Early administration of epinephrine (adrenaline) in patients with cardiac arrest with initial shockable rhythm in hospital: propensity score matched analysis
BMJ 2016; 353 doi: https://doi.org/10.1136/bmj.i1577 (Published 06 April 2016) Cite this as: BMJ 2016;353:i1577
- Lars W Andersen, research fellow1 2 3,
- Tobias Kurth, professor of public health and epidemiology4,
- Maureen Chase, assistant professor1,
- Katherine M Berg, instructor of medicine5,
- Michael N Cocchi, director of critical care quality1 6,
- Clifton Callaway, professor of emergency medicine7,
- Michael W Donnino, director of center for resuscitation science1 5
- for the American Heart Association’s Get With The Guidelines-Resuscitation Investigators
- 1Department of Emergency Medicine, Beth Israel Deaconess Medical Center, Rosenberg Building, One Deaconess Road, Boston, MA 02215, USA
- 2Department of Anesthesiology, Aarhus University Hospital, Nørrebrogade 44, Bygn. 21, 1 Aarhus 8000, Denmark
- 3Research Center for Emergency Medicine, Aarhus University Hospital, Trøjborgvej 72-74, Bygn. 30, Aarhus 8200, Denmark
- 4Institute of Public Health, Charité – Universitätsmedizin Berlin, Seestrasse 73, Berlin D-13347, Germany
- 5Department of Medicine, Division of Pulmonary and Critical Care Medicine, Beth Israel Deaconess Medical Center, 330 Brookline Avenue, Boston, MA 02215, USA
- 6Department of Anesthesia Critical Care, Division of Critical Care, Beth Israel Deaconess Medical Center, 330 Brookline Avenue, Boston, MA 02215, USA
- 7Department of Emergency Medicine, 400A Iroquois, 3600 Forbes Avenue, Pittsburgh, PA 15260, USA
- Correspondence to: M Donnino, Beth Israel Deaconess Medical Center, One Deaconess Road, W/CC 2, Boston, MA 02215, USA mdonnino{at}bidmc.harvard.edu
- Accepted 24 February 2016
Abstract
Objectives To evaluate whether patients who experience cardiac arrest in hospital receive epinephrine (adrenaline) within the two minutes after the first defibrillation (contrary to American Heart Association guidelines) and to evaluate the association between early administration of epinephrine and outcomes in this population.
Design Prospective observational cohort study.
Setting Analysis of data from the Get With The Guidelines-Resuscitation registry, which includes data from more than 300 hospitals in the United States.
Participants Adults in hospital who experienced cardiac arrest with an initial shockable rhythm, including patients who had a first defibrillation within two minutes of the cardiac arrest and who remained in a shockable rhythm after defibrillation.
Intervention Epinephrine given within two minutes after the first defibrillation.
Main outcome measures Survival to hospital discharge. Secondary outcomes included return of spontaneous circulation and survival to hospital discharge with a good functional outcome. A propensity score was calculated for the receipt of epinephrine within two minutes after the first defibrillation, based on multiple characteristics of patients, events, and hospitals. Patients who received epinephrine at either zero, one, or two minutes after the first defibrillation were then matched on the propensity score with patients who were “at risk” of receiving epinephrine within the same minute but who did not receive it.
Results 2978patients were matched on the propensity score, and the groups were well balanced. 1510 (51%) patients received epinephrine within two minutes after the first defibrillation, which is contrary to current American Heart Association guidelines. Epinephrine given within the first two minutes after the first defibrillation was associated with decreased odds of survival in the propensity score matched analysis (odds ratio 0.70, 95% confidence interval 0.59 to 0.82; P<0.001). Early epinephrine administration was also associated with a decreased odds of return of spontaneous circulation (0.71, 0.60 to 0.83; P<0.001) and good functional outcome (0.69, 0.58 to 0.83; P<0.001).
Conclusion Half of patients with a persistent shockable rhythm received epinephrine within two minutes after the first defibrillation, contrary to current American Heart Association guidelines. The receipt of epinephrine within two minutes after the first defibrillation was associated with decreased odds of survival to hospital discharge as well as decreased odds of return of spontaneous circulation and survival to hospital discharge with a good functional outcome.
