Article Text

Abstract
Purpose To determine intentional injury burden, incident characteristics, and outcomes among Ugandan youth.
Methods A cross sectional analysis of trauma registry data from accident and emergency units of five regional referral hospitals was conducted. Data had been prospectively collected from all patients accessing injury care at the five sites between July 2004 and June 2005: youth records were analysed.
Results Intentional injuries among youth victims, especially school-age males, are common in all five regions, constituting 7.3% of their injury burden with a male dominance. Intentional youth victimisation mainly occurred at home, on roads, and in public places; incidents were largely due to blunt force, stabs/cuts, and gunshots in general, although variations in causes were evident depending on age. Intentional injuries among the youth victims often manifested as head, neck, and face injuries: 2% were severe and there were 4%case fatalities at 2 weeks.
Conclusions and recommendations Intentional injuries among youth victims, especially school-age males, are important contributors of injury burden in all five sites. Homes, roads, and public places are unsafe for Ugandan youth. Although guns were used in all five sites, less lethal mechanisms (blunt force, stabs/cuts, and burns) are the most common with variations between locations. Incidents involving teenage housewives could reflect underlying problem of domestic violence. Community based studies could be highly informative. Youth should be prioritised for prevention of injuries both in and out of school.
- Youth
- intentional injury
- trauma registry
- Uganda
- adolescent
- violence
- youth violence, injury outcomes, Uganda
Statistics from Altmetric.com
- Youth
- intentional injury
- trauma registry
- Uganda
- adolescent
- violence
- youth violence, injury outcomes, Uganda
Introduction
Violence is a common cause of mortality in Africa.1–5 The extent of violence attributed to youth is not clear. World Health Organization (WHO) estimates place Africa's youth homicides at double the global average of 9.2/100 000.6 In Uganda, injuries and violence have been ranked among the top six mortality causes (MOH–CDC, 1996); 13–21% of injury deaths are intentional, with proportional youth victimisation rates ranging between 14% and 24%. Homes constitute 55% of intentional injury locations, with women as the most common intentional domestic injury victims. Other locations include roads and public facilities. Gunshots, blunt trauma, and cuts/stubs are lead intentional injury mechanisms, although with variations across locations. Recent media reports seem to indicate an upsurge in youth victimisation in Uganda, especially child sacrifice, school arsons and strikes, child abductions, (child) sexual violations, corporal punishments, and gang activities.7–10
Much of what is known about injuries in Uganda is, however, facility based and limited in geographic scope. Few community studies have been conducted. To generate a more national picture, the existing hospital based injury surveillance system (described elsewhere)11–13 was expended to five regions (Uganda has five major geo-political divisions). Referral facilities were targeted because of their capacity for major trauma management. It was not clear how the expansion would modify the known injury patterns, especially youth victimisation. We set out to determine the intentional injury patterns and characteristics of youth victims in the five regions using trauma registry data. We adopt the WHO definition of youth as persons between the ages of 13 and 23 years.6
Methods
Study design
A cross sectional analysis of trauma registry data from accident and emergency units of five regional referral hospitals was undertaken. Data prospectively collected earlier (between July 2004 and June 2005) from all patients accessing injury care by specifically trained casualty department staff were used. Records of intentionally injured (self-inflicted, assaults, and war related) victims are analysed. The registry (primary dataset) disaggregates intentional injuries as self-inflicted or assaults.
Setting
Data originated from regional referral hospitals. Uganda operates a tiered healthcare system with two national and 11 regional referral facilities. Lower units are organised within district health services.14 Referral hospitals have resident surgeons. Lacor, the northern site, has an estimated bed capacity of 548 and is 315 kilometres from Kampala in a war affected region; Mbarara, the south-western site, has an estimated bed capacity of 500 and is 266 kilometres from Kampala along the highway to Rwanda; Fort Portal (estimated bed capacity of 200), the western site, is approximately 300 kilometres from Kampala; Mbale (estimated bed capacity of 400), the eastern site, is approximated 250 kilometres from Kampala; and Mulago (total bed capacity of over 1500), one of two national referral hospitals, is in the capital. Referral facilities have resident surgeons and are designated for more specialised care from catchments on referral bases; they do, however, provide routine primary care. The five facilities were selected for their prominence as care centres in the five geo-political regions. The 2002 spatial distribution of Uganda's population is 6.6% in central, 6.2% in eastern, 3.2% in northern, and 4.5% in western regions.15
Participants
Study participants were intentionally injured youth seeking care at the five referral facilities. The accessible population was those whose records were captured in respective registries. Only incident cases were eligible and official referrals were tracked.
Data sources and variables
Trauma registries earlier established and managed by the Injury Control Centre–Uganda (ICC-U) provided primary data. Injury data on all patients accessing injury care at the study sites had been recorded using a standard format. The registry form includes WHO recommended minimal datasets for injury surveillance. Specifically trained emergency care staff completed the forms. Completed forms are field edited by surveillance staff and entered into a computerised database. Regular reports are generated and disseminated to the National Health Ministry, participating hospitals, and interested institutions. Variables analysed in the current study included age, gender, time, place, activity at injury time, intent, injury mechanism, severity, nature, affected body part, and outcome. Presence of alcohol had been subjectively assessed by emergency staff; this is not mandatory. Except for blunt injury and stabs/cuts, classification of external causes had been derived from ICD-10.12 Severity had been assessed using the Kampala Trauma Score (KTS). Although simplified for low resourced outpatient settings, KTS has all elements of the trauma and injury severity scores.16 Surveillance system sensitivity had been estimated in 2000 to range between 28% (in Mulago) and 70% (in Lacor), with good daytime but poor night-time coverage. The WHO definition of youth as persons aged between 13 and 23 years is applied.6
Statistical methods
Data analysis was conducted using STATA V.8: incident characteristics were disaggregated by age, location, and cause, and summarised using proportions. The total number of injuries captured in the registries constituted the overall injury burden at the five sites. Odds of occurrence were computed by age, cause, and location and compared for differences. Proportional incidence rates were also calculated by age, location, and cause and used to establish risk trends for youth.
Results
A total of 7415 injured patients were registered in the five regions between June 2004 and July 2005; 22.2% of the injuries were intentional. One third (510) of the intentional injuries involved youth victims: 95% of them were assaults, 3% were self-inflicted, and 2% were war related. Subsequent results are based on all three categories of youth victims.
Intentional injuries among youth victims constituted 7.3% of total injury burden in the five (regional) facilities. Their distribution was skewed towards older youth (18–23 years), peaking at 21 years (see figure 1). Males doubled the female proportion (32.7%) of youth victims. Generally, the effect of age on intentional injury odds was marginal (OR=1.07, CI=1.03 to 1.10).

Age distribution of intentional injuries.
Students accounted for 28% of intentionally injured youth victims: casual labourers constituted 21%, housewives, 11%, and others 40% (see table 1). Over half (55%) of the injured housewives were 12–19 years old. Above the age of 23 years, casual labourers (20.1%), followed by peasants (17.3%) are the most common intentional injury victims: below age 10 years, students/pupils (72.1%), followed by children (22.9%) are the most frequent (see table 1). Age influenced occupational intentional injuries patterns (p<0.001). Students exhibited greater intentional injury risk among school-age youth.
Intentional incident characteristics by incident location, occupation and age group
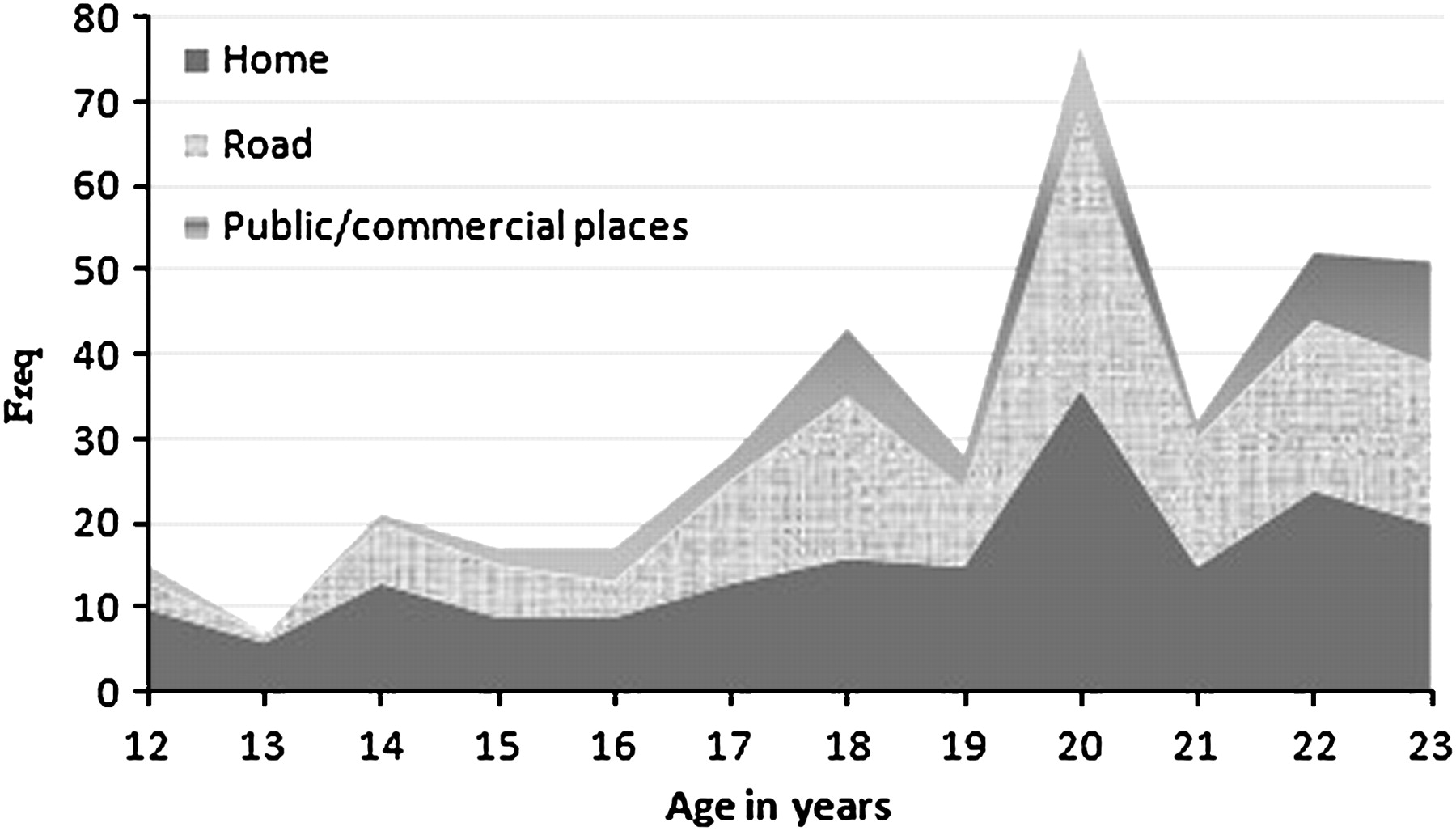
Leading intentional injury locations were homes (34.1%), roads (31.7%), and public places (11.5%) (see figure 2). In general, blunt force (45.28), stabs/cuts (18.45%), and gunshots (12.02%) were the most common injury mechanisms. There were, however, significant differences in injury mechanisms across age strata and locations (p<0.001, see table 1). Alcohol was suspected in 37.4% of cases.

{kind=link}
{kind=link}
Intentional injury proportion by location.
Cuts/bites or open wounds (55%), followed by bruises/superficial injuries (17%) were the top two intentional injury types among youth victims: the majority were minor (KTS >8). Head, neck, and face were the most common (31%) seriously injured body parts. Only 2% of intentional injuries were severe (KTS <6). Of the 171 admissions, fatalities at 2 weeks were 4%.
Discussion
This study described intentional injury patterns and characteristics among youth victims in Uganda. It shows youth victims as constituting one fifth of the total injury burden at the five study sites. Although the effect of age on injury odds was marginal, youth victimisation tended to be skewed towards older ages, peaking at 21 years. Males doubled female prevalence with an absolute difference of 70.6%. Students, followed by casual labourers and housewives were the most common victims; 55% of intentionally injured housewives were teenagers. Homes, roads, and public places were the lead incident locations, with blunt force, stabs/cuts, gunshots, and burns as cross-cutting mechanisms. The most prevalent injury types were cuts/bites or open wounds and superficial injuries; the majority were minor. Case death was 4%.
These findings are more national given their geographical scope. Variations from earlier findings include: more modest intentional domestic injury prevalence of 43% compared to previously reported estimate of 55%; male dominance of intentional domestic injuries contrary to the previous finding; over-representation of teenagers among intentionally injured housewives which was not previously reported; and an increment in youth victimisation in South Central Uganda (as compared to a 1998 estimate). The main limitations include: inherent biases associated with routine data such as coverage and completeness errors (the sensitivity of this surveillance system had earlier been estimated to range between 28% and 70%); the facility basis of the study which limits external validity of findings; and the fact that socioeconomic status, as a major violence determinant, was not measured. Current intentional injury prevalence of 22% is, however, comparable to the previous estimates (14–24%).
A number of factors could account for our findings: adolescence being a transitional stage is characterised by biologically and socioculturally driven physical, physiological, psychosocial, and behavioural changes that influence intentional injury risks and patterns among them. The skewing of injuries towards older youths may have had developmental correlates including age related risk taking. Regarding the incidents among teenage housewives, it was unclear whether this reflected an emerging trend or improved detection. It is also not clear if it was associated with underlying intimate partner or domestic violence. Studies have, however, shown teenage motherhood to be associated with violence risks such as poor health, poor educational attainment, poor employment prospects, negative attitudes, and socioeconomic deprivation.17 18 In Uganda, sexual maturity is legally regulated: the age of sexual majority is 18 years. Further qualitative community studies are recommended.
The gender difference in intentional youth victimisation was real: masculinity could account for this. The relationship between masculinity and violence has been explored and documented in the past.19 This could have been compounded by the general lack of safety in schools and homes, which is a national rather than regional problem as previously indicated. The low case death rates could reflect dominance of low lethality mechanisms in the majority of cases; gunshots were, however, reported at all sites.
The study underscores the importance of intentional injuries among youth victims in Uganda; highlighting, among others, teenage housewives as a high risk group. Their predominance could indicate failure of the sexual majority law in Uganda. The safety and suitability of Ugandan homes and schools as places of nurture and child upbringing is also questionable given the intentional injuries in them. The findings show gun violence to be a problem in Uganda's non-civil and civil conflict regions despite current strict controls. This should motivate for a national response to armed violence in Northern Uganda. The findings also question the effectiveness of existing gun regulation and control mechanisms. Their importance as choice tools of violence could be growing in Uganda. The study also highlights the significance of time in intentional injury risk distribution throughout youth.
Future research could focus on contexts, victim–perpetrator relationships, family relationship types, and socioeconomic status of victimised teenage housewives. Childcare practice linkages and gender differences in public place, farm, and sports related victimisation also require further review.
Conclusions and recommendations
Intentional injuries are important emergence visit causes among youth victims in Uganda. They are significant contributors to Uganda's injury burden. Homes, roads, and other public places are unsafe for Ugandan youth. Blