis was performed using SPSS V.21. Descriptive statistics were used to assess compliance to our new workflow, and the extent to which our predefined audit standards were met. Waiting times were reported as median. Both audit periods were compared with the baseline measurements using the Mann-Whitney U test. A p value <0.05 was considered statistically significant.
Evaluation in-between audits
After the first audit, staff of all involved departments were invited to attend a meeting to evaluate the new workflow based on their experiences and the gathered data. This was used to define further optimizations of the workflow prior to the second audit.
Patient and public involvement
Patients were not involved in design, intervention, research question, or outcome measures.
Results
First audit: April 2020
In total, 184 patients with a fracture were eligible for VFC review during the first audit.
First standard: 162 of 184 eligible patients (compliance: 88.0%) were referred for VFC review by the ED staff. More information (eg, additional imaging) was needed in six patients (3.3%) before a treatment plan could be made.
Second standard: After VFC review, 19 of 162 patients (11.7%) could not be contacted immediately. Of these patients, 16 (9.9%) contacted the VFC team after being requested to do so via voice mail. The other three patients (1.9%) could not be reached. A letter was sent to the patient and their GP, requesting to contact the hospital.
Third standard: Of the 162 patients reviewed, the VFC team discharged 29 patients (17.9%, table 2).
Patients ‘virtually’ discharged after VFC review during first audit
Fourth standard: The treatment plans of all patients totaled 291 appointments, 137 (45.0%) of which to be conducted remotely.
Waiting time
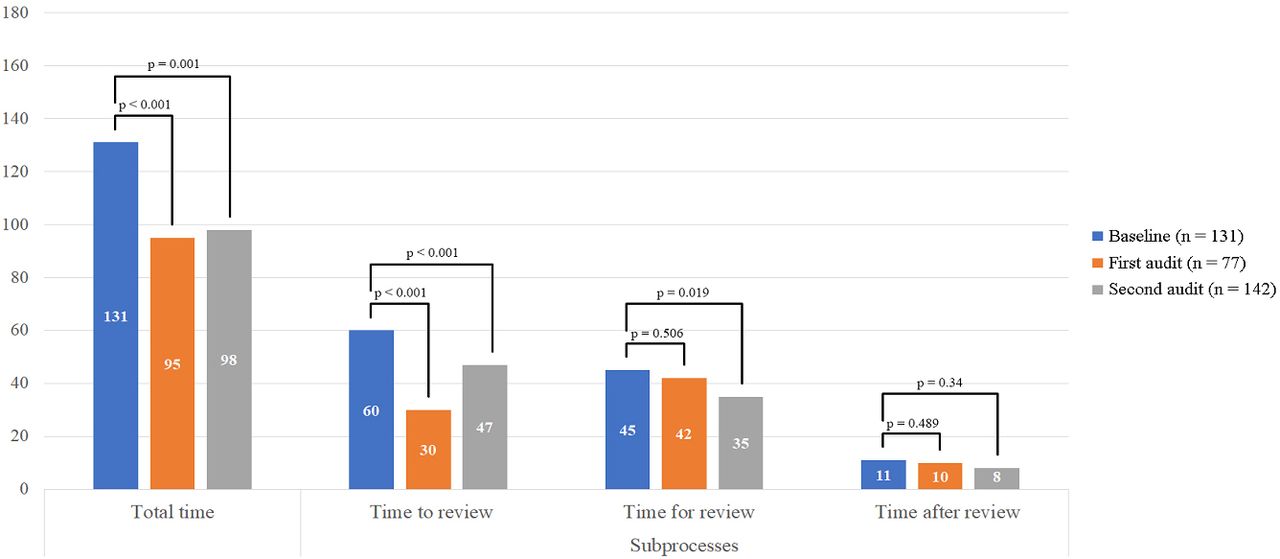
Of all patients presenting to our ED with a suspected fracture, 88% were treated in the fast-track rooms. Waiting time was measured in 77 patients during the first audit, and compared with baseline measurements performed in 131 patients prior to the pandemic. The median total time per patient from entering the ED until leaving the ED was 95 minutes during the audit, compared with 131 minutes in January (figure 3 and online supplemental table S2; p<0.001). Time to review was 30 minutes during the audit, compared with 60 minutes in January (p<0.001). Time for review was 42 minutes during the audit, and 45 minutes in January (p=0.506).
Supplemental material
{kind=link}
{kind=link}
{kind=link}
Median time spent in the emergency department (ED) in minutes during baseline, first audit and second audit period. Mann-Whitney U test was used to compare the first audit (April 2020, orange bars) and the second audit period (September 2020, gray bars) to baseline (January 2020, blue bars), respectively. A p value <0.05 was deemed statistically significant.
During the first audit, the median time needed for VFC review was 9 minutes per patient.