Introduction
Epinephrine (adrenaline) has been used in resuscitation after cardiac arrest for decades and the provision of epinephrine is currently suggested by both the American Heart Association (AHA) and the European Resuscitation Council (ERC) in both shockable and non-shockable rhythms.1 2 Despite this, the utility of epinephrine administration in patients with cardiac arrest remains controversial.3 4 5 6 7 8 9
The effect of epinephrine is thought to be mediated primarily through α-adrenergic effects10 leading to improved coronary perfusion pressure,11 which is associated with increased probability of return of spontaneous circulation in animals12 and humans.13 The effect on cerebral perfusion, however, remains controversial.11 14 Human interventional and observational studies in patients who have cardiac arrest outside hospital have consistently found improved return of spontaneous circulation but have yielded inconsistent results with regard to long term outcomes.15 16 17 18 We have previously found that delay in the first administration of epinephrine is associated with a decreased chance of good outcomes in both adults19 and children20 in hospital who experience cardiac arrest with an initial non-shockable rhythm but there is a lack of published studies in such patients presenting with a shockable rhythm (that is, pulseless ventricular tachycardia or ventricular fibrillation). As additional highly effective interventions are recommended in these patients (primarily early defibrillation), clinical decision making becomes even more complex and both the efficacy and the optimal timing of administration of epinephrine remain unknown. Currently, there are discrepant recommendations for treatment from the AHA and the ERC, with the AHA recommending epinephrine after the second defibrillation and the ERC after the third defibrillation.1 2 In addition, clinical practice patterns could include the provision of epinephrine even earlier, such as after the first defibrillation, in patients with a persistently shockable rhythm.
We used a large multicenter registry of cardiac arrest in inpatients in the United States to describe the use of epinephrine during cardiac arrest with a shockable rhythm and to assess compliance with current AHA guidelines. As the recommendation is based essentially on expert opinion as opposed to strong science, we then determined whether early administration of epinephrine (after the first defibrillation) is associated with survival to hospital discharge.
Methods
Study design and data source
This was an analysis of prospectively collected data from the Get With The Guidelines-Resuscitation (GWTG-R) registry. The GWTG-R registry is a national prospective quality improvement registry of inpatients with cardiac arrest sponsored by the AHA. The design for data collection and reliability has been described previously in detail.21 Data are collected on all inpatients with cardiac arrest who do not have prior do not resuscitate orders or cardiopulmonary resuscitation events that began outside the hospital. Cardiac arrest is defined as pulselessness requiring chest compressions and/or defibrillation, with a hospital-wide or unit based emergency response by acute care personnel. The registry uses Utstein-style templates for cardiac arrest, which are a set of standardized reporting guidelines used to define patient variables and outcomes.22 23 Integrity of the data is improved through certification of data entry personnel and the use of standardized software.24 We included data from January 2006, when the AHA guidelines for shockable rhythms changed to their current form,25 to September 2012, after which time the required data fields were no longer part of the registry. Hospital data were obtained from the American Hospital Association’s annual survey from 2013.26
All participating hospitals are required to comply with local regulatory guidelines. Because data are used primarily at the local site for quality improvement, sites are granted a waiver of informed consent under the common rule.
Patient involvement
No patients were involved in determining the research objective or the outcome measures; nor were they involved in the design, conduct, or interpretation of the study. There are no plans to involve patients in the dissemination of results.
Study population
We included adult patients with an index cardiac arrest and a documented initial shockable rhythm (that is, pulseless ventricular tachycardia or ventricular fibrillation). We included only patients who underwent documented first defibrillation within two minutes. This was done because current guidelines recommend defibrillation as the first line treatment (along with chest compressions) for such patients27 and because we considered rapid defibrillation as a surrogate marker for overall quality of resuscitation (currently used as a quality metric by the AHA). Furthermore, previous research has found an association between early defibrillation and improved outcome with comparable outcomes for a time to defibrillation of zero, one, and two minutes.28 We included only patients who had a documented shockable rhythm after the first defibrillation.
We excluded patients who received epinephrine before the first defibrillation, who had return of spontaneous circulation, or in whom resuscitation was terminated within the same minute as the first defibrillation, visitors/employees, patients with missing data on included covariates, those with missing time of epinephrine administration, and patients with missing data on survival (the primary outcome).
Epinephrine and outcomes
Epinephrine administration was defined as any bolus dose of epinephrine given during the cardiac arrest through an intravenous or intraosseous route. Endotracheal administration of epinephrine is not recorded in the registry. The time to epinephrine was defined as the time interval in minutes from the first defibrillation to the first bolus dose of epinephrine. The recording of the time of the first defibrillation and the first dose of epinephrine was done in whole minutes. As such, a time to epinephrine administration of zero minutes means that epinephrine was given within the same whole minute as when the patient was identified as pulseless; a time of one minute represents that epinephrine was given within the next whole minute, etc.
