Article Text

Abstract
Background The COVID-19 pandemic has had far-reaching effects on healthcare systems and society with resultant impact on trauma systems worldwide. This study evaluates the impact the pandemic has had in the Washington, DC Metropolitan Region as compared with similar months in 2019.
Design A retrospective multicenter study of all adult trauma centers in the Washington, DC region was conducted using trauma registry data between January 1, 2019 and May 31, 2020. March 1, 2020 through May 31, 2020 was defined as COVID-19, and January 1, 2019 through February 28, 2020 was defined as pre-COVID-19. Variables examined include number of trauma contacts, trauma admissions, mechanism of injury, Injury Severity Score, trauma center location (urban vs. suburban), and patient demographics.
Results There was a 22.4% decrease in the overall incidence of trauma during COVID-19 compared with a 3.4% increase in trauma during pre-COVID-19. Blunt mechanism of injury decreased significantly during COVID-19 (77.4% vs. 84.9%, p<0.001). There was no change in the specific mechanisms of fall from standing, blunt assault, and motor vehicle crash. The proportion of trauma evaluations for penetrating trauma increased significantly during COVID-19 (22.6% vs. 15.1%, p<0.001). Firearm-related and stabbing injury mechanisms both increased significantly during COVID-19 (11.8% vs. 6.8%, p<0.001; 9.2%, 6.9%, p=0.002, respectively).
Conclusions and relevance The overall incidence of trauma has decreased since the arrival of COVID-19. However, there has been a significant rise in penetrating trauma. Preparation for future pandemic response should include planning for an increase in trauma center resource utilization from penetrating trauma.
Level of evidence Epidemiological, level III.
- injury
- COVID-19
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The COVID-19 pandemic has had far-reaching effects on healthcare systems and society in general. Some of these changes, such as impact on hospital utilization and supply chain, are directly related to the impact of the virus, whereas others result from decisions made on individual, local, regional, national, and international levels in an effort to mitigate the extent of disease spread, loss of life, and economic damage.1 Understanding the consequences of these choices allows for better ability to adjust the allocation of limited resources, anticipate secondary effects, and prepare for similar future events.
The National Capital Region (NCR) consists of a shared labor market encompassing the District of Columbia (DC) and surrounding portions of central Maryland and northern Virginia.2 With 5.2 million people in 2019, the NCR contributes most of the population to the Washington-Arlington-Alexandria metropolitan area, which is the sixth largest metropolitan statistical area in the USA as designated by the Office of Management and Budget.3–5
