Article Text

Abstract
Background Although non-operative management (NOM) has become the treatment of choice in hemodynamically normal patients with liver injuries, the optimal management of Organ Injury Scale (OIS) grades 4 and 5 injuries is still controversial. Oslo University Hospital Ulleval (OUHU) has since 2008 performed angiography only with signs of bleeding. Simultaneously, damage control resuscitation was implemented. Would these changes result in a decreased laparotomy rate and need for angioembolization (AE), as well as decreased mortality?
Methods We performed a retrospective study on all adult patients with liver injuries admitted at OUHU between 2002 and 2014. The total study population and patients with OIS grades 4 and 5 liver injuries underwent comparison between the periods before (P1) and after (P2) August 1, 2008.
Results 583 patients were included (P1: 237, P2: 346), with a median Injury Severity Score (ISS) of 29. The total population and the subgroup of OIS 4 and 5 injuries were comparable in age, gender, mechanism of injury, injury severity and physiology. Overall laparotomy rates decreased from P1 to P2 (35%–24%; p<0.01), as did the AE rate (11%–5%; p<0.01). The 30-day crude mortality decreased from 14% to 7% (p<0.05). A logistic regression model predicted an OR of 0.45 (95% CI 0.21 to 0.98) for dying when admitted in P2. In OIS grades 4 and 5 injuries (n=149, median ISS 34), similar reduction in AE rate was seen (30%–12%; p<0.05). The NOM rate for OIS grades 4 and 5 injuries was 70%, with 98% success rate. For the 30% requiring surgery, the mortality remained high (P1 52%; P2 40%), despite more balanced transfusion strategy.
Discussion Changes in resuscitation and treatment protocols were associated with decreased laparotomy, and AE rates as well as overall mortality. NOM is safe in 70% of patients with OIS grades 4 and 5 injuries, in contrast to the critically ill 30% requiring surgery who still have poor outcome.
Level of evidence IV.
- liver injury
- traumatic hemorrhage
- angiography
- transfusions
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Background
The treatment of liver injuries in adults has changed substantially during the last 50 years. In the 1980s the aggressive operative approach was challenged by a non-operative management (NOM) strategy associated with improved patient outcomes.1–3 The current treatment of blunt liver injuries is based on physiology with NOM as the standard in hemodynamically normal(ized) patients irrespective of injury grade.4 However, it is well recognized that a significant number of patients with severe liver injuries (American Association for the Surgery of Trauma Organ Injury Scale (OIS) grades 4 and 5)5 still require emergency surgery, and most reported overall mortality rates for these patients exceed 50%.6 7 The majority of these patients have multiple injuries, are physiologically compromised, and undergo aggressive fluid resuscitation.2 8 The contemporary initial resuscitation strategy of severely injured patients termed damage control resuscitation (DCR) includes early balanced use of blood products and restrictive use of crystalloids.9 10 DCR has been associated with reduced mortality and complication rates in the trauma population.2 11 12 It is important to underline that any comparison between published studies remains challenging due to lack of consistency with regard to inclusion and exclusion criteria.
In line with international trends, our initial treatment of severely injured patients has changed during the last 15 years, including improved multidisciplinary approach, updated protocols for interventional radiology, and DCR.13–15 We have previously shown that DCR was associated with improved outcome in patients with severe pelvic injuries, including reduced need for operative interventions and angioembolization (AE).16
The aim of the present study was to describe the treatment and outcomes in patients with liver injuries during a 13-year period. Based on the changes in treatment strategies during the study period, a further exploration of high-grade injuries, the need for and type of operative intervention, as well as the use of AE was performed.
Methods
Oslo University Hospital Ulleval (OUHU) is a major Scandinavian trauma center with a catchment area of more than 2.8 million people, covering the south-eastern part of Norway. The number of admissions has increased gradually with almost 1700 trauma team activations in 2014 vs 650 in 2002. Approximately 90% are blunt trauma and one-third are severely injured, with an Injury Severity Score (ISS) higher than 15.
