Article Text

Abstract
Background Blunt thoracic aortic injury (BTAI) is an uncommon diagnosis, usually developing as a consequence of high-impact acceleration–deceleration mechanisms. Timely diagnosis may enable early resuscitation and reduction of shear forces, essential to prevent worsening of the injury prior to definitive management. Death is commonly due to haemorrhagic shock, but clinical features may be absent until sudden and massive haemorrhage.
Objectives The aim of this systematic review was to determine the proportion of patients with BTAI who present with unstable vital signs.
Methods Manuscripts were identified through a search of MEDLINE, EMBASE and the Cochrane Library databases, focusing on subject headings and keywords related to the aorta and trauma. Mechanisms of injury, haemodynamic status and mortality from the included manuscripts were reviewed. Meta-analysis of presenting haemodynamic status among a select group of similar papers was conducted.
Results Nineteen studies were included, with five selected for meta-analysis. Most reported cases of BTAI (80.0%–100%) were caused by road traffic incidents, with mortality consistently higher among initially unstable patients. There was statistically significant heterogeneity among the included studies (P<0.01). The pooled proportion of patients with haemodynamic instability in the setting of BTAI was 48.8% (95% CI 8.3 to 89.4).
Conclusions Normal vital signs do not rule out aortic injury. A high degree of clinical suspicion and liberal use of imaging is necessary to prevent missed or delayed diagnoses.
- aorta
- wounds and injuries
- blunt
- aortic rupture
- aortic aneurysm
- hypotension
Statistics from Altmetric.com
Introduction
Blunt thoracic aortic injury (BTAI) is an uncommon diagnosis, usually developing as a consequence of high-impact sudden deceleration mechanisms. Responsible for approximately 8000 deaths per year in the USA, it is the second leading cause of death behind traumatic brain injury (TBI) among blunt trauma patients.1 Many patients do not survive to reach hospital, with as many as 90% dying at the scene of the incident.2 About one-half of patients surviving to hospital die within 24 hours if untreated.3 Timely diagnosis in patients surviving to hospital may enable early resuscitation and prevent worsening of the injury, prior to definitive management.
It is recommended that CT of the chest with intravenous contrast is performed for the diagnosis of BTAI.4 However, whole-body CT (WBCT) for all blunt trauma patients remains controversial. Radiation exposure is a common concern with the risk of dying from radiation-induced cancer estimated to be 0.08% after one single WBCT in a 45-year-old patient.5 In many situations, clinicians rely on symptoms and signs to screen patients who should undergo thoracic CT after blunt trauma.6
Physiological vital signs are commonly used for prehospital and in-hospital triage. In the presence of normal vital signs and a non-specific clinical presentation after injury, clinicians may not consider BTAI as a differential diagnosis. Clinical signs of BTAI have been reported to be uncommon, with less than half of patients who survive to hospital having clinical signs or symptoms of aortic injury.7 8 Approximately a third to one-half of patients have minimal or no external signs of chest trauma.9–11
Trauma triage protocols continue to recognise a systolic blood pressure (SBP) of less than 90 mm Hg as a triage criteria for trauma centre need, presence of life-threatening injuries and, in some settings, a trigger for blood transfusion.12 13 The aim of this systematic review was to evaluate the capacity of initial haemodynamic stability (exposure) to rule out aortic injury (outcome) in a population of blunt trauma patients and to assess the impact of initial physiological status on outcomes. Specific focus was afforded to SBP as a primary measure of haemodynamic stability.
Methods
A systematic review of the literature was undertaken and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.14 A study protocol was developed according to these guidelines and registered with the International prospective register of systematic reviews (PROSPERO), an international prospective register of systematic reviews (available from http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42016037031).
Information sources
The authors searched for English language articles in MEDLINE (1990–16 February 2016), EMBASE (1990–16 February 2016) and the Cochrane library (1990–16 February 2016) using a combination of the following subject headings and keywords: ‘aorta,’ ‘trauma,’ ‘injury,’ ‘perforation’ and ‘rupture’ (online supplementary appendix 1). Clinical trials, observational studies and meta-analyses were accepted, while case series and case studies were excluded.
Supplementary material
Study selection
We selected studies of trauma patients with a final diagnosis of thoracic aortic injury resulting from blunt trauma. Studies were included if they described the proportion of patients in a stable/unstable haemodynamic condition (measurements taken in the prehospital phase or on arrival to the ED). Specific exclusion criteria were studies of young patients (age <10 years) and studies examining patients with penetrating aortic injuries, non-traumatic aortic injuries or abdominal aortic injuries. Two reviewers independently scanned titles and abstracts to select articles for full-text review. Disagreements regarding eligibility were resolved by consensus.