The NCR contains four American College of Surgeons’ verified adult level 1 trauma centers. Within DC, these include: The George Washington University Hospital, MedStar Washington Hospital Center, and Howard University Hospital.6 The fourth level 1 trauma center, Inova Fairfax Hospital, is in a Virginia suburb of DC, approximately 15 miles from the center of the city. In addition, Suburban Hospital and the University of Maryland Capital Region-Prince George’s Hospital (PGH) are designated level 2 trauma centers that border DC in Maryland and are each approximately 10 miles from the center of the city. PGH is the second busiest trauma center in Maryland and treats a high proportion of patients with penetrating trauma.7
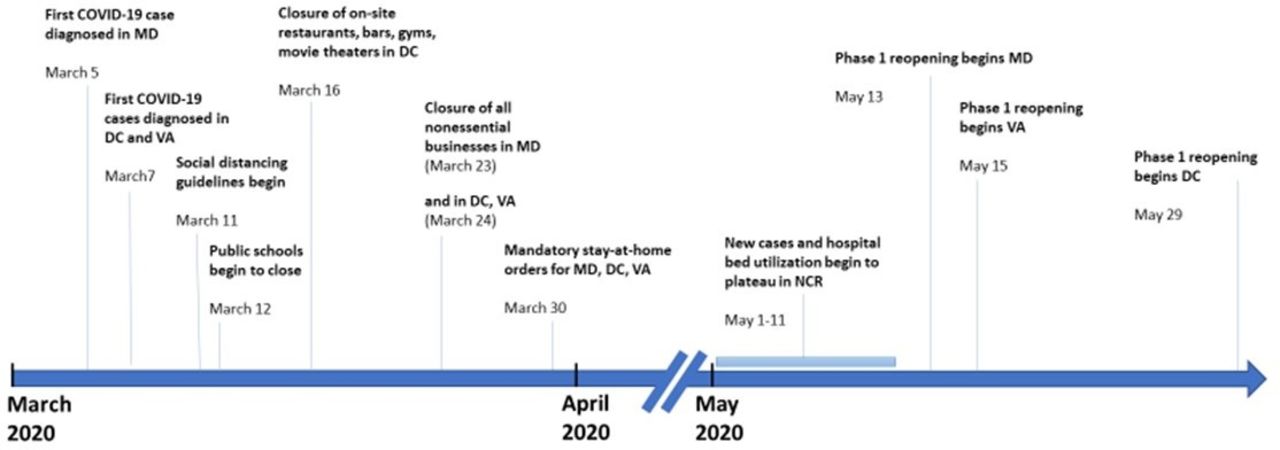
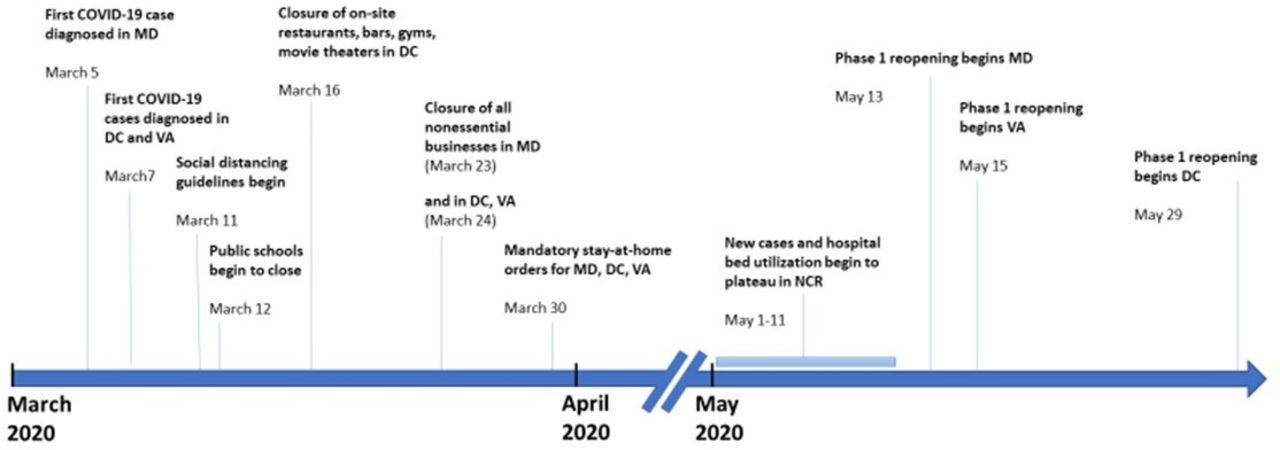
The COVID-19 pandemic reached the NCR in early March 2020, with the first case reported on March 5 (figure 1).8–10 Social distancing measures began to be introduced the second week of March 2020. Mandatory stay-at-home orders were announced in Maryland, Virginia, and DC on March 30, 2020.11–13 New cases of COVID-19 and hospital bed utilization started to reach a plateau in the NCR the first week of May 2020.14 15 The early COVID-19 period ended with the start of phase 1 reopening in DC on May 29.16–18
{kind=link}
Timeline of COVID-19 in the National Capital Region (NCR). DC, District of Columbia; MD, Maryland; VA, Virginia.
Early reports after onset of the COVID-19 pandemic from individual trauma centers around the world described a decrease in overall trauma volume after the declaration of stay-at-home orders.19–24 However, trauma centers in large cities across the USA also started to note an increase in the amount of penetrating trauma.25–30
This study investigates the temporal association between the COVID-19 pandemic and the epidemiology of trauma in the sixth largest metropolitan area in the USA from the approximate onset of local cases through early phase 1 of reopening. We hypothesize that COVID-19 19 is associated with a significant decrease in the overall incidence of trauma, but a concomitant increase in the rate of penetrating injury.
Methods
After obtaining individual Institutional Review Board approval or exemption from each institution and data use agreements among centers, amalgamated monthly data from January 1, 2019 to May 31, 2020 from the trauma registry of each of the trauma centers were entered into a REDCap database. The data were queried for number of trauma contacts, trauma admissions, admissions requiring top-tier activation, mechanism of injury (MOI), Injury Severity Score (ISS), and patient demographics. Additional information, such as trauma center verification level and location (urban or suburban), was collected. January and February 2020 were designated pre-COVID-19 whereas March through May 2020 was defined COVID-19. These months were compared with the corresponding times during 2019.