Optimizations after evaluation of first audit
ED staff were invited to be present during the VFC review if their time allowed. We expected this would improve the completeness of their documentation in the ED, as well as their compliance (eg, only 88% of eligible patients were referred for VFC review while the standard was 100%), as feedback could be provided directly. Furthermore, we expected the VFC workflow would postpone the often lengthy process of decision-making and supervision of orthopedic trauma patients in the ED. However, time for review and decision-making did not decrease. The ED staff noted it was not always clear if a case should be referred for VFC review, or discussed directly. Therefore, multiple presentations were held explaining the workflow, and posters depicting the workflow were provided in the ED. An information leaflet was developed and provided to the patient at discharge, which requested patients to contact the hospital if not contacted by 15:00 on the next workday.
Furthermore, we expected our time comparisons were biased by the low volume of patients in April 2020 (online supplemental figure S1). Therefore, we wanted to perform the second audit once the patient volume was more comparable to January 2020, hence also more representative of a non-COVID situation. We evaluated patient volume monthly and found patient volume in August 2020 to be comparable to 2019 (online supplemental figure S1). Therefore, the second audit started on September 7, 2020. To illustrate, in September 2019 there were 1123 trauma patients who presented to our ED with suspected injuries, compared with 1069 in September 2020 (online supplemental figure S1).
Supplemental material
Second audit: September 2020
In total, 305 patients with a fracture were eligible for VFC review during the second audit.
First standard: 302 of 305 (compliance: 98.4%) eligible patients were referred for VFC review by the ED staff. More information (eg, additional imaging) was needed in 11 patients (3.6%) before a definitive treatment plan could be made.
Second standard: After VFC review, 13 of 305 patients (4.3%) could not be contacted immediately. Of these patients, 10 (3.3%) contacted the VFC team after being requested to do so via voice mail. The other three patients (1.0%) could not be reached. A letter was sent to their GP, and to the patient requesting to contact the hospital.
Third standard: Of the 302 patients reviewed, the VFC team discharged 41 patients (13.6%, table 3).
Patients ‘virtually’ discharged after VFC review during second audit
Fourth standard: The treatment plans of all patients totaled 436 appointments, 179 of which (41.1%) to be conducted remotely.
Waiting time
Of all patients who presented to our ED with a suspected fracture during the second audit, 92% were treated in the fast-track rooms. Waiting time was measured in 142 patients during the second audit. Total time was 98 minutes per patient (−33 minutes, p=0.001 compared with January 2020). Time to review was 47 minutes (−13 minutes, p<0.001 compared with January 2020). Time for review was 35 minutes during the second audit, compared with 45 minutes in January (p=0.019).
During the second audit, the median time needed for VFC review was 7 minutes per patient.
Discussion
This study showed that once the new workflow had settled in, the implementation of a VFC review on workdays allowed the VFC team to review, triage and outline a treatment plan for 98.4% of ED orthopedic trauma patients. Prior to the implementation of the VFC review, all of these patients would have been referred for face-to-face review in our fracture clinic.2 Instead, the VFC team discharged 17.9% and 13.6% of these patients ‘virtually’, and therefore seems to have reduced the number of unnecessary face-to-face reviews of these patients during the first and second audits, respectively. Moreover, an extensive treatment plan was documented for all other patients, which is in line with national guidelines for the outpatient management of patients during the coronavirus pandemic.2 3 Hence, our study indicates that a VFC review can be established in 3 weeks with a relatively high level of compliance.
To our knowledge, this is the first study conducted outside the UK to describe the implementation and effects of a VFC review.9 According to the original UK VFC model, the VFC team either discharges patients ‘virtually’, or refers patients to a nurse-led clinic or subspecialty clinic for further treatment.4 5 The reviewing nurse or physician then decides on further follow-up during that subsequent clinic visit. However, we were of the opinion that such a set-up is prone to high levels of treatment variation. Furthermore, national guidelines for the outpatient treatment of patients during the pandemic required the necessity and mode (eg, face to face or remote) of each follow-up appointment to be evaluated by an attending physician. For these reasons, in addition to the original UK VFC model, our VFC review included the documentation of an extensive and complete treatment plan for each patient. To this end, we established special care pathways shortly after the coronavirus pandemic was declared, which were based on the principles in the national guidelines, that is, requiring minimized consultations and increased remote care during the pandemic.2 3
Previous studies have reported ‘virtual’ discharge rates ranging from 11.1% to 26.4%.4 5 Our virtual discharge rate was 17.9% and 13.6% during the first and second audits, respectively. Differences in these numbers across hospitals are most likely caused by a difference in the number of simple stable injuries that are discharged directly by ED staff,10 that is, the larger the number of injuries discharged directly from the ED, the smaller the number of injuries that can be discharged ‘virtually’ after VFC review. Furthermore, the extent to which removable immobilization is used in the ED also determines whether patients can be ‘virtually’ discharged or not. When revising our treatment protocols based on national guidelines, we did not make any changes to the immobilization materials used in the ED. Therefore, in the future, increased use of removable orthoses in the ED can further eliminate the need of cast removal, which in turn might allow even more patients to be discharged ‘virtually’ after VFC review.
