Article Text

Abstract
Background Peer-reviewed publication plays important roles in disseminating research findings, developing generalisable knowledge and garnering recognition for authors and institutions. Nonetheless, many bemoan the whole manuscript writing process, intimidated by the arbitrary and somewhat opaque conventions.
Methods This paper offers practical advice about organising and writing a manuscript reporting quality improvement or patient safety research for submission to a peer-reviewed journal.
Results Each section of the paper discusses a specific manuscript component—from title, abstract and each section of the manuscript body, through to reference list and tables and figures—explaining key principles, offering content organisation tips and providing an example of how this section may read. The paper also offers a checklist of common mistakes to avoid in a manuscript.
- Quality improvement
- Patient safety
- Continuing education, continuing professional development
Statistics from Altmetric.com
Peer-reviewed publication plays important roles in disseminating research findings, producing generalisable knowledge and garnering recognition for authors and institutions. Yet, writing is rarely taught in medical school. In a 1985 survey, only 11 of 100 American medical schools offered some type of composition course for biomedical research papers.1 Pierson2 studied manuscript rejections and found that one of the major reasons was poor preparation (eg, over interpretation of results, text difficult to follow).
Many healthcare professionals have trouble organising and writing a research manuscript. One editor-in-chief described it this way: ‘Their scholarly and creative ideas and insightful data interpretation often seem to get lost in the translation from brain to page.’3 This quote begins the foreword for the AMA Manual of Style, which is a comprehensive guide to writing and publishing biomedical research.4 While a useful manual, it does not discuss the nuances of reporting quality improvement and patient safety research.
Published guidelines are available to improve the reporting of quality improvement and other health services–related research.5 The Standards for QUality Improvement Reporting Excellence (SQUIRE) guidelines offer an informative checklist when describing quality improvement studies, which often have interventions that evolve over time and are context-dependent.6
Whether clinical or quality improvement, research is conducted to observe or explain something unknown or to evaluate an intervention's impact on an outcome.7 Observational studies ask questions and generate hypotheses, while evaluation studies test hypotheses. Randomised clinical trials generally evaluate one therapy's impact on one outcome, sometimes comparing to a placebo or an alternative therapy, most often controlling all other care. Quality improvement is messier because it involves changing human behaviour in practice, testing and evolving interventions over time, developing theories that explain how the intervention relates to improved outcomes, incorporating how local context influences implementation and, often, evaluating performance.
The SQUIRE guidelines help authors untangle the mess of quality improvement work. Nonetheless, we repeatedly hear colleagues and mentees bemoaning the whole manuscript writing process. They have trouble determining what to include and how to frame their paper, seeking practical guidance and heuristics. This paper offers practical advice about organising and writing a manuscript reporting quality improvement or patient safety research for submission to a peer-reviewed journal.
Planning a manuscript
The four phases of a manuscript include planning, writing, submitting and revising. We cover the first two phases. A recent article nicely lays out the last phase, revising your manuscript following peer-review comments.8 This section is important, please read it carefully.
In the planning phase, define your audience and choose an appropriate journal. Understanding your audience will guide the level of detail you provide (eg, definitions for terminology). Look at the journal's scope and article categories to ensure your research fits. Once you have chosen a journal, read the author instructions for the word limit, specific formatting instructions, and required content and forms (eg, disclosing competing interests). Also, draft the order of authorship, complete a literature search related to your research topic, assemble tables and figures of your data and outline your paper.
Outlining can help organise your thoughts and manuscript content, offering a double check for complete and consistent information. For instance, if you describe a survey of laboratory technicians and nurses in the methods, report the response rates by job category and the survey data in the results. Head your outline with a thesis statement to avoid scope creep and remain focused on the paper's main message.
Writing a manuscript
Writing the first draft of your manuscript is different from writing a novel, in which you start at the beginning and proceed to the end. A research paper has distinct sections (abstract, introduction, methods, results, discussion) that fit together like a jigsaw puzzle to tell your story. Write each section separately.
We can recommend several strategies to make the writing process less onerous. You can write the sections in the following order: methods, results, introduction, discussion and finish with the abstract. Alternatively, write the abstract and create the tables and figures first, write the methods and results together next, then write the discussion and finish with the introduction. You could also write the methods during the planning and implementing phases of the study. Writing your paper concurrently with the work is invaluable because it helps produce a more accurate account of what occurred and clarifies what needs to be done. This strategy may also help you catch omissions or limitations early in the implementation phase when they are more easily remediable. Another strategy is to write your results concurrently with the assembly of each table and figure, or write the methods, results and important conclusions with each table or figure. You should select a strategy that works for you. Several books on academic writing may also be helpful references.9–12 When writing your paper, think of your main message in terms of a newspaper headline and use the manuscript to narrate that message.
We have organised our manuscript into six distinct parts: title, abstract, body, reference list, tables and figures, and acknowledgements.
Title and abstract
The title and abstract are prominent parts of a manuscript. Both sections are the first, and in some cases, the only content the editor and journal readers will peruse. Your title should grab the readers’ attention, like a news headline, while providing an informative description of the study. Try to mention the intervention, setting, patient population, outcome measure and study design. For example, ‘Patient information sheet improves inpatient care during Radiology testing.’ Notice that this title is concise and is not a wordy sentence.