The primary outcome was survival to hospital discharge. Secondary outcomes were return of spontaneous circulation, defined as at least 20 minutes with a palpable pulse, and good functional outcome at the time of hospital discharge. Functional outcome was assessed with the use of the cerebral performance category score (score 1=mild or no neurological deficit, 2=moderate cerebral disability, 3=severe cerebral disability, 4=coma or vegetative state, and 5=brain death).29 A score of 1 or 2 was considered a good functional outcome and a score of 3-5 or death was considered a bad functional outcome, as commonly used in cardiac arrest research.30 31 32 The score was determined by abstractors reviewing the medical record.
Statistical analysis
Descriptive statistics were used to characterize the study population. Continuous variables are reported as medians with interquartile ranges and categorical variables are reported as counts with relative frequencies. Categorical data were compared with χ2 test and continuous data with the Wilcoxon rank sum test. The Cochran-Armitage test was used to assess for trends over time.
The goal of the main analysis was to determine survival to hospital discharge in those who received epinephrine within the two minutes after the first defibrillation (that is, before the recommended second defibrillation) compared with those who did not receive epinephrine or received epinephrine more than two minutes after the first defibrillation. To assess the adjusted relation we performed propensity score matching. The propensity score was calculated with multivariable logistic regression with generalized estimating equations with an exchangeable variance-covariance structure to account for clustering within hospitals. For the calculation of the propensity score, the dependent variable was administration of epinephrine within two minutes after the first defibrillation. We included all variables presented in tables 1, 2, and 3⇓ in the propensity score model. These variables have been defined elsewhere.33 We included quadratic and cubic terms of age, and year of the cardiac arrest was treated as a categorical variable. We also included an interaction term between time to defibrillation and intubation within the first minute as these factors could theoretically affect (timing of) epinephrine.We chose all variables a priori based on prior work and/or clinical reasoning.33 34 35 36 37 38 39
Characteristics of patients in full cohort of patients with cardiac arrest in hospital according to timing of administration of epinephrine. Figures are numbers (percentage) of patients unless specified otherwise
Hospital characteristics in full cohort of patients with cardiac arrest in hospital according to timing of administration of epinephrine. Figures are numbers (percentage) of patients
Characteristic of cardiac arrest in full cohort of patients with cardiac arrest in hospital according to timing of administration of epinephrine. Figures are numbers (percentage) of patients
We next performed 1:1 matching on the propensity score using nearest neighbor matching with a maximum caliber of 0.01 of the propensity score. Patients who received epinephrine at either zero, one, or two minutes after the first defibrillation were separately matched on the propensity score with a patient who was “at risk” of receiving epinephrine within the same time frame. “At risk” patients included those still undergoing resuscitation (that is, patients who did not have return of spontaneous circulation or in whom resuscitation was terminated) and who did not receive epinephrine before or within the same minute, including patients who received epinephrine at a later time point (“as yet untreated” patients).40 The matching was performed separately for minutes zero, one, and two after the first defibrillation with replacement of controls to optimize the sample size. If we included a patient with return of spontaneous circulation within or before this time period, and who was therefore never “at risk” for receiving epinephrine, in the analysis this could bias the results towards a harmful effect of epinephrine because early return of spontaneous circulation (that is, short duration of arrest) is associated with improved survival.39 41 To assess the performance of the matching, we compared baseline categorical variables between the matched groups using the Cochran-Mantel-Haenszel test and calculated standardized differences.
Using the matched cohort, we next performed conditional logistic regression to assess the association between epinephrine administration and survival to hospital discharge. Given the potential importance of time to defibrillation, we included this variable in the regression model as a categorical variable. We report the results from the regression model as odds ratios with 95% confidence intervals. We performed similar conditional logistic regression analyses for the secondary outcomes of return of spontaneous circulation and good functional outcome. To compare the number of total defibrillations, the time to the second defibrillation, total dose of epinephrine, and the time to the end of resuscitation in the two groups we used Poisson regression with robust variance estimates while accounting for the correlation between matched participants. The results of these analyses are presented as relative increases with 95% confidence intervals.