Data collection
We extracted data about number of patients, age, sex, inclusion/exclusion criteria, mechanism of injury, SBP, Injury Severity Scale (ISS), repair type and in-hospital mortality. Where reported, classification of injury was extracted as outlined by the Society for Vascular Surgery, which groups aortic tears into grade 1 (intimal tear), grade 2 (intramural haematoma), grade 3 (pseudoaneurysm) and grade 4 injuries (aortic transection).14
Analysis
The primary outcome measure was the proportion of patients that presented in a haemodynamically unstable condition. Haemodynamic status was assessed using the definition reported in the included studies. Where unadjusted data were available, patients with a SBP ≤90 mm Hg were considered unstable. A subgroup of studies that reported instability defined by SBP ≤90 mm Hg was selected for quantitative analysis. Statistical heterogeneity was assessed using the Q test and I2 statistic. In the setting of significant heterogeneity, the use of a random-effects model to calculate a pooled proportion was deemed appropriate. Further analysis involved assessment of mortality data, with specific attention paid to the influence of initial haemodynamic presentation and treatment choices. All analyses were carried out using Stata (StataCorp, College Station, Texas, USA). Bias assessment among individual observational studies was conducted using the Newcastle-Ottawa Scale (NOS). For cohort studies, the NOS assigns up to a maximum of nine points for the risk of bias in three domains: (1) selection of study groups (four points), (2) comparability of groups (two points) and (3) ascertainment of outcomes (three points).15
Results
Study identification and exclusions
Seventy potentially relevant articles were identified during the title and abstract screening process (figure 1). Thirty-nine papers were excluded for the following reasons: insufficient data on primary outcomes (16 articles); duplication of patients (11); population characteristics not meeting eligibility criteria (6); abstract only publication (6). The remaining 31 eligible papers reportedly collected data on the variables of interest. The authors of 12 of these papers were contacted for this information because data on haemodynamic stability were incomplete or absent in the published results. None of these papers were eventually included because either (1) the data were no longer in the author’s possession or (2) the author did not return correspondence. Of the 19 included papers, meta-analysis of outcomes was carried out for a group of five manuscripts that used the same definition of haemodynamic instability (SBP ≤90 mm Hg on arrival to hospital). Description of the included studies and patient population are reported in table 1.