All adult patients (18 years old or older) with a liver injury admitted between January 2002 and December 2014 were identified from the institutional trauma registry and included in the study. Patients who were deemed dead on arrival (DOA) and patients who underwent laparotomy before transfer to our institution were excluded. Patients injured more than 24 hours before admission were excluded unless the trauma team was activated.
Demographic data obtained from the hospital-based trauma registry included age, gender, mechanism of injury, time of injury, arrival time at the emergency department (ED), admission systolic blood pressure (SBP), heart rate (HR), base deficit (BD), Glasgow Coma Scale (GCS) score, ISS, transfusions prior to intensive care unit admission, Trauma and Injury Severity Score probability of survival17 with the National Trauma Data Bank (NTDB) 2005 coefficients, 30-day survival, and main cause of death. The main cause of death was determined as the most probable condition resulting in death after reviewing all available sources of information—patient charts, radiological imaging, and autopsy reports. Survival status 30 days after injury was collected from patient records and the Norwegian Population Registry. Liver injury was graded according to the OIS grading system based on operative and/or radiology reports and reviewed by two of the authors. Anatomic injury was classified according to the Abbreviated Injury Scale (AIS) 1998 version.18 Additional data on blood transfusions received during the first 24 hours after admission were extracted from the OUHU blood bank. Data on liver-related angiographic procedures and surgical