For all these reasons, our VFC review supported the adherence to national guidelines for the outpatient treatment of patients during the coronavirus pandemic. To illustrate, we evaluated the necessity of each (face-to-face) appointment by documenting an extensive VFC treatment plan for each patient, and we minimized face-to-face review whenever possible through the VFC treatment plan as well as by ‘virtually’ discharging patients with minor injuries. Moreover, while not part of the current study, we assume that the documentation of an extensive treatment plan also reduces treatment variation and untimely or unnecessary appointments and imaging during further follow-up.
It is worth noting that, while numbers were low, a small proportion of patients could not be contacted after VFC review. Despite the safety netting that includes a discharge leaflet, voice mail and letter to the GP, one patient (clavicle fracture) had not contacted our hospital at all, a few weeks after the last VFC review in September 2020. It is also important to consider that the number of patients that cannot be reached after VFC review might be higher in other countries (ie, compared with the Netherlands or UK), particularly those with limited cellular phone saturation. If this would be the case, a possible solution would be to refer the patient to the fracture clinic for face-to-face review, while a VFC team would still document an extensive treatment plan for all patients on the first workday after the ED visit. This would eliminate the need for a telephone call after VFC review, while we expect that the documentation of an extensive treatment plan would then still reduce treatment variation and unnecessary appointments.
Another aim of the VFC review (ie, postponing decision-making to the next workday) and the orthopedic trauma fast-track pathway was to alleviate ED workload and minimize ED waiting time. We found that the total time spent by the patient in the ED was decreased by 36 and 33 minutes during the first and second audits, respectively, compared with baseline measurements performed before any changes were in effect. Time to review was reduced from 60 minutes (baseline) to 30 minutes during the first audit. Once patient volume was comparable during the second audit, this increased to 47 minutes. However, this is still a statistically significant median reduction of 13 minutes per patient compared with the baseline measurements.
Furthermore, during the second audit, the time spent by the ED physician for review and decision-making decreased by 10 minutes (from 45 to 35 minutes) compared with the baseline. The median time needed for VFC review on the next workday was 7 minutes per patient. Hence, the VFC pathway is time effective compared with direct supervision in the ED, with the benefit of an extensive treatment plan that is explained to the patient in detail. This also allows ED physicians to spend time on reviewing other patients or performing different tasks.
This study has several limitations. First, time measurements were performed during the COVID-19 pandemic. While we performed the second audit once patient volume normalized, it is unclear if the time effectiveness will be comparable to a non-COVID scenario. Second, this was a study focusing on the compliance to our new workflow and its effects on waiting time in the ED. Therefore, we did not study if the treatment plans were followed in the subsequent months, nor did we study patient outcome or experience. Last, workflow, treatment protocols or cellular phone usage might be different in other countries or even across hospitals within a country, and therefore generalizability of our results should be tested. We do expect, however, that the documentation of an extensive and tailored treatment plan for each individual patient shortly after the initial ED assessment is a generalizable concept that will improve care in most current settings.
Based on these first results, our hospital will continue to use and evaluate this new workflow. Future studies should assess the extent to which the VFC treatment plans are followed throughout the patient’s treatment, and whether the documentation of this extensive plan reduces treatment variation, as well as untimely and unnecessary follow-up appointments and imaging. Furthermore, studies should assess patient outcome and experience, ultimately providing evidence on the model’s (cost-)effectiveness.
In conclusion, this is the first study outside the UK to describe the use of the VFC model to streamline outpatient trauma care during the coronavirus pandemic. Without previous experience, the VFC was implemented with high compliance, despite being established in a quick response to national guidelines. The VFC allowed us to review, triage, and outline an extensive treatment plan using agreed-on care pathways for the majority of ED orthopedic trauma patients during the coronavirus pandemic, under direct supervision of the attending physician, while being time effective. This supported adherence to national guidelines for the outpatient treatment of patients during the coronavirus pandemic. We assume this process will also reduce treatment variation and will minimize unnecessary or untimely appointments and imaging, which is likely to also be of value in a postpandemic scenario. Future comparative studies, including follow-up of the patients reviewed, are needed to further assess this.
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request to the corresponding author. This includes deidentified data of the waiting time measurements.
Ethics statements
Patient consent for publication
Ethics approval
Ethics review was not sought because the study was deemed an improvement activity and not a human subjects research.
Acknowledgments
The authors would like to thank the following persons for their contributions to this article: Simone Augustinus, Leontien MG Nijland, Diederik HR Kempen, Michelle J van der Pols.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators Simone Augustinus; Leontien CW Nijland; Diederik HR Kempen; Michelle J van der Pols.
Contributors THG was responsible for the methodology, statistical analysis of the data, and the writing of the article. DAS was responsible for the methodology and writing of the article. KAdV was responsible for time measurements, methodology, statistical analysis of the data and draft of the article. PCWN was responsible for the development of the VFC review and implementation in the EPR, and the writing of this article. JMvD was responsible for the methodology, statistical analysis and writing of the article. RH, JCG and RNvV were responsible for the development of the VFC review, the methodology of this study and the writing of this article. RNvV was the guarantor of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.