Search and selection process. Search process and assessment of eligibility of manuscripts for qualitative synthesis and meta-analysis.
Study and population characteristics methodology and population characteristics for manuscripts included in qualitative synthesis
Mechanisms and injury severity
High velocity mechanisms were the predominant cause of BTAI in the included studies. Road traffic incidents (motor vehicle collisions, motor cycle collisions, bicycle crashes, pedestrians hit by motor vehicles) were responsible for between 80.0% and 100% of BTAI in the 14 studies that included quantitative mechanism of injury data.16 17 The next most common mechanisms were falls and crush injuries. Four papers described falls as occurring ‘from height’. Among the five studies that provided data on degree of BTAI, free rupture (grade 4 injury) was observed in 19%–49% of cases.18–20 The presence of BTAI was associated with a significant burden of injury overall, as demonstrated by mean unadjusted ISS in the 12 papers that included severity data (range 31–54).16 21
Mortality
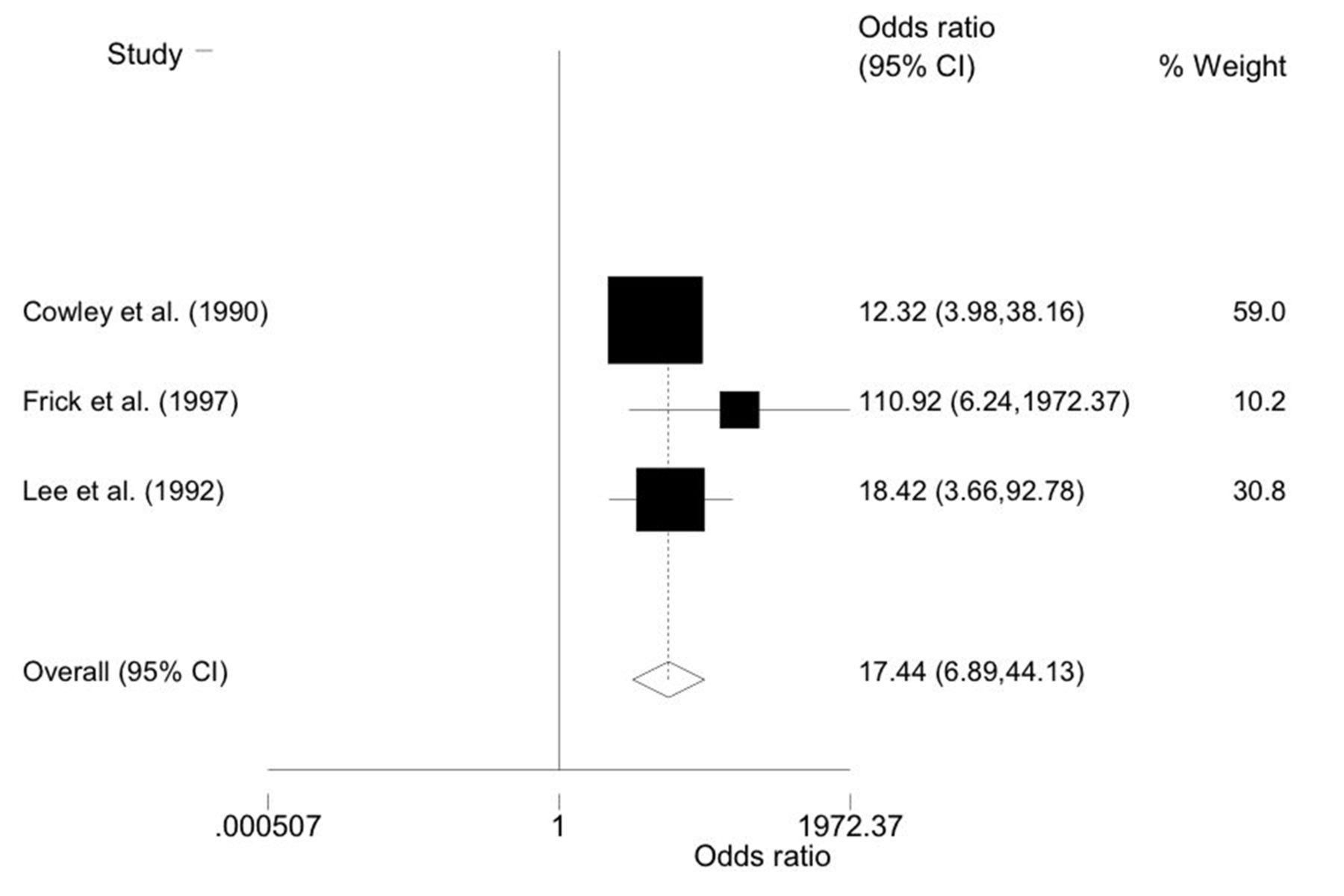
Among the five papers that underwent quantitative analysis, we observed a marked variation in reported mortality (range 14%–64%).21 22 There did not appear to be a correlation between mortality rates and proportion of patients with unstable vital signs (figure 2). The pooled ORs of death in unstable versus stable patients was 17.4 (95% CI 6.89 to 44.13) in the three studies that included mortality information for these subgroups (figure 3).21 23 24 An adjusted OR of 5.02 (3.65 to 7.34) was reported in the single study that accounted for possible confounders (table 2).25 Mortality was consistently greatest in patients who did not undergo repair of their aortic injury (range 65%–100%), with much lower rates among patients who underwent endovascular repair (range 7%–18%) and open surgical repair (range 19%–33%). Therefore, as compared with the remaining four studies, mortality was significantly lower in the single study that included only patients who underwent repair.22
Mortality in-hospital mortality, mortality by haemodynamic status, mortality by type of repair

Proportion of initially haemodynamically unstable patients and overall in-hospital mortality for manuscripts included in meta-analysis.
{kind=link}
{kind=link}
{kind=link}
Forest plot—odds of death in unstable (initial systolic blood pressure (SBP) ≤90 mm Hg) versus stable patients for manuscripts included in meta-analysis and overall pooled OR calculated by random-effects analysis.