interventions were extracted from the patient electronic records. Due to improvements in patient documentation during the study period, complications could only be reliably identified in a retrospective fashion for the later part of the study, and were thus not included in the analysis.
Until August 2008 our algorithm for treatment of liver injuries mandated angiography as part of NOM in all grades 3 to 5 injuries. Based on our previously published results and other reports, the protocol was adjusted to include selective angiography only when clinical signs of bleeding or significant contrast extravasation were identified on CT scan.19–21 At that time DCR was already implemented in our institution with an updated local massive hemorrhage protocol (MHP) from 2007. We therefore analyzed the study population for differences between January 1, 2002 to July 31, 2008 (period 1, P1) and August 1, 2008 to December 31, 2014 (period 2, P2). Patients with severe liver injuries defined as OIS grades 4 and 5 were identified and subjected to subgroup analysis.
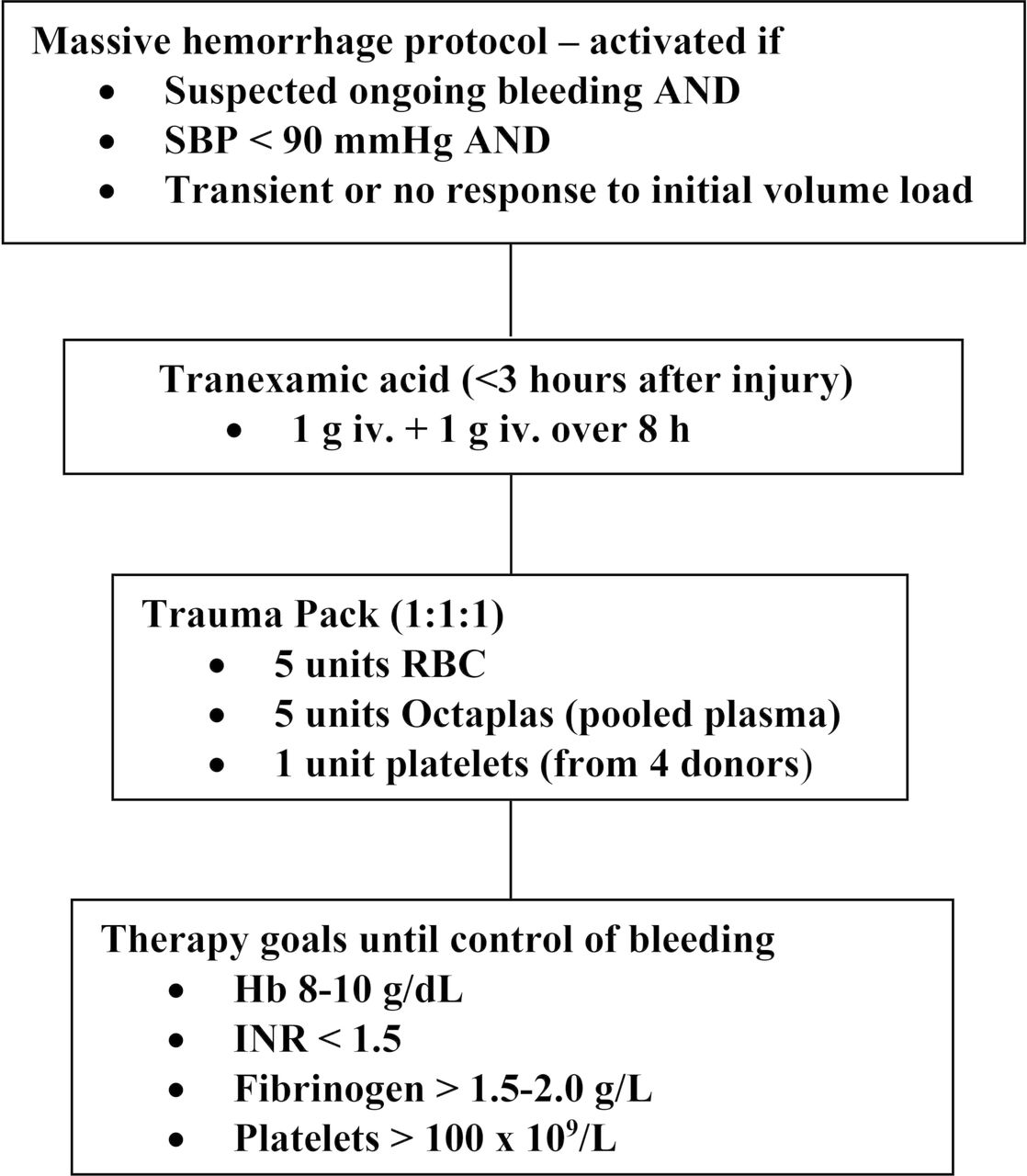
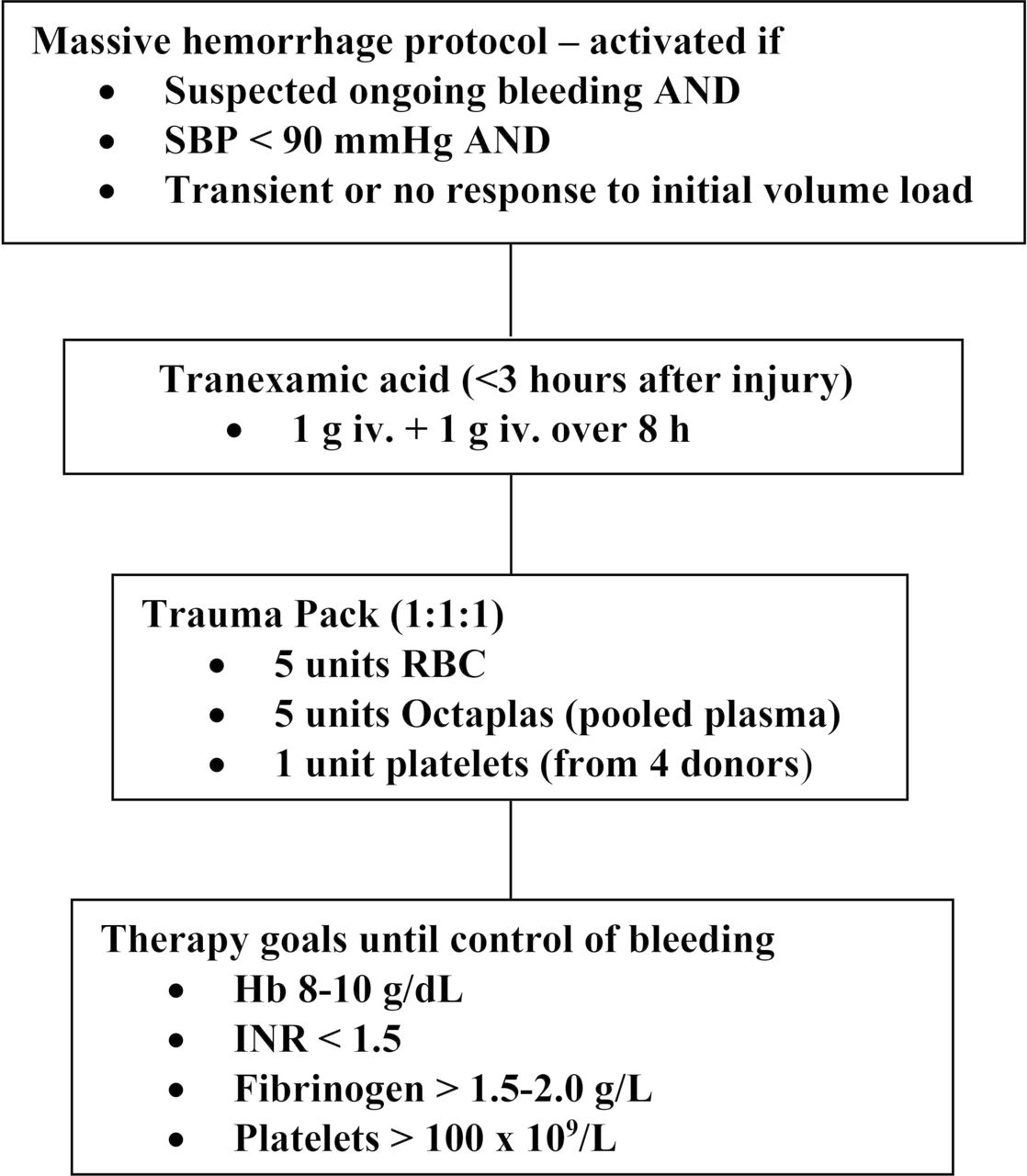
Throughout the study period, all patients with liver injury were managed according to our institutional protocol (figure 1), applying damage control principles as needed. Any patient with identified or suspected intra-abdominal hemorrhage and persistent hemodynamic instability despite adequate resuscitation would be subject to a damage control strategy. In P1, hypovolemic shock was addressed with aggressive fluid resuscitation consisting of crystalloids, colloids and red blood cells (RBCs). In P2, DCR with our