The abstract is a snapshot of your study and should inform and persuade the editor and audience to read the full manuscript. Content that will clearly illustrate your study includes the objective, study design, population, setting, intervention, primary outcome measure and the method of analysis, important findings and brief conclusion. Before you draft the abstract, read the author instructions and follow their structure and word length. Avoid abbreviations unless it is a unit of measure (eg, mg for milligram) and exclude references.
Your abstract must make sense and not read as random content grabbed from your manuscript and plunked into subheadings. For example, if you report that ‘92% of radiology technicians perceived the patient information sheet was useful’ in the results, then describe the mechanism of data collection (eg, survey, interviews) and sample size in the methods. Read some published abstracts to guide your writing. Whether you write the abstract before or after the main body of your manuscript is a matter of preference. If you write it first, remember to revise it when the manuscript is complete to ensure consistency of content. As a general composition rule, write in the past tense when discussing what you did or found and in the present tense when describing what is known (eg, the evidence).
Manuscript body
Your manuscript body is a nonfiction story, with a beginning (Introduction), a middle (Methods and Results) and an ending (Discussion); in the biomedical publishing world this is called the IMRaD structure. All of the pieces of your story should connect and the information must be consistent. The introduction describes why your research was undertaken and what question you wanted to answer. The methods explain how your results were achieved; whatever you promise in the methods needs corresponding data in the results section, tables or figures. The discussion answers your research question, summarises where your findings fit in the existing body of evidence and discusses what this means moving forward.
Our manuscript body follows the IMRaD structure and includes information recommended in the SQUIRE guidelines in each section.13 Within each section, we describe its purpose, offer tips to organise the content and end with an example of how this section may read.
Introduction
The introduction provides the context regarding why your research is needed and important. Limit this section to one double-spaced page (about 300 words, generally two or three paragraphs) and cite the most recent and relevant evidence to support your statements. While you want to exhibit a thorough literature search, avoid describing and citing every article you read. You can elaborate on important details from your literature search in the discussion section. In general, comment on studies in the aggregate rather than as individual studies.
Your introduction should funnel down from the broader problem to your specific action to resolve the problem. Define the problem in the leading sentence and back this up with current evidence. Justify why your study is needed, clarifying the limitations or gaps in the current knowledge and making the connection to your study. In the next paragraph, summarise what you intended to improve; include the study aim and the tipping point that prompted the change. This point may have been a series of adverse events in your workplace, high complication rates across the USA or a national patient safety goal. If you are testing a hypothesis (evaluation study), consider including it here rather than (or in addition to) in your methods section. End this section with your main research question or questions.
Introduction Examplea
Define problem (lead sentence): ‘Communication problems are common during patient handoffs and linked to preventable harm.’
Current evidence (remainder of paragraph 1): {Include the evidence delineating how common communication problems are during handoffs. Reference [R] your statement and read the author instructions to determine if the in-text citation goes before or after the punctuation mark. Provide the summary estimates linking patient handoffs to preventable harm.[R] If available, also include any evidence linking poor communication to preventable harm.[R]}
Make a connection (next paragraph): ‘Checklists have improved the exchange of important information between caregivers when transferring patients to another team or unit.[R] Nonetheless, information sharing remains a substantial problem during temporary hand-offs for inpatient testing.’
Intended improvement (same or new paragraph): ‘The specific aim of this study was to send a sheet that communicated the medical information Radiology technicians needed to safely perform an imaging study on inpatients. We chose radiology because the complication rate among inpatients undergoing imaging studies was high and missing patient information (eg, allergies) was a common cause of these complications.’
Research question (end of introduction): ‘We sought to assess whether the sheet was an effective and efficient way to communicate pertinent patient information during temporary handoffs, and whether complication rates decreased among inpatients undergoing Radiology imaging studies.’
aQuotation marks set off an example of content, and italicised text within brackets offers recommendations for content.
Methods
The methods section describes what you did. The editor and reviewers will carefully scrutinise this section to determine whether your study represents good science. Provide sufficient detail to show how the study can be replicated, to evaluate how bias may influence your study results, and to consider how another organisation may implement the intervention. Think of the methods as a historical documentation of your study in which more is better. Organise your methods in a logical or chronological order that makes sense to the reader. For instance, it is more logical to describe the intervention (intended to have an effect on an outcome) before the outcome variable.
Describe your research framework first, including the study design, study period, population of interest (if there is one), setting, ethical issues and institutional review board (IRB) approval. Also, introduce the reader to your project by mentioning the intervention and main outcome. Whether an improvement or safety project requires IRB review remains unclear, causing review processes to vary widely by hospital.14 A new ethical framework highlights the moral imperative to learn and improve and may provide guidance.15 ,16 Given the local variation in oversight for quality improvement work, consult your hospital IRB when planning a project and describe the criteria that decided whether your project required IRB review in your methods. Explain why or how the setting and the population (if appropriate) were chosen and justify exclusions (eg, children).
Under the subheading, Intervention, or a more descriptive title, explain your programme theory (how the intervention related to the improved outcome and why you chose them). The theory will offer a way to understand and predict the effects of your quality improvement or patient safety project.17 Also describe how the intervention was implemented in the setting, how you assessed its effectiveness and how you evaluated its impact on your outcome. Describe whether or how your intervention evolved over time. If multiple sites participated, mention whether they modified the implementation phase to fit the local context. In some instances, iterative changes in an improvement intervention will generate qualitative data that should be reported in your results section. If your intervention is substantially refined during the implementation phase based on what you have learned, this new knowledge should go in your results.6 Thus, provide the context for the intervention's evolution in the methods so the reader will understand the basis for your results. It may help to supply an online supplement with additional details about your evaluation of the intervention overtime and the learning that occurred.
If you have multiple interventions, use different subheadings. Use appropriate subheadings (eg, Data Collection and Variables) to describe your data collection methods, variables, and defining information about the variables. If you administered a survey, for example, describe how it was developed, pilot tested and administered, and define the respondent categories (eg, bedside nurse, radiology laboratory technician). Describe your primary outcome measure, any secondary outcomes and hypothesis if it was not stated in your introduction (some journals want all of this information under a new subheading). End the methods with an Analysis subsection, describing the statistical analyses and the software product used.
Quality improvement researchers typically collect data at multiple time periods (called time series measurements) to evaluate variations in performance over time. The intervention often varies over time. If you are evaluating the impact of an intervention, collect baseline data for comparison to your postimplementation data. If your study includes a single site, statistical process control methods are often helpful. If your study includes multiple sites, time series regression analysis, which allows for time-dependent covariates, for adjustment of historical trends and for confounding, will help reduce potential biases when reporting your findings. These methods, which are well developed for observational clinical studies, also help the authors communicate their results by providing a point estimate for the degree of improvement, usually in the form of a risk ratio. Researchers should avoid single time period pre/post studies because the post-time period is often defined after the results are available (encouraging authors to pick the time period that shows the greatest improvement) and have the most risk for bias. Fan and colleagues offer guidance to interpret robust study methods for quality improvement.18
Reporting the science of quality or safety improvement in healthcare requires a fair amount of explanation. Your methods will likely be the longest section of your manuscript. Table 1 shows how the methods connect to the data reported in the results.
Common subheadings for methods section mapped to structure of results
Methods Example with Subheadings
‘Study design and setting
This prospective cross-sectional study tested the patient information sheet on the adult inpatient medicine service from September 2009 to March 2010. We chose this service because of the high frequency of temporary handoffs for inpatient testing. Paediatric inpatients were excluded to increase the homogeneity of our sample population. A survey was administered at the end of the 6-month pilot study to assess the efficacy of the sheet.
Patient information sheet
The sheet intended to communicate pertinent patient information that the radiology technician needed to safely perform the imaging study, and to reduce the risk of complications. The sheet was developed by two patient safety leaders (one nurse, one physician) and distributed to three bedside nurses and three physicians on the medicine service in August 2009 to determine face validity. Figure X illustrates the final sheet that was pilot tested. The bedside nurse printed out the patient information sheet from the electronic medical record (EMR) and gave it to the transporter. Patient transporters were instructed, at the time of patient pick up, to give the sheet to the radiology technician performing the test.
The pilot study was introduced to radiology technicians and patient registrars in a staff meeting. Radiology technicians were instructed to record the unique identification number (assigned when the sheet was generated from the EMR) on a log to document receipt of the sheet and answer two questions: Was the medical information useful? Was it necessary to call the unit for more information about the patient? Radiology technicians or the registrar used the same log to keep a count of inpatients arriving without a sheet (stratified by unit or floor). Patient-specific information was not collected to maintain anonymity. The study project coordinator collected the log at the end of each week.
Survey and data collection
A three-item survey was administered to bedside nurses on the medical inpatient units and to radiology technicians between April and June, 2010. The survey elicited opinions regarding the usefulness of the patient information sheet. The items included the following:’ {include verbatim wording of each question or assemble a table with the questions as row headings and corresponding data in columns and point the reader to the table}. ‘The response category was dichotomous. The project coordinator distributed the survey during staff meetings and collected it after the meeting. Survey respondents were instructed to refrain from putting their name on the survey to maintain anonymity. The project coordinator returned for a second staff meeting to capture additional respondents.
Primary and secondary outcome variables and hypothesis
The primary outcome measure was efficacy of information sharing, calculated as the number of inpatient sheets wherein the technician did not call the unit for additional information, divided by the total number of inpatients with a documented sheet delivery. The secondary outcome measure was the complication rate after 6 months of exposure to the patient information sheet. We hypothesised that use of the sheet would decrease the frequency of radiologic imaging-related complications among adult inpatients. We obtained complication rates (baseline and postimplementation) from the radiology quality assurance officer; rates were calculated per 100 diagnostic imaging studies.
Analysis
Survey data were summarised as proportions. We compared complication rates at baseline to rates 6 months after the sheet was implemented; mean±SD were reported. Paired t tests were performed and statistical significance defined as p<0.05.’