Sensitivity analyses
We performed two predefined sensitivity analyses. First, we performed the propensity score matching without replacement of the control patients. Second, we accounted for missing data for 347 patients (10%) on covariates time of epinephrine administration or survival (fig 1⇓) and for 140 patients (5%) on functional outcome. We imputed missing values for covariates and outcomes by using the fully conditional specification (FCS) method42 and created a total of 10 datasets. As time to epinephrine follows an approximate zero inflated Poisson distribution, we performed imputations for those receiving epinephrine using this distribution for all 10 datasets.20 43 We then performed the propensity score matching and conditional logistic regression on each of these 10 datasets and combined the results using SAS, version 9.4, (SAS Institute, Cary, NC) “proc mianalyze.” We also performed two post hoc sensitivity analyses. As guideline changes can take a substantial amount of time to be implemented,44 and because important changes were made in the 2005 guidelines, we conducted the analysis after excluding events in 2006 and 2007. In our second post hoc sensitivity analysis, we matched only patients who received epinephrine at zero or one minute after the first defibrillation as some patients could have received their second defibrillation during the two minute period.
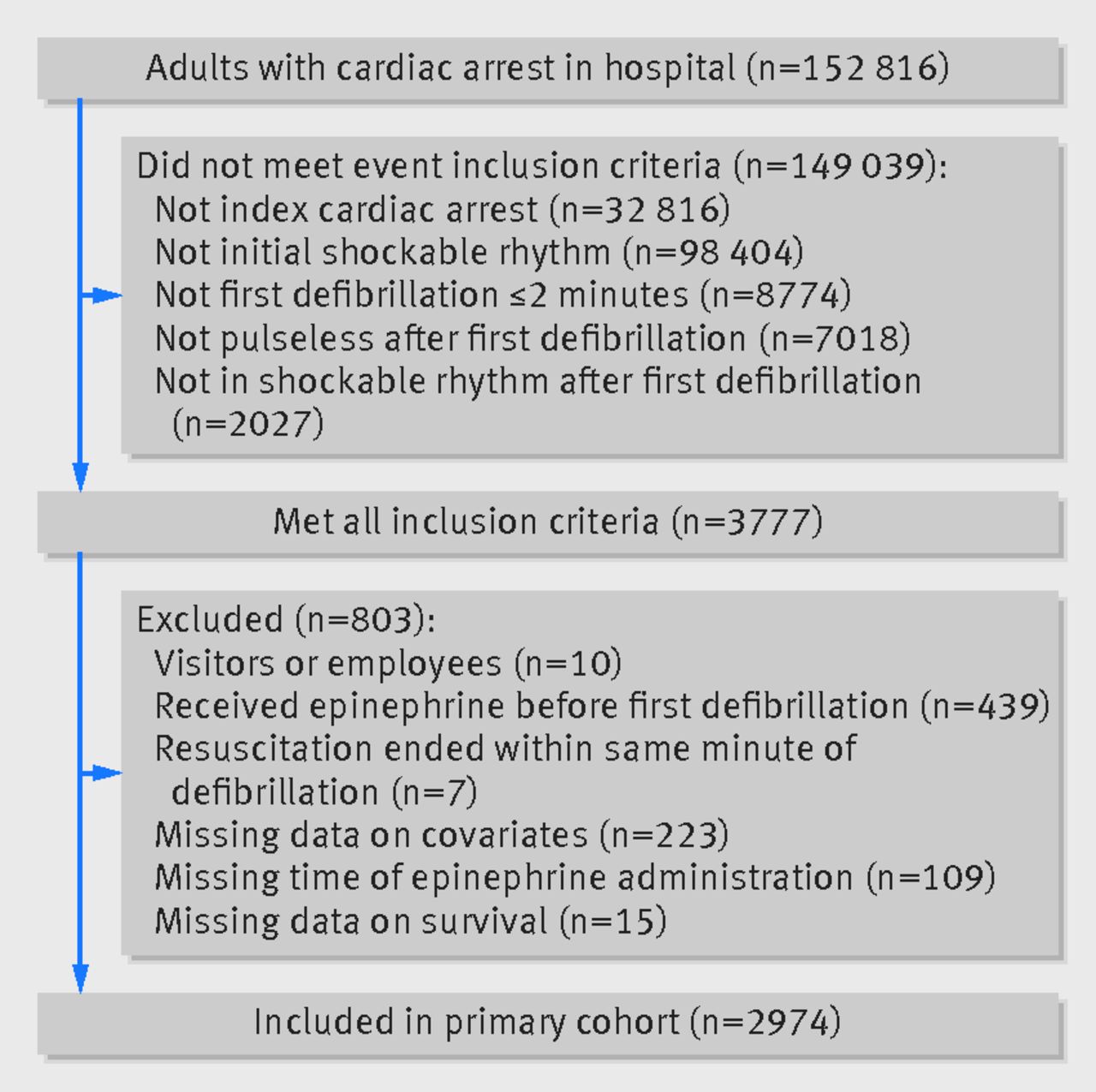
Fig 1 Inclusion and exclusion of patients in study of timing of administration of epinephrine for inpatients with cardiac arrest. Out of 3777 patients who met all inclusion criteria, 2974 were included in main cohort
{kind=link}
Post hoc analyses
We performed two additional post hoc analyses. In the first, we included the same patients as above but also included those who received epinephrine before the first defibrillation. We then restricted the population to those who received a second defibrillation and who received the second defibrillation between one and three minutes after the first defibrillation. In this cohort, we assessed whether receiving epinephrine at any time before the second defibrillation, compared with not receiving epinephrine before the second defibrillation, was associated with the various outcomes. In this analysis, we also utilized propensity score matching as above. In the second analysis, we broadened the inclusion criteria to include patients who had a documented first defibrillation within five minutes with no changes to the remaining inclusion/exclusion criteria. We then performed the main analysis in this patient cohort.