updated MHP was initiated in patients with suspected ongoing bleeding, SBP <90 mm Hg, and inadequate response to resuscitation (figure 2). The MHP provides plasma, platelets, and RBCs in a 1:1:1 ratio, with adjustments guided by arterial blood gases, physiologic response to resuscitation measures, and change in conventional coagulation parameters.16

Management algorithm for patients with liver injuries. ED, emergency department; FAST, focused assessment with sonography for trauma; ICU, intensive care unit.
{kind=link}
{kind=link}
Basic massive hemorrhage protocol. Hb, hemoglobin; INR, international normalized ratio; RBC, red blood cells; SBP, systolic blood pressure.
According to the institutional protocol, irrespective of liver injury grade, the indications for laparotomy are hemodynamically unstable patients with inadequate response to resuscitation with suspected intra-abdominal bleeding, peritonitis, or CT evidence of other injuries requiring laparotomy. The surgical approach to liver injuries with ongoing bleeding has remained unchanged during the study period, with goal-directed packing as the procedure of choice when effective. Despite allowing a selective NOM approach during the past decade to hemodynamically stable patients with penetrating isolated liver injuries, most penetrating abdominal traumas undergo operative exploration in our institution. Our treatment algorithm, including indications for laparotomy and AE as part of a damage control strategy, has been described in a previous publication.19 Angiographic procedures were performed by interventional radiologists, who were available 24/7 with a response time of 30 minutes.