The George Washington University Hospital, MedStar Washington Hospital Center, Howard University Hospital, and the University of Maryland Capital Region-PGH were defined as urban trauma centers, and Inova Fairfax Hospital and Suburban Hospital were defined as suburban trauma centers. Information related to crime in Washington, DC was collected from the COVID-19 and Crime in the US Cities project of the University of Pennsylvania31 and from the Washington, DC Metropolitan Police Department.32
Pearson’s correlation coefficient analysis, r, was used to analyze trends over time for the overall incidence or MOI for trauma cases from our data set. McNemar’s test was implemented to compare proportional changes in trauma incidence by MOI stratified by pre-COVID-19 and COVID-19 months in 2020, and separately by the corresponding sets of months in 2019. These comparisons were analyzed for the overall sample as well as substratified to compare urban trauma centers to suburban trauma centers. SAS V.9.4 (SAS Institute) was used for data analysis and a two-sided p value <0.05 was considered statistically significant.
Results
The incidence of trauma in the NCR was increasing prior to the arrival of COVID-19 such that a total of 1900 patients were evaluated for trauma in January and February 2020 (pre-COVID-19) compared with 1837 patients in the corresponding months of 2019—a 3.4% increase in trauma volume. Trauma volume decreased significantly after the arrival of COVID-19 in that a total of 2559 patients were evaluated for trauma during COVID-19 as compared with 3299 patients evaluated for trauma in the corresponding period of 2019—a 22.4% decrease in trauma volume. There was no significant change in median patient age, which was 43.5 years old (IQR 28, 62.5) versus 41.5 years old (IQR 29, 61, p=0.83) in 2020. There was also no change in percentage of patients who were male (66% vs. 69%, p=0.48). The median ISS for both groups was 5 (IQR 1, 10).
Analyzing trends of absolute trauma incidence over time, we see that for pre-COVID-19, the trend for total trauma volume shows little to no effect size (r=−0.037) indicating steady trauma volume between January 2019 and February 2020. However, incorporating the COVID-19 months into the trend analysis shows a shift towards a moderate, negatively correlated trend between time and absolute trauma volume (r=−0.425). This indicates a sudden decrease in total trauma volume corresponding to the COVID-19 period. Similarly, trends of decreased blunt MOI volume were compounded after incorporating COVID-19 months (r=−0.553) relative to pre-COVID-19 (r=−0.131). Conversely, trends of increased penetrating MOI volume were amplified when including COVID-19 months (r=0.416) relative to pre-COVID-19 only (r=0.268). Specifically, COVID-19 months were associated with a large, positively correlated trend between time and both gunshot wound (GSW) and stab wound (SW) incidences (r=0.814 and r=0.921, respectively) relative to pre-COVID-19 (r=0.322 and r=0.300, respectively).
These findings are consistent with Washington, DC crime statistics. The incidence of violent crime in January and February 2019 as compared with 2020 was 3.8% and 4%, respectively. However, this incidence rose significantly, mostly due to an increase in firearm-related crimes, from 4.2% in March–May 2019 to 6.3% in March–May 2020. There was a similar significant change in proportion of trauma by MOI before and after COVID-19. The proportion of all-blunt MOI and specifically assault and motor vehicle collision (MVC) as well as the proportion of penetrating MOI and specifically GSW and SW did not significantly differ when comparing pre-COVID-19 to corresponding months in 2019 (table 1). In contrast, COVID-19 months relative to their 2019 counterparts showed a significant decrease in proportion of blunt MOI (77.4% vs. 84.9%, p<0.001) and a significant increase in proportion of penetrating MOI (22.6% vs. 15.1%, p<0.001). Specifically, the proportion of GSW increased approximately 75% (11.8% vs. 6.8%, p<0.001) and the proportion of SW increased approximately 33% (9.2% vs. 6.9%, p=0.002; table 1).