Haemodynamic status
Various definitions of haemodynamic instability were presented. SBP was the most commonly used determinant of haemodynamic status. Aside from SBP, several other clinical criteria were used including intravenous fluid requirements, arrhythmia, tachycardia and signs of peripheral vascular shutdown. Most patients with BTAI were initially stable on presentation to hospital, with 12 of the 19 included studies reporting a proportion of unstable patients between 20% and 50%. There were five studies that defined haemodynamic instability based on SBP ≤90 mm Hg on arrival to hospital, which were selected for meta-analysis. Using the Newcastle-Ottawa Scale, only one of the five selected cohort studies was adjudged to have a low risk of bias in the determination of the impact of presenting haemodynamic status (exposure) on in-hospital mortality (outcome), with the other four manuscripts found to carry a moderate risk (table 3). Methods of recruitment and outcome assessment were considered appropriate, with points deducted in most cases for comparability of exposed and unexposed participants. Possible confounders were adjusted for in only one of the five studies, with a paucity of reported data demonstrating comparability between the two groups. Among these five manuscripts, the pooled proportion of patients with BTAI who had early haemodynamic instability as defined by initial SBP ≤90 mm Hg was calculated to be 48.8% (95% CI 8.3 to 89.4), using a random-effects model (figure 4). However, variation in the reported proportion of stable and unstable patients resulted in significant heterogeneity (χ2=912.38; P<0.01), reducing confidence in the calculated pooled proportion estimate. In all, 99.6% of variation in calculated incidence is attributable to differences in study characteristics (I2=99.6).
Assessment of bias using Newcastle-Ottawa quality assessment scale risk of bias in the determination of the impact of presenting haemodynamic status (exposure) on in-hospital mortality (outcome), based on selection of study groups (four points), comparability of groups (two points) and ascertainment of outcomes (three points)
- Download figure
- Open in new tab
- Download powerpoint
Forest plot—proportion of unstable patients (initial systolic blood pressure (SBP) ≤90 mm Hg) for manuscripts included in meta-analysis and overall pooled proportion calculated by random-effects analysis. ES, effect size.
Discussion
Haemodynamic instability in association with BTAI was detected in only about half of patients presenting with BTAI, with the majority of patients presenting with contained injuries (grades 1–3). This review adds to the existing pool of evidence suggesting liberal diagnostic imaging to identify BTAI based on the treating physician’s clinical suspicion, rather than specific clinical or physiological signs. However, confidence in this conclusion was limited by marked heterogeneity in sample sizes and the proportion of unstable patients included in the studies (range 16% to 91%).22 25
BTAI occurring in isolation is uncommon, with other serious associated injuries an important cause of clinical signs and possible haemodynamic instability in a proportion of patients. Therefore, haemodynamically unstable patients may have two distinct pathophysiological processes—patients with full-thickness tear of the aorta and patients with other sources of clinically significant haemorrhage from associated injuries to the chest or abdomen.26 It is the latter group that is more likely to be seen in hospital, though patients may present without haemodynamic instability at all if major associated injuries are not present. In haemodynamically stable patients, the hallmark of medical management is control of additional shearing forces to the aorta through heart rate and blood pressure control (including permissive hypotension). However, recognition of the aortic injury remains essential, and normotension may be falsely reassuring leading to delayed diagnosis. According to the Recommendations of the European Society of Cardiology Task Force on Aortic Dissection, control of blood pressure and contractility is of utmost importance in traumatic aortic dissection, regarded as a class 5 aortic dissection, to avoid progression to frank aortic rupture.27
Although a majority of papers reported a similar proportion of haemodynamically unstable patients, several major outliers were observed. At the lower end of the spectrum, the reported rate of haemodynamic instability was 4% in a 2010 study of 80 patients and 7% in a 2007 study of 28 patients.20 28 The first manuscript defined haemodynamic instability by a SBP <70 mm Hg, no doubt contributory to the remarkably low reported rate of unstable patients. The second manuscript reported a similarly low rate, despite using the more widely accepted cut-off of 90 mm Hg to determine haemodynamic status. Given only patients who underwent attempted repair were included in this report, the low reported rate of instability may be a consequence of the exclusion of unstable patients who expired early in their clinical course (before repair could be attempted).
Conversely, a 2009 analysis of the National Trauma Databank (NTD) found that 91% of 2402 patients were haemodynamically unstable.25 This high value was observed despite the use of a SBP cut-off of 90 mm Hg and the exclusion of 712 patients who were dead on arrival or who died during triage. Compared with the previous American major multicentre study of BTAI, a significantly greater proportion of patients with associated major head and abdominal injuries were observed in this cohort.22 This may have contributed to the higher rates of instability and overall mortality. Additionally, in contrast to previous multicentre collaborations, the NTD does not only include level I trauma centres. Level I centres receive a disproportionate number of patients transferred from distant locations, possibly introducing survival bias. Patients with BTAI resulting in haemodynamic instability may be seen less commonly at these centres if they do not survive long enough to travel such distances. The significantly higher rate of instability observed in the analysis of the NTD may therefore be a truer reflection of the clinical presentation of BTAI America wide.
Chart reviewers for the individual studies are unlikely to have been biased in their extraction of data on vital signs, given most of the articles had aims unrelated to the patients’ presenting clinical data. Eleven of the studies had treatment as the focus, four aimed to identify prognostic factors, one focused on imaging strategies, while four authors provided a general overview of the experience with BTAI at their institution(s). Only one paper had initial clinical presentation as its primary focus.29 While aims unconcerned with initial haemodynamic status may reduce risk of bias in data extraction, the lack of reported information comparing stable and unstable groups meant these groups could not be confidently deemed comparable across potential confounders. This introduces risk of bias in determining the impact of presenting haemodynamic status on in-hospital mortality.
The non-specific and often subtle clinical presentation of BTAI poses a major challenge to clinicians working within the ED. To improve assessment of risk for this injury, several clinical prediction rules have been put forward.30 31 Unfortunately, these rules remain incapable of ruling out the possibility of BTAI and have thus far failed to accurately stratify patients into clinically useful high-risk and low-risk categories.32 33 Mechanism of injury continues to be a critically important variable that should trigger further investigations, with the majority of patients injured following high-velocity road traffic incidents. Clinicians must be on high alert for the possibility of an underlying aortic injury in patients injured by such mechanisms, even in the presence of stable vital signs. The findings of this review highlight the significant overall injury burden observed in patients with BTAI. In addition to speeding up injury identification and reducing missed diagnoses, routine early use of WBCT among patients at risk of BTAI would enable early recognition of coexisting injuries. While mortality appears to be greater among unstable patients, the findings of our review demonstrate that stable patients should not be exempt from this practice, as early endovascular or open surgical management has been associated with favourable outcomes.34
A major perceived limitation of included studies was the definition of haemodynamic instability that used SBP ≤90 mm Hg as the only parameter for determining haemodynamic status. Current research inadequately addresses the complex matter of haemodynamic status among patients with BTAI, with a lack consistently reported data on other indicators of clinical status. A clinical diagnosis of haemodynamic instability usually encompasses a wide range of criteria, including, but not limited to, tachycardia, shock index, pallor and assessment of internal blood loss with tools such as ultrasonography.35 Our review demonstrates the inadequacy of SBP alone to identify patients suffering severe internal vascular injury. Further reaching parameters (such as those aforementioned) should be universally incorporated into future research in this area. A more rigorous assessment of stability may improve sensitivity of clinical tools to diagnose adult TAI.
A strength of this study is the comprehensive literature search that was undertaken and the assessment of eligibility and extraction of data by pairs of blinded reviewers. Most of the included studies were retrospective in nature and carried out at level I trauma centres using a combination of trauma registry data and chart review. While prospectively maintained trauma registry data can be considered good quality, retrospective chart review (used in 16 of the included studies) can be unreliable, especially if extraction of data is not systematic. Diversity in clinical and methodological aspects was significant, necessitating the selection of a subgroup of more similar studies for meta-analysis. Restricting our quantitative analysis to only a small proportion of the included studies, in this way, is a further limitation. Statistical heterogeneity was high, even among this subgroup. Despite observed heterogeneity, haemodynamic instability was often present in a significant portion of patients with BTAI. The analysis of associations between mortality and presenting haemodynamic status was limited by absence of details on cause of death in the included studies. While the deaths were associated with an aortic injury in all included patients, it is likely non-aortic injuries were the direct cause of death in a substantial proportion. With all limitations considered, hypotension, the predominant measure of instability observed in this review, appears to be insufficiently sensitive to rule out this injury.
Conclusions
Haemodynamic stability, as determined by SBP alone, cannot rule out blunt thoracic aortic injury in the adult trauma population. The use of other clinical variables in diagnosing BTAI remains unclear, with no known variables that can reliably diagnose or rule out aortic injury. At this stage, we recommend that CT with intravenous contrast should continue to be used liberally among patients where BTAI is possible.
References
Footnotes
Contributors All authors have made substantial contributions to the design of the study, drafting and revising the article, and final approval of the manuscript and its submission to the journal. Specifically, JB-B, BM and MCF planned the study; JB-B, JKM and BM designed the search strategy; JB-B and BM undertook the study selection process; JB-B undertook the data extraction process; JB-B, BM and MCF undertook the data analysis; BM provided statistical review; JB-B, JKM and BM articulated the discussion section; JB-B, JKM, MCF and BM revised the manuscript; JB-B submitted the study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.