Statistical analysis
Continuous data are presented as median with IQR. Comparisons between groups are performed using the Mann-Whitney U test. Categorical data are reported as proportions and tested for significance using Pearson’s χ2 test and Fisher’s exact test as appropriate. For all analyses, a p value <0.05 derived from a two-tailed test was considered statistically significant.
A forward stepwise selection of significant covariates including potential confounders was performed to identify variables independently associated with 30-day mortality in patients with liver injury. These core variables were then applied to construct a multiple logistic regression model evaluating mortality. All variables were prespecified and considered clinically important. The fit of the models was measured with the Hosmer-Lemeshow goodness-of-fit test statistic. Calculation of the accuracy of the test was measured by the area under the receiver operating characteristic curve for the prediction of 30-day mortality. All statistical analyses were performed using the IBM SPSS Statistics V.24.0 for Windows.
Results
During the 13-year study period, 635 patients were diagnosed with liver injury. Twenty-seven patients deemed DOA and 25 patients who had undergone laparotomy before transfer to our institution were excluded from the study. Hence, the study cohort consists of 583 patients. The median age was 33 years (IQR, 23–50), the mechanism of injury was blunt in 90%, and 65% were men.
P1 compared with P2 for the total study population
P1 included 237 patients and P2 included 346 patients. The two periods are compared in table 1. When comparing baseline data, patients included in P2 were older with a higher median GCS score and HR than P1, otherwise there were no significant differences between the groups, including the proportions of patients admitted with hypotension (SBP <90 mm Hg) (18% in P1 and 19% in P2; p=0.713). The rate of AIS head grade ≥4 showed no statistical difference between the periods (14% in P1 and 18% in P2; p=0.253).
Comparison between periods for the total study population
The proportion of patients selected for NOM increased from 65% in P1 to 76% in P2 (p=0.003) without increased NOM failure rate (1% vs 1%; p=0.883). Penetrating injury was the mechanism in 10% of the patients, with 1 patient (4%) treated non-operatively in P1 and 11 (32%) in P2. Of those undergoing operative management (OM), the proportion of patients who had liver-related operative procedures performed remained unchanged (67% vs 61%; p=0.419). Death from liver-related hemorrhage in patients who underwent OM was 8% (7 of 83) in P1 and 4% (3 of 82) in P2 (p=0.203). The proportion of patients undergoing angiography decreased in P2 (31%–9%; p<0.001) with a concomitant reduction in AE (11%–5%; p=0.002). There was a decrease in overall 30-day mortality in P2 from 14% to 7% (p=0.015) and hemorrhage-related deaths decreased from 8% to 3% (p=0.003) (table 1).
Subgroup analysis for OIS grades 4 and 5 liver injuries
Table 2 shows the baseline characteristics and outcomes of patients from both periods with liver injuries OIS grades 4 and 5. The groups were comparable physiologically. The proportion of patients with a grade 5 injury exceeded 20% in both periods. Patients in P2 received significantly more plasma during the first 24 hours after admission (median 13 units vs 4 units in P1; p<0.001), with a resulting more balanced plasma to RBC ratio (median 1.04 vs 0.39; p<0.001). In P2 patients with severe liver injuries who received blood products were administered significantly lower volumes of crystalloid (5.0 L vs 1.7 L; p<0.001). There was no difference in NOM rate (68% vs 70%; p=0.860) or failures of NOM (4% vs 0%; p=0.195) between the periods. Not surprisingly, all penetrating OIS grades 4 and 5 injuries underwent laparotomy, one in P1 and four in P2. The rates of angiography and AE decreased from 68% to 22% (p<0.001) and from 30% to 12% (p=0.006), respectively.