Mechanism of injury, pre-COVID-19 and COVID-19 compared with 2019*
Urban and suburban trauma center substratification comparing COVID-19 and analogous months in 2019 showed a significant decrease in proportion of blunt MOI and a significant increase in penetrating MOI for both the urban and suburban strata (table 2). The proportional decrease in blunt MOI and increase in penetrating MOI were greater in the urban cohort relative to the suburban cohort (7% vs. 5.7%). Furthermore, COVID-19 months were associated with an increase in GSW proportion specific to urban centers (13.8% vs. 8.3%, p<0.001) and an increase in SW proportion specific to suburban centers (8.1% vs. 4.3%, p<0.001) when compared with their 2019 counterparts (table 2).
Suburban vs. urban location: mechanism of injury, pre-COVID-19 and COVID-19 compared with 2019*
Discussion
The COVID-19 pandemic has changed the daily work and leisure routine for people throughout the world. This resulted in significant changes in the incidence of traumatic injury, with multiple regions reporting a substantial decrease in the incidence of trauma volume as social distancing and patterns of on-site work and in-person schooling changed.19–24
Regional strategies to mitigate the spread of COVID-19 as the pandemic reached the NCR included closure of schools to in-person education, closure of non-essential businesses, and issuance of stay-at-home orders. Collectively, this resulted in a marked decrease in vehicle and pedestrian traffic, gatherings both during the workday as well as after hours, and distancing of friends and families. Specifically, Apple Mobility Trends Reports demonstrates a precipitous drop in driving (approximately 55%), walking (approximately 60%), and transit (approximately 80%) in DC starting in early March and with a nadir in early April 2020.33 Similarly, Google Mobility Data, which provides information on mobility trends in different communities, identifies an approximately 70% drop for work and a 25% increase for at-home residence by April 2020 compared with a 5-week baseline period starting January 3, 2020 in DC.34 Our multicenter study found a 22.4% decrease in the regional trauma volume while these strategies were in place compared with the analogous period the previous year. This is more striking because trauma volume was rising with a 3.4% increase in incidence in the pre-COVID-19 period of 2020 relative to the same months of 2019. While the relative impact on specific injury mechanisms was not uniform, blunt trauma decreased during the regional height of the COVID-19 pandemic, while penetrating, and specifically firearm-related and stabbing trauma, increased. Urban locations saw a significant increase in gunshot injuries but not stabbings, whereas the opposite was true for suburban centers.
It is unlikely that our findings are explained by a more direct effect of the virus, such as a change in emergency medical service trauma referral patterns to centers outside the NCR. At no point during the study period did the region’s hospitals become overwhelmed, need to go on bypass, or alter their trauma triage criteria as a result of COVID-19.14 35 36 In addition, while it is possible that some patients chose not to seek medical care because of the pandemic, this study captures injuries of sufficient severity to necessitate evaluation in an emergency department. Patients admitted to the hospital due to injury would have been captured in the trauma registry.
Though many different injury mechanisms fall within the auspices of blunt trauma, we opted to evaluate three specific blunt mechanisms of injury which might be impacted the most by stay-at-home orders. Fall from standing is the most common MOI in the USA,37 with many of these events occurring at or near people’s residence or during recreational activities.38 Despite a potential increase in the number of hours people spent at home in the COVID-19 period, we did not find an increase in the incidence of injury related to this mechanism. Blunt force assault was examined as an index for non-firearm-related interpersonal domestic violence, which we thought might have increased due to stay-at-home orders and cohorting of people in the same residence. However, we did not find an increase in blunt assault during the COVID-19. Lastly, we examined MVCs as we anecdotally saw a large decrease in traffic volume in the NCR after issuance of stay-at-home orders. Although we did not find a statistically significant decrease in MVC-related injury during COVID-19 compared with the same months of 2019, there was a decrease in trend line for injury related to this mechanism (r=−0.246 vs. r=0.180) relative to January 2019 through the end of pre-COVID-19.
Shortly after the issuance of social distancing guidelines and/or mandates, trauma centers in some major cities began to report an increase in trauma due to a violent MOI, including firearm-related aggression.25–27 29 30 It is noteworthy that over 1 million more background checks for firearm sales were performed in March 2020 alone as compared with March 2019, and that this number does not include firearm transactions that occurred without a background check.39 Despite this, using publicly available police-recorded open crime data from eight cities in the USA, as compared with pre-COVID levels, Ashby found no significant change in the frequency of serious assaults, including aggravated assaults and homicides of all causes, during a similar time frame to our study.40 In contrast, Sutherland et al found a significant increase specifically in gun-related violence in three of four major US cities in 2020 compared with 2019, including two of the same cities (Baltimore and Los Angeles) evaluated by Ashby, when they analyzed police department and Federal Bureau of Investigation data.41 This could be related to the categorization of aggravated assault as violent crime in which a decrease in blunt assault would offset increases in firearm and stabbing violence.