All hypothesis tests were two sided, with a significance level of P<0.05. All secondary analyses should be considered exploratory as we did not adjust for multiple comparisons. We conducted all statistical analyses using SAS software.
Results
Characteristics of study population
We included 2974 patients from 310 hospitals in the main cohort (fig 1⇑). The median age was 65 (interquartile range 54-75), 1041 (35%) were women, and 1167 (39%)survived to hospital discharge. Tables 1, 2, and 3⇓ provide additional characteristics for patients, hospitals, and events for the overall group. Overall, 692 (23%) patients did not receive epinephrine at any time during the resuscitation. Figure 2⇓ shows the timing of epinephrine administration in relation to the first defibrillation.

Fig 2 Distribution of timing of epinephrine in relation to first defibrillation. 692 (23%) patients did not receive epinephrine at any time during resuscitation and 1510 (51%) received epinephrine within two minutes after first defibrillation
{kind=link}
Epinephrine within first two minutes after first defibrillation
In total 1510 (51%) patients received epinephrine within two minutes after the first defibrillation. Tables 1, 2 and 3⇓ show the characteristics of these patients and those not receiving epinephrine within this timeframe. Over time, there was an increase in the incidence of epinephrine given within two minutes after the first defibrillation (275/595 (46%) in 2006 to 118/197 (60%) in 2012, P=0.001 for a linear trend, fig 3⇓, table 3⇑).This increase over time remained in multivariable analysis when we adjusted for variables included in the tables (odds ratio 1.07 per year, 95% confidence interval 1.03 to 1.12; P=0.001).

Fig 3 Proportion of patients with early administration (within two minutes after defibrillation) of epinephrine per year, showing significant increase over time in both bivariable and multivariable analysis (both P=0.001 for linear trends)
{kind=link}
Early epinephrine administration within two minutes after the first defibrillation was associated with a decreased likelihood of survival in unadjusted analysis (464/1510 (31%) v 703/1464 (48%), odds ratio 0.48, 95% confidence interval 0.41 to 0.56; P<0.001). Early epinephrine administration was also associated with decreased likelihood of return of spontaneous circulation (1018/1510 (67%) v 1158/1464 (79%), 0.55, 0.46 to 0.65; P<0.001) and good functional outcome (357/1445 (25%) v 567/1389 (41%), 0.48, 0.41 to 0.56; P<0.001).
Propensity score matched cohort
We matched 2978 patients on the propensity score for receipt of epinephrine within the first two minutes after defibrillation. Characteristics of the two groups in the matched cohort are displayed in appendix 1, and the distributions of propensity scores before and after matching are displayed in appendix 2. The two groups were well balanced on all included variables (all P>0.05 with standardized differences between −0.1 and 0.1). In the matched cohort, epinephrine administration within two minutes after the first defibrillation was still associated with decreased odds of survival (odds ratio 0.70, 95% confidence interval 0.59 to 0.82; P<0.001). Epinephrine administration also remained associated with a decreased odds of return of spontaneous circulation (0.71, 0.60 to 0.83; P<0.001) and good functional outcome (0.69, 0.58 to 0.83; P<0.001), see figure 4⇓. These associations remained significant when we analyzed patients with return of spontaneous circulation (n=1974) for survival (0.79, 0.64 to 0.98; P=0.03) and good functional outcome (0.77, 0.61 to 0.96; P=0.02).