Comparison between periods for patients with liver injuries OIS grades 4 and 5
As expected, patients with OIS grades 4 and 5 injuries who underwent laparotomy were severely physiologically compromised compared with patients treated non-operatively, with a 46% mortality rate of which 67% were hemorrhage-related (table 3). The two fatalities in the NOM group were due to traumatic brain injury.
Comparison of NOM and OM patients with liver OIS grades 4 and 5 injuries
Table 4 compares the two periods for patients with OIS grades 4 and 5 injuries who underwent laparotomy. Patients in P2 received significantly more plasma (median 17 units vs 5 units in P1; p=0.001), a more balanced plasma to RBC ratio (0.96 vs 0.22; p<0.001) and less volumes of crystalloid (2.0 vs 7.0; p=0.001) during the first 24 hours after admission. There was no difference in overall mortality and only a trend towards reduced mortality from bleeding in P2.
Comparison between periods for operated patients with liver injuries OIS grades 4 and 5
Multiple regression model
A multiple regression model predicting overall 30-day mortality in liver injuries was constructed in stepwise fashion to determine the clinically relevant and significant core variables. The variables selected for univariate analysis were the period, age, BD, GCS score, ISS, OIS liver, and laparotomy. Table 5 presents the crude and adjusted odds ratios, identifying P1, age, GCS score, ISS, and laparotomy to be independently correlated with increased 30-day mortality. In fact, the logistic regression model predicted an OR of 0.45 (95% CI 0.21 to 0.98) for dying when admitted in P2. The area under the curve for the score in the test data set was 0.92 (95% CI 0.88 to 0.96; p<0.001). The Hosmer-Lemeshow test statistic for model fit was acceptable (χ2=8.93, df=8, p=0.348).
Univariate and multiple logistic regression models for predicting 30-day mortality in patients with liver injuries
Discussion
We have shown that multiple general improvements in the treatment of severely injured patients, including contemporary resuscitation strategies, have improved overall results, whereas outcome in physiologically deranged patients with grades 4 and 5 injuries has not changed.
During the past two decades, the care of patients with liver injuries has dramatically changed from operative to non-operative management, with a review from the NTDB in 2008 demonstrating that only 14.8% of hepatic injuries are managed operatively.22 On that background, our reported decrease in OM from 35% to 24% during the 13-year study period might seem unsatisfactory. However, existing publications tend to vary concerning the study population characteristics, with some treating isolated liver injuries, some including penetrating injuries, and some restricting inclusion to patients surviving a certain number of hours after admission.3 22–24 In our institution, although allowing selective NOM for hemodynamically stable patients with penetrating liver injuries, the vast majority of patients with penetrating abdominal trauma undergo laparotomy. We chose to include penetrating injuries in the current analysis. With increased use of NOM, the risk of increased failures of NOM has been a matter of concern, and the possible overuse of NOM has been discussed.3 25 The overall NOM failure rate (1%) was unchanged during the study period and low compared with recent reports.25 26
There is no consensus on appropriate patient selection criteria for the patients with liver injuries who would benefit from angiography and AE.27 However, most recent reports seem to agree on some situations where angiography and AE are indicated: Patients with significant contrast extravasation in the liver on CT scan should undergo angiography.7 27–29 In patients with liver injuries taken directly to laparotomy without imaging, angiography is indicated directly after surgery if the patients show clinical signs of ongoing bleeding, or after early postoperative CT scan with contrast extravasation. Since 2008 our treatment algorithm for patients with liver injury has mandated selective angiography only in patients with signs of bleeding in accordance with the above-mentioned criteria, leading to a significant reduction in the use of angiography and AE (table 1). Unnecessary interventional radiology procedures should be avoided since the treatment modality is not without associated morbidity.27
The increased rate of NOM and reduced use of interventional radiology were associated with a reduction in crude total and hemorrhage-related mortality in P2 from 14% to 7% and from 8% to 3%, respectively. This is in accordance with one of very few recently published studies on overall mortality rate for liver injuries.23
A multiple regression model for the whole study population predicted an OR of 0.45 (95% CI 0.21 to 0.98) for dying when admitted in P2. Four other factors in the multiple regression analysis were significant for predicting overall 30-day mortality: age, GCS score, ISS, and laparotomy. Although GCS score can be influenced by hypovolemia due to hemorrhage, the most frequent cause of low GCS score is severe brain injury. As expected, higher ISS is independently associated with increased mortality caused by the severity of the injuries. Undergoing laparotomy increased the risk of mortality by an adjusted OR of 5.39. This is hardly surprising as the group of patients undergoing laparotomy are more severely injured and physiologically compromised than patients treated non-operatively.