Firearm-related trauma is particularly concerning in a resource-constrained environment that may be present during a pandemic. Despite a suspension of elective operations, the nation’s blood supply reached critical shortages during the March through May 2020 period.42 With a finite shelf lifespan, maintaining an appropriate blood product inventory depends on continuous collection from blood donors. Prior to the COVID-19 pandemic, approximately 80% of this occurred during blood drives, which had to be canceled because of social distancing requirements.43 44 Firearm-related injuries are frequently associated with hemorrhage and the need for transfusion.45 DeMario et al found that patients with GSWs were approximately five times more likely to require transfusion and received approximately 10 times more component units compared with non-ballistic injuries.46 The increase in firearm injuries identified in this study places additional stress on an already limited blood product inventory.
In addition, many health systems across the nation instituted substantial changes in staffing models to facilitate optimal management of patients with COVID-19, asking surgeons to assist in intensive care unit coverage. Depending on trauma center coverage models this could present significant challenges to select centers. Distribution of staff at trauma centers should consider potential increased demands related to penetrating trauma. Finally, proactive interventions to mitigate the pandemic-associated rise in stabbing and gun trauma should be considered.
This is the first regional and multicenter report on the impact that the COVID-19 pandemic has had on the incidence and nature of traumatic injury in a major metropolitan area in the USA. Although COVID-19 is the most prevalent pandemic seen since the influenza pandemic of 1918, there have been many recent instances of other viral outbreaks with the potential for widespread infection, and agencies such as the WHO regularly identify new potential threats. Therefore, we think the findings of this study are helpful in planning for future pandemic events, with the key finding being that overall trauma volume decreases significantly, but, in contrast to most reports from other Western countries, there may be a significant increase in stabbing and firearm-related injury in urban settings in the USA. Resource availability as part of planning for a pandemic should include supplies used with frequency in penetrating trauma, such as blood products or alternatives and equipment required for mitigation of infectious disease transmission. A comprehensive understanding of the regional variability of these findings is essential to any future pandemic preparation
This study has several limitations that we acknowledge. First, it is a retrospective study with all the limitations therein. Second, this study only captures data from the first 3 months of COVID-19 impact on the NCR; therefore, it is unclear how this will evolve over time. Third, other factors including year-to-year variability and seasonal variability could explain our findings, but we have tried to control for this by analyzing the same time periods in sequential years. Fourth, to maintain patient anonymity, we did not review data at the patient level. This precluded our ability to better characterize the nature of the injuries seen and/or exact treatments rendered. However, we were able to measure overall injury severity, which was unchanged, and the purpose of this article was to describe the incidence of injury and the types of injuries seen as opposed to outcomes obtained from specific treatments rendered. Lastly, this study does not include patients who either did not come to the hospital or went to a non-trauma center. However, that population most likely represents patients with lower acuity injury and thus does not alter the conclusions of this study regarding severe injury.
Conclusion
After the institution of guidelines and mandates to mitigate the spread of COVID-19 there was a significant decrease in the incidence of overall trauma, a marked decrease in the volume of blunt injury mechanism trauma, and a concomitant rise in the incidence of penetrating mechanism trauma in this multicenter region-wide study. This increase was particularly notable for stabbing and firearm injuries. We think this information is important for guiding continued efforts towards addressing the current pandemic and in preparing for potential future events.
Footnotes
Contributors Study design: MC, BS, AS, JE, ERH, EH. Data acquisition: BS, BB, SG, CPM, JC, EH, CTT, CA, ERH, MLK, MW, AZ, JE. Data analysis and interpretation: MC, BS, AS, BB, SG, CPM, EH, ERH, JE. Article draft and revision: MC, BS, AS, BB, SG, CPM, JC, EH, CTT, CA, ERH, EE, MLK, MW, AZ, JE.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Institutional Review Board of each institution.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.