Fig 4 Graphical representation of odds ratios in propensity matched cohort for outcomes survival, return of spontaneous circulation (ROSC), and good functional outcome epinephrine administration compared with no epinephrine administration ≤2 min after first defibrillation. Error bars represent 95% confidence intervals
{kind=link}
Patients who received early epinephrine had a similar number of total defibrillations as those not receiving early epinephrine (median 3 (interquartile range 2-5) in both groups; relative increase 1.03, 95% confidence interval 0.98 to 1.09; P=0.25). In each group 87% of patients had a second defibrillation (P=0.91). There was no difference in the time from the first defibrillation to the second defibrillation (median 2 minutes (1-3) in both groups; relative increase: 0.77, 0.58 to 1.03; P=0.08). Patients who received early epinephrine had a higher total dose of epinephrine (3 mg (1-4) v 1 mg (0-3); relative increase: 1.57, 1.47 to 1.68; P<0.001). Time to return of spontaneous circulation was similar in those who did and did not receive early epinephrine (13 minutes (7-27) v 13 minutes (6-26); relative increase 1.02, 0.93 to 1.13; P=0.63). The time to termination of resuscitation efforts in patients who did not achieve return of spontaneous circulation was also similar (22 minutes (14-32) v 21 minutes (14-29); relative increase 1.05, 0.95 to 1.17; P=0.32).
Sensitivity analyses
We included 2310 patients in the matched cohort without replacement of controls. The association between early epinephrine administration and survival remained in this cohort (odds ratio 0.73, 95% confidence interval 0.62 to 0.87; P<0.001). The association between early epinephrine and return of spontaneous circulation (0.72, 0.60 to 0.87; P<0.001) and functional outcome (0.68, 0.56 to 0.83; P<0.001) also remained. The full cohort used for multiple imputation to account for missing data included 3321 patients. Between 3330 and 3519 patients were matched in the 10 created datasets. The combined estimate for the matched cohorts was similar to that reported in the main analysis for survival (0.72, 0.61 to 0.85; P<0.001), return of spontaneous circulation (0.76, 0.62 to 0.94; P=0.01), and good functional outcome (0.75, 0.63 to 0.99; P=0.001).
In our first post hoc sensitivity analysis, which excluded events in 2006 and 2007, we matched 1878 patients. The association between early epinephrine administration and survival (odds ratio 0.70, 0.57 to 0.85; P<0.001), return of spontaneous circulation (0.76, 0.62 to 0.84; P=0.01), and functional outcome (0.71, 0.57 to 0.89; P=0.003) remained. In our second post hoc sensitivity analysis, we matched only the 1418 patients in the zero and one minute timeframes (that is, excluding minute two). The association between early epinephrine administration and survival (0.72, 0.57 to 0.90; P=0.004) and functional outcome (0.70, 0.54 to 0.90; P=0.007) remained. The association between early epinephrine administration and return of spontaneous circulation was not significant in this sensitivity analysis (0.82, 0.65 to 1.03; P=0.09).
Additional analyses
There were 1758 patients in the cohort of patients with epinephrine administration any time before the second defibrillation, of whom 1252 were propensity score matched. The groups were well matched. In this analysis, we looked at epinephrine administration at any time before the second defibrillation compared with no epinephrine administration before the second defibrillation. We found that early epinephrine administration was also associated with decreased odds of survival (odds ratio 0.54, 95% confidence interval 0.42 to 0.69; P<0.001), return of spontaneous circulation (0.55, 0.42 to 0.72; P<0.001), and good functional outcome (0.55, 0.42 to 0.72; P<0.001) in this analysis.
In the cohort of patients with the first defibrillation within five minutes, we matched 3520 patients for propensity score. In this cohort, the results remained similar. Early epinephrine administration was associated with decreased odds of survival (odds ratio 0.77, 95% confidence interval 0.66 to 0.89; P<0.001), return of spontaneous circulation (0.73, 0.63 to 0.85; P<0.001), and good functional outcome (0.77, 0.66 to 0.91; P=0.002).
Discussion
For in hospital patients with cardiac arrest and a shockable rhythm, administration of epinephrine within the first two minutes after the initial defibrillation was common and was associated with decreased chance of return of spontaneous circulation, survival, and survival with a good functional outcome compared with those who were not given epinephrine within this period. This association remained when we used time dependent propensity score matching and in sensitivity analyses.
Epinephrine background and guideline recommendation
Epinephrine, a potent α- and β-adrenergic agonist with inotropic, chronotropic, and vasoconstrictive effects,45 has been used during cardiac arrest for decades. This practice is partly based on findings from animal studies from the 1960s,6 46 47 and epinephrine has been recommend since 1974 when the American Heart Association (AHA) published its first recommendations on cardiac arrest.48 The most recent AHA guidelines state that it is “reasonable to consider” epinephrine every three to five minutes for patients with a non-shockable rhythm and every three to five minutes after the second defibrillation in patients with a shockable rhythm.1 In the current study, we found that over half of our included patients received epinephrine within two minutes after the first defibrillation (contrary to current guidelines). The true proportion of patients treated contrary to guidelines is even larger as we excluded 439 who received epinephrine before the initial defibrillation. Furthermore, we found that the proportion of patients who received early epinephrine has been increasing over the years (from 46% in 2006 to 60% in 2012), a finding that remains largely unexplained.
Comparison with previous studies
The published evidence in humans regarding the use of epinephrine in cardiac arrest with shockable rhythms is scant, especially in those who experience cardiac arrest as inpatients and in the early stages of arrest.4 To our knowledge, one randomized controlled trial has compared intravenous drug administration during cardiac arrest outside hospital with no intravenous drug administration,49 and only one randomized controlled trial has been published directly comparing epinephrine with placebo.15 In this trial, Jacobs and colleagues analyzed 534 patients with cardiac arrest outside hospital and found that those who were randomized to epinephrine had markedly increased rate of return of spontaneous circulation and admission to hospital, but they also found no significant difference in survival or survival with a good functional outcome, although the study was underpowered to detect such differences.15 In the group of patients with an initial shockable rhythm, which was the focus of our investigation, the findings were similar to those of the non-shockable group, although the magnitude of the benefit regarding return of spontaneous circulation was somewhat less compared with in the non-shockable group.15 In Jacobs and colleagues’ study, epinephrine was administered after the third unsuccessful defibrillation, consistent with European and Australian guidelines.2 15 Furthermore, all patients had cardiac arrests outside hospital, and the mean response time of emergency providers was about 10 minutes, making any comparison with the current study difficult or essentially impossible.
Recently, several large observational studies regarding the use of epinephrine in cardiac arrest outside hospital have been published.16 17 50 In a large Japanese study utilizing a similar statistical approach as here, Nakahara and colleagues found that administration of epinephrine in the prehospital setting was associated with increased overall survival but found no difference in good functional recovery among patients with a shockable rhythm.17 While these findings are different from the current report, Nakahara and colleagues also examined a different population of patients (cardiac arrest outside hospital), a different algorithm, and a different time of epinephrine administration. As noted by other investigators,51 there are profound differences between patients with cardiac arrest in and outside hospital, both in term of patients’ characteristics, underlying etiology, treatment and timing of treatment, and outcomes. As such, the efficacy of interventions such as epinephrine might vary between these populations.
Potential mechanisms
There are multiple potential reasons for why epinephrine could be detrimental in early cardiac arrest with a shockable rhythm. Patients with a shockable rhythm more often have a cardiac cause of their arrest.52 Epinephrine’s β-adrenergic effects could increase myocardial oxygen demand, which, despite increased coronary perfusion pressure, can lead to increased myocardial damage and increased myocardial dysfunction after cardiac arrest.53 54 Epinephrine can also decrease blood flow to other organs including the kidneys,55 lungs,56 and brain14 as well as reduce microcirculatory blood flow.57 All these findings, however, are from controlled animal studies and are not consistent between studies.11 As such, their translation to complex heterogeneous patients with various underlying etiologies and interventions is questionable.
Although it was not the primary focus of our study, we found that those receiving early epinephrine received a higher cumulative dose during their cardiac arrest (3 mg (interquartile range 1-4) v 1 mg (0-3); P<0.001). Previous observational studies have found that a high cumulative epinephrine dose is associated with worse outcomes,58 59 and it is possible that the cumulative dose in the current study could be a driver of outcomes. It also remains possible that the early administration of epinephrine could have interfered with the administration or quality of other interventions, such as subsequent defibrillations, chest compressions, or airway management. In contrast to epinephrine, defibrillation has minimal, if any, side effects. Therefore, one could postulate that an effective treatment with limited side effects might be superior to another with important side effects, particularly early in the arrest period (that is, what has been termed, the “electrical phase” of cardiac arrest).60 In other words, during the electrical phase of cardiac arrest many patients with shockable rhythms could have return of spontaneous circulation with defibrillation, without the need for an intervention such as epinephrine with potential side effects. This contrasts with non-shockable rhythms, where treatments are limited to cardiopulmonary resuscitation and attempts to deal with the underlying etiology of arrest. Of note, in one animal study epinephrine had no effect on subsequent success of defibrillation, although animals treated with epinephrine had increased return of spontaneous circulation.61 An ongoing large randomized controlled trial comparing epinephrine with placebo in cardiac arrest outside hospital (“Paramedic2”),62 currently enrolling in the United Kingdom, will help answer many lingering questions, but the translatability to cardiac arrest in hospital, where interventions are usually administered much earlier, is unknown.