In patients with OIS grades 4 and 5 liver injuries, earlier studies reported NOM to be successful in approximately 50%, with survival rates from 60% to 80%.2 6 8 30 Compared with these studies our results seem fairly acceptable with a NOM rate of approximately 70% and a survival rate of approximately 85% throughout the study period (table 2). However, direct comparisons between different studies should always be undertaken with caution due to differences in patient inclusion and exclusion criteria. Polanco et al 3 presented NTDB data on 3.337 patients with isolated severe blunt liver injuries and reported attempted NOM in 73% of patients with a failure rate of 7%. The rate of attempted and failed NOM increased during the 7-year-long study period. Shrestha et al 2 reported an increase from 54% to 74% in successful NOM of OIS grades 4 and 5 liver injuries after implementation of DCR. Moreover, the DCR treatment was associated with improved survival from 73% to 94%. The observed high survival rate compared with our results, 68% in P1 vs 70% in P2 despite a more balanced plasma to RBC ratio in P2 (1.04 vs 0.39), can be partly explained by the fact that patients who died in the ED were excluded in the study by Shrestha et al. 2
Despite increased focus on NOM, a subgroup of patients with severe liver injuries will still need surgical treatment facing a significant risk of fatal outcome. Patients with OIS grades 4 and 5 injuries who underwent laparotomy were much sicker and had a dramatically worse outcome compared with patients treated non-operatively (table 3). The mortality in the operative cohort was identical to the reported rate of 46% in patients with hypotension undergoing trauma laparotomy presented in a recent multicenter study by Harvin et al.31 In their study liver-related and spleen-related procedures were the most often performed and exsanguination was the cause of death in 60%. Despite a more balanced transfusion practice in P2 in our study, the mortality in the group of patients with severe liver injuries undergoing laparotomy was unchanged throughout the study period, with 67% attributable to bleeding (table 4).
This study has several limitations, in addition to those associated with its retrospective nature. In the subgroup of severe liver injuries, the limited number of patients means that the statistical power to identify a change is low. Furthermore, many of the institutional changes adapted during the 13 years are not quantifiable. Identifying complications retrospectively remains challenging. With improvements in patient documentation during the study period, complications proved to be too difficult to identify in a retrospective fashion for the early part of the study period, making comparisons unreliable.
Conclusion
In this retrospective single-center study on patients with liver injuries, we found decreased laparotomy, angiography, and AE rates, as well as overall and hemorrhage-related mortality, compared with historic controls. With improved treatment protocols including DCR strategies, NOM is safe in 70% of patients with OIS grades 4 and 5 liver injuries with normal(ized) physiology, with low failure rates and mortality, in contrast to the critically ill 30% who still need surgery and in whom future studies are warranted to improve outcome.
References
Footnotes
Contributors IAG, PAN, and CG designed the study and conducted the literature search. IAG, TE, TK, PAN, and CG collected the data. IAG, PAN, and CG analyzed the data. All authors interpreted the data, and participated in writing, revising, and editing the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Approval for the study was obtained from the Institutional Data Protection Officer at Oslo University Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.