Results
The results section should highlight pertinent findings from your study in an objective manner. This section is not meant to convince the reader why your findings are important; save adjectives for your discussion. ‘Significant’ only applies if you can provide supporting confidence intervals or p values below your threshold for statistical significance, usually <0.05. Pay close attention to parallel construction within sentences and across sentences. Parallel construction establishes a rhythm and an expectation of content that easily walks the reader through your findings. The following example highlights nonparallel and parallel construction of the same sentence.
-
Nonparallel: The baseline complication rate was 11.5 per 100 diagnostic imaging studies compared to 1.3/100 diagnostic imaging studies 6 months after the intervention was implemented.
-
Parallel: The complication rate was 11.5 per 100 diagnostic imaging studies at baseline compared to 1.3 per 100 diagnostic imaging studies 6 months after the intervention was implemented.
The results section should follow the same logical order presented in the methods (table 1). If you compare predata and postdata, the logical order will always report the predata (baseline) first in a sentence (as done in both examples above), giving the reader a reference point to compare the postintervention results. Report the demographics/characteristics of your population or setting first (usually the first table) to illustrate the framework of your study. Next, report what you found, starting with unadjusted estimates followed by any adjusted estimates (other tables/figures). Again, only highlight important results and use your tables and figures to show all the data. If you have a substantial amount of qualitative data, report it in bullet format in a table or box and provide the main points in the text. As a quality check, any data reported in your results must be defined in the methods. For example, if you report complications rates by type of surgery, the methods section should describe how you categorised types of surgery and complications.
Results Example
Framework of study: ‘Ninety of 92 (98%) inpatients from the medicine service had a patient information sheet on presentation to radiology for diagnostic imaging (table 1).’
What you found: {The length of your results section may determine whether subheadings are needed. If subheadings will make the connection to the methods, use them; the editorial office can always delete subheadings if they feel they are unnecessary.}
‘Efficacy of sheet: Eighty-five of 90 (85%) patient information sheets shared pertinent medical information. Eight-nine of 100 (89%) survey respondents felt the sheet was an effective communication tool (Table X).
Complication rates in Radiology: The complication rate was 11.5 per 100 diagnostic imaging studies at baseline compared to 1.3 per 100 diagnostic imaging studies 6-months after the intervention was implemented (Figure X).’
Discussion
The discussion should make sense of your findings. You want to interpret and discuss your findings, not regurgitate data. Tell the reader what is important and what they should do with this information. In the first paragraph, answer your research question and summarise important findings. For example, ‘our intervention was associated with a 66% reduction in infections over 18 months.’ Unless your study was a randomised controlled design, use words that imply an association (as described in the previous example) rather than declare or infer causality (eg, the intervention reduced infections).18 Explain why your findings are new and important knowledge; even negative findings will offer useful information.
In the next paragraph or two put your findings in the context of other relevant studies, expanding on similarities and differences. Discuss how your study builds on prior studies and what knowledge your study adds. Talk about your intervention and any contextual factors that helped or hindered your intervention (did any other study encounter the same issues?). Reiterate your hypothesis and explore any differences in what you observed and expected. Discuss whether the intervention would work in other hospitals in the same setting or even translate to different clinical settings (is it generalisable?). This is a question broached by many, particularly anyone working with limited resources in quality improvement and patient safety. If your study is translatable, simple or inexpensive, mention these strengths.
In the next paragraph, discuss the implications of your research for stakeholders, whether they are clinicians, patients or policymakers. What does this mean for them and what should they do? In the next paragraph, or even earlier in your discussion, disclose your study limitations in a subsection, titled Limitations. Disclose all the limitations, any expected impact on the inferences you made and your efforts to mitigate or eliminate the effects of these limitations. Conclude with a strong take-away message about the importance of your findings. Your conclusion should be brief (four sentences or less) to ensure your message is not missed by the reader. As a last bit of advice, keep the discussion as short as possible and tightly connected to your results and research question.
Discussion example
Answer research question: ‘We found that the patient information sheet was a practical and effective mode of communication between bedside nurses and radiology technicians.’
Summarise important findings: ‘The majority of nurses and technicians reported that the sheet saved time and relayed pertinent patient information. Moreover, use of the sheet was associated with decreased complication rates among inpatients undergoing diagnostic imaging in Radiology.’
Put findings in context of existing body of literature: ‘No known studies have addressed poor communication during temporary hand-offs for inpatient testing.’ {Discuss any published studies describing interventions that focused on exchange of information during transitions of care (eg, between units, between care teams). As you do this, walk the reader through what is known, where your findings fit, and what this means.}
Discuss if generalisable: ‘Although we only tested the sheet with medicine patients undergoing radiology imaging, it would generalise to other patient populations and clinical testing areas. The sheet could be easily adapted to print any patient information from the EMR for any medical test.’
Explore implications: ‘This study has important implications for clinical practice. The sheet was easily generated from the patient's EMR and was an effective way to communicate patient information to an inpatient testing unit. It was an inexpensive solution to a problem that was causing costly complications.’