Limitations of study
The design and limitations of the current study should be taken into account in the interpretation of the findings. Despite adjustment for multiple patient, event, and hospital factors, and with the timing of epinephrine taken into account, this is an observational study and no strong conclusions can be made regarding the causal effect of early epinephrine administration. Unknown and/or unmeasured confounders, such as the quality of cardiopulmonary resuscitation, could have changed our results if they had been included in the analysis. Despite inclusion of data from more than 300 hospitals, the sample size was inadequate for making inference about epinephrine administration at later time points (such as after the second and third defibrillation). As such, these findings should not be extrapolated to later time points, nor to settings outside hospital. Furthermore, most of our included patients were monitored at the time of the arrest. This might not be comparable with other settings and countries,63 which could limit the generalizability of our findings.
The GWTG-R registry does not collect information on endotracheal administration of epinephrine. In the unlikely event of this occurring in the “no early epinephrine group,” however, we believe this would bias our results towards to null. Misclassification of variables could have influenced our results, given the nature of this data registry. Misclassification related to timing of interventions would be especially concerning,64 65 although we suspect that errors would more likely occur for absolute times rather than relative times (that is, differences between two time points), which we used for this study. Furthermore, we believe that any misclassification, including those related to timing, would be unrelated to outcomes and would therefore most likely bias the results towards the null (that is, this potential bias is unlikely to explain our current finding).
Conclusion
In conclusion, we found that early administration of epinephrine after the first defibrillation (that is, contrary to guidelines) was common (>50%) in patients who experience cardiac arrest in hospital with a shockable rhythm. Moreover, the provision of epinephrine at this time point was associated with a decreased chance of good outcome, including decreased in hospital survival. These findings might be relevant to guideline developers, educators, and clinicians involved with the care of such patients.
What is already known on this topic
There is conflicting evidence regarding the effectiveness of epinephrine in patients with cardiac arrest outside hospital
Little is known about the effectiveness of epinephrine in patients in hospital who experience cardiac arrest with a shockable rhythm, particularly early during the arrest
What this study adds
Early administration of epinephrine after the first defibrillation (that is, contrary to guidelines) was common in inpatients with cardiac arrest and a shockable rhythm (> 50%)
Provision of epinephrine at this time point was associated with a decreased chance of good outcome including decreased survival in hospital
Footnotes
Get with the Guidelines-Resuscitation Investigators
MWD, Paul S Chan (Saint Luke’s Mid America Heart Institute), Steven M Bradley (VA Eastern Colorado Healthcare System), Girotra Saket (University of Iowa Carver College of Medicine), Monique L Anderson (Duke Clinical Research Institute), Matthew M Churpek (University of Chicago), Ahamed H Idris (University of Texas Southwestern Medical Center), Dana P Edelson (University of Chicago), Robert T Faillace (Geisinger Healthcare System), Romergryko Geocadin (Johns Hopkins University School of Medicine), Raina Merchant (University of Pennsylvania School of Medicine), Vincent N Mosesso Jr (University of Pittsburgh School of Medicine), Joseph P Ornato and Mary Ann Peberdy (Virginia Commonwealth University), Sarah M Perman (University of Colorado, School of Medicine), Mindy Smyth (retired).
Contributors: LWA and MWD were responsible for study concept and design, acquisition of data, and drafting of the manuscript. LWA and TK performed the statistical analysis. All authors interpreted the data, critically revised the manuscript for important intellectual content and approved the final version for submission. All authors agree to be accountable for all aspects of the work. LWA and MWD are guarantors.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organization for the submitted work; no financial relationships except as noted below with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. MWD is a paid consultant for the American Heart Association.
Ethical approval: All participating hospitals in the Get With The Guidelines-Resuscitation registry are required to comply with local regulatory guidelines. Because data are used primarily at the local site for quality improvement, sites are granted a waiver of informed consent under the common rule.
Transparency: The lead author affirms that this manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant) have been explained.
Data sharing: No additional data available.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/.