Consider limitations: ‘The study has several limitations. First, the sample size was small and only one clinical area was studied. Second, we did not collect confounders that may have influenced complications rates and cannot make inferences about the impact of the sheet.’ {In this section it is good to offer brief counterarguments for a limitation.}
Conclusion: The patient information sheet was a quickly generated tool that effectively communicated medical information during temporary handoff of inpatients to Radiology. Moreover, there was an associated decrease in complication rates in the diagnostic imaging area. This tool should be tested in other clinical areas of the hospital.’
References
The reference list follows the manuscript body and begins on a new page. Each journal has specific formatting requirements for the in-text citations and the list of references (read author instructions). The in-text citation is the call out (number, or author last name and date) in your manuscript body, tables, and figures that points to the corresponding full reference in the list. Use a software program to automate the management and manipulation of your references. Proof the reference list carefully to ensure the information is complete, accurate, and formatted according to the journal specifications. Check links to web content to ensure they are active.
As a general rule, include anything accessible to the public in the reference list, such as journal articles, books, book chapters and websites. A more detailed list of reference types is available from the International Committee of Medical Journal Editors Uniform Requirements for Manuscripts Submitted to Biomedical Journals.19 If you make a statement based on a personal communication or unpublished data, note this in parentheses at the end of the statement (eg, personal communication, Jane Smith, MD, 17, July 2011) and obtain written permission from the individual to include this information and grant publication rights if the manuscript is accepted.
Tables and figures
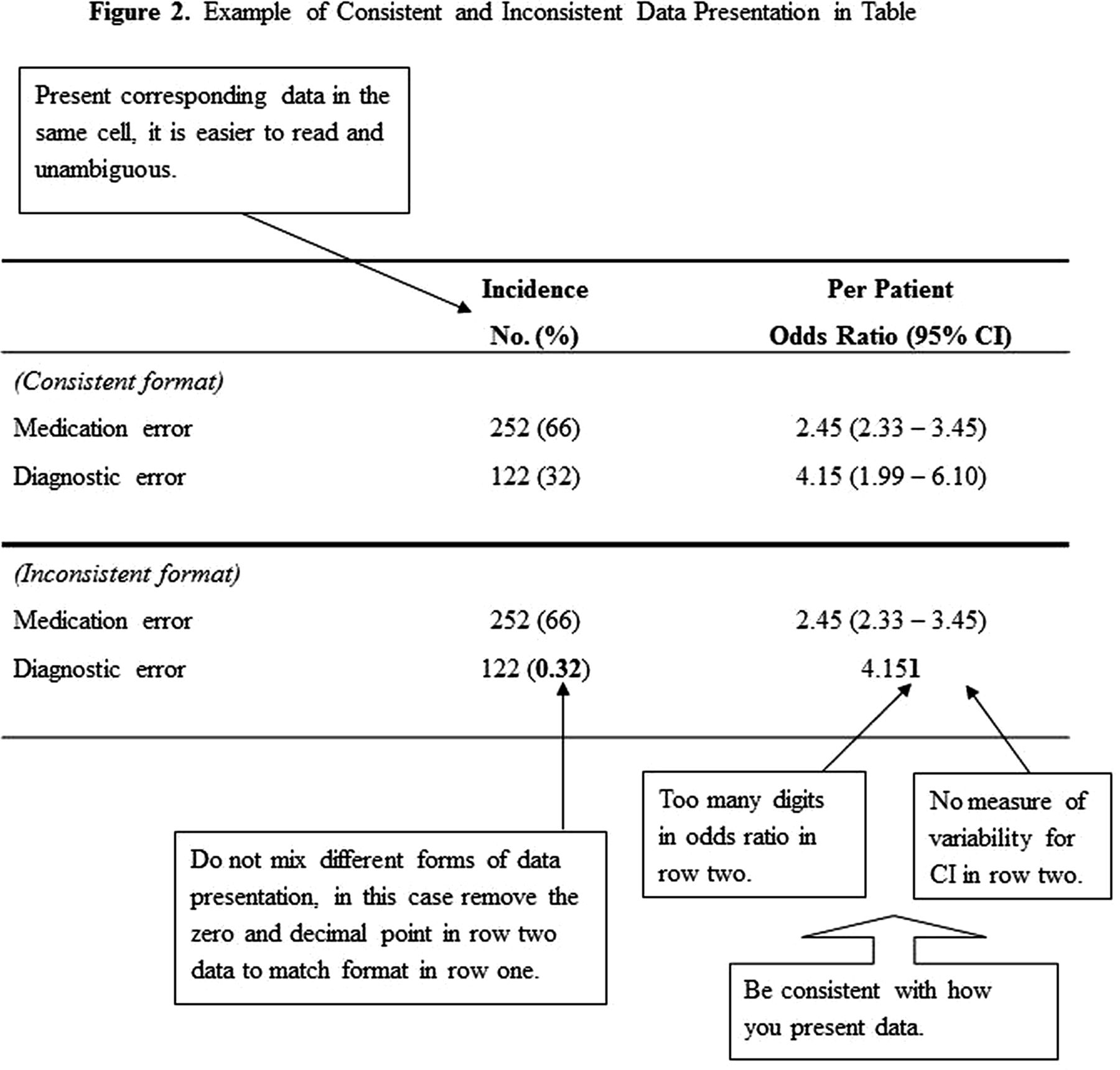
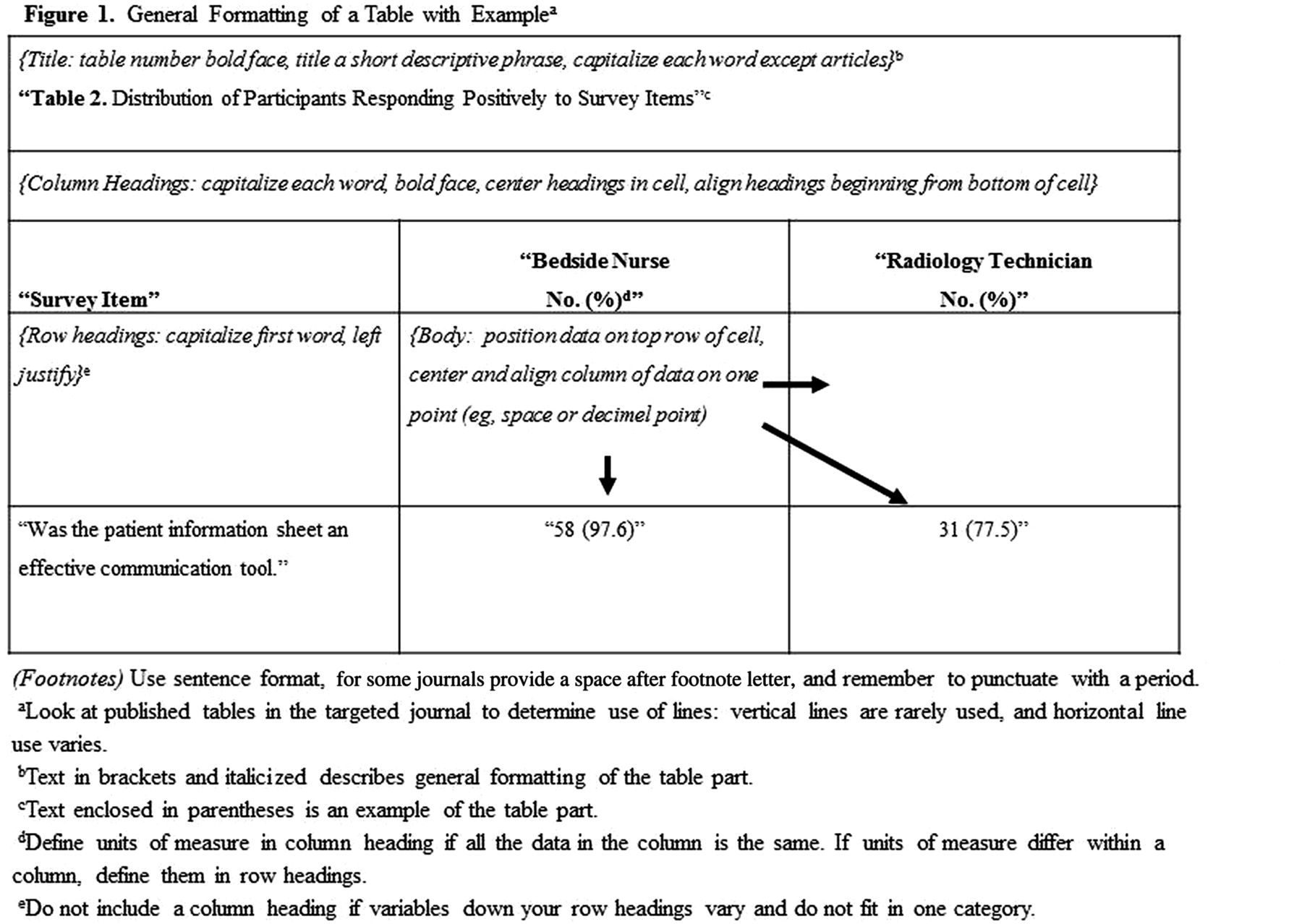
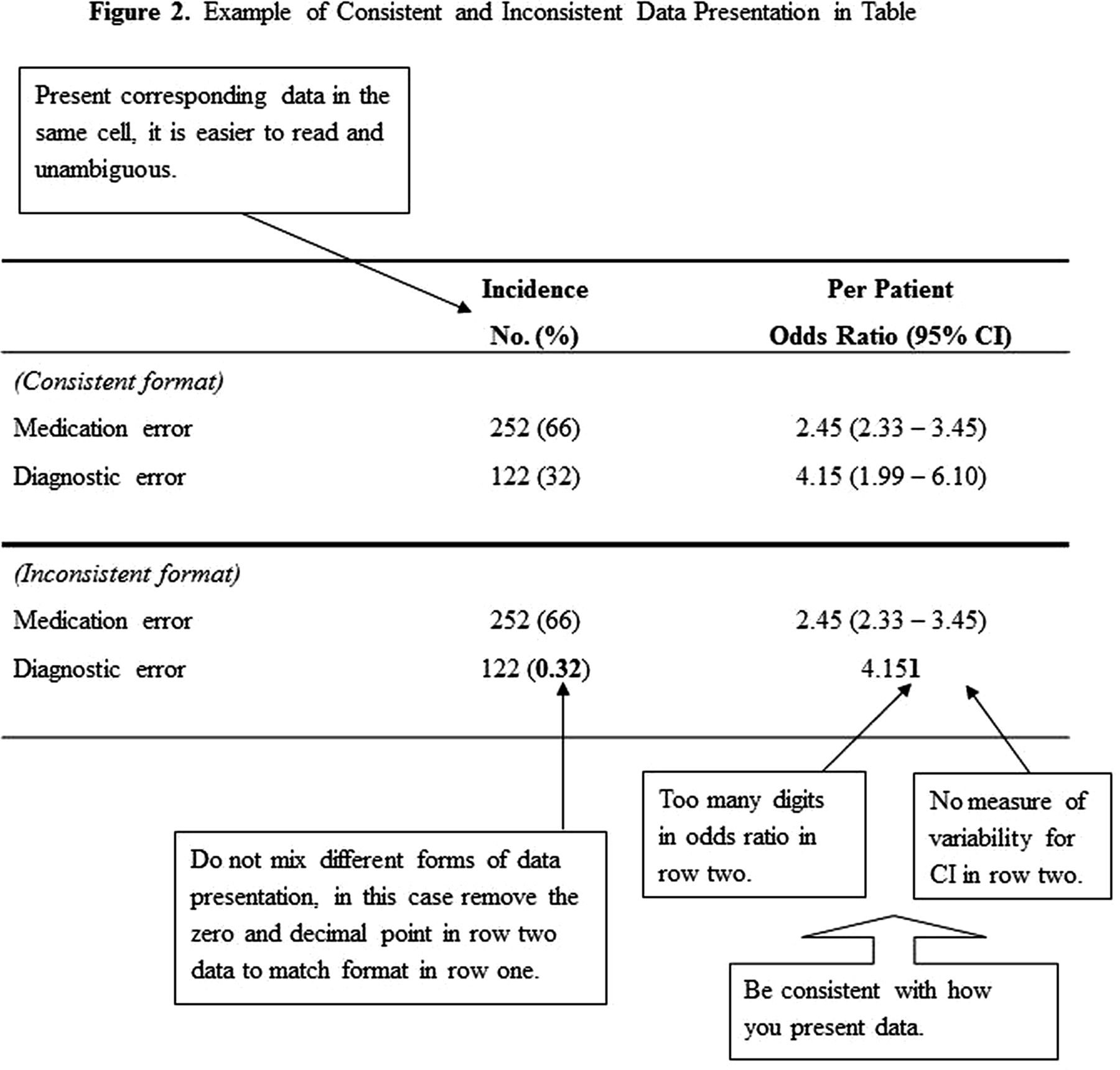
The tables follow your reference list (or figure legend page) and precede your figures. Present each table and figure on a separate page in chronological order. Your tables and figures must stand alone without referring to the manuscript. Therefore, use footnotes to define abbreviations and describe statistical methods for estimates reported in a table, and provide a legend page that clearly explains each figure. Use concise short titles and standardise the format and presentation of data in your tables. We have provided a (figure 1) that dissects the components of a table and offers some common formatting requirements, and a (figure 2) that illustrates how to present data in a table. It may help to annotate a graph of your performance data over time, labelling when interventions were implemented or pertinent times when it evolved. If you include any tables or figures previously published, you must obtain permission from the publisher for copyright privileges; this process can be found on the publisher's website.
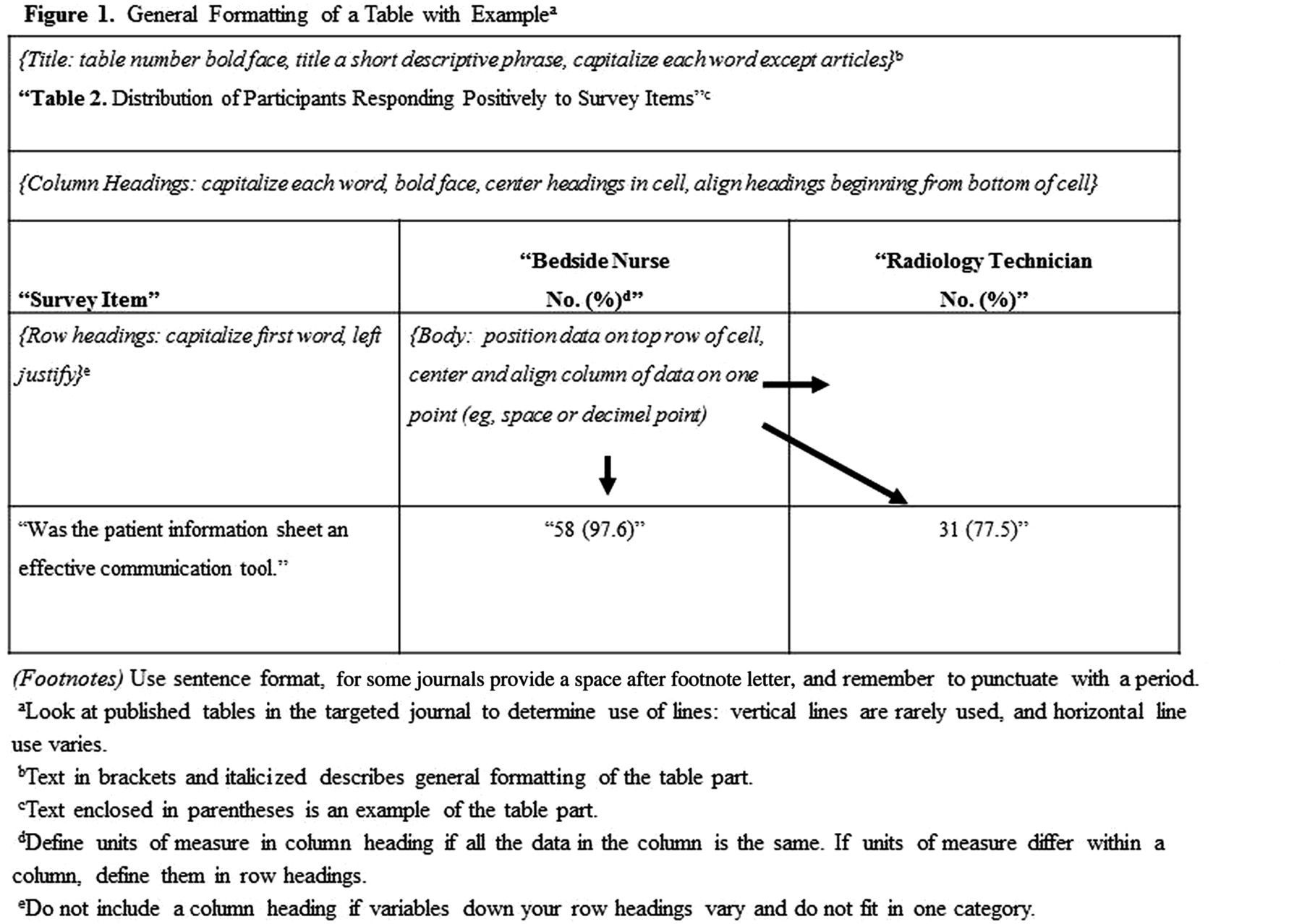
Shows the five parts of a table: title, column headings, row headings, body and footnotes. Each part is labelled and the general formatting rules described and set off by brackets and italic font. An example of each part is enclosed in quotation marks.
{kind=link}
{kind=link}
Focuses on the consistent presentation of data in a table. The reference format in row one provides an example of how data should be presented compared to row 2 in which inconsistent formatting and missing data are illustrated.
Acknowledgement section
This section follows your manuscript body and describes anyone who contributed to your study but did not meet the three criteria for authorship. For example, an individual who collected data, but did not work on the manuscript, only meets one criterion.19 Provide their name, degrees, professional affiliation, and description of contribution (again, obtain written permission to publish their name). Other content in this section or elsewhere (such as the title page) includes the authors’ conflicts of interest relevant to the research being reported,20 a statement expanding on author contributions, and any financial support for the research and the manuscript production. Many journals supply a conflict of interest form that outlines types of financial and nonfinancial information that should be disclosed, be transparent when reporting and follow the instructions. It takes time to gather this information and, in many cases, the form(s) required by a journal. Try to collect this information and any forms (including a copyright form) when the authors are reviewing the manuscript rather than when the paper is ready for submission.
Conclusion
In summary, organising and writing a manuscript reporting quality improvement or patient safety research is not as intimidating as it may seem. Think about your target audience, choose an appropriate journal, read the author instructions and several published articles, and use this article and checklist of common mistakes (table 2) to help you along the way. Your study is a nonfiction story in which it is best to write the sections separately. One approach is to write the middle (methods then results) first, followed by your ending (discussion), and then your introduction. While we have not mentioned this previously, it is an appropriate ending: there is better writing through rewriting. A good, quick reference book to help you is Strunk and White's The Elements of Style.21
Checklist to avoid common mistakes
Footnotes
-
Contributors CGH provided the concept and design, drafted the article and revised it for critical intellectual content, and provided final approval for submission of the manuscript. PJP contributed to critical revisions of the article, offered supervision and gave final approval of the version submitted.
-
Competing interests Ms Holzmueller received honoraria from MCIC Vermont, Inc. to conduct a workshop on organising and writing a manuscript describing quality improvement and patient safety research. Dr Pronovost reports receiving grant or contract support from the Moore Foundation, the Agency for Healthcare Research and Quality, the National Institutes of Health, RAND and The Commonwealth Fund for research related to measuring and improving patient safety; honoraria from various hospitals and healthcare systems and the Leigh Bureau to speak on quality and safety; consultancy with the Association for Professionals in Infection Control and Epidemiology, Inc.; and book royalties for authoring ‘Safe Patients, Smart Hospitals: How One Doctor's Checklist Can Help Us Change Health Care from the Inside Out.’
-
Provenance and peer review Not commissioned; externally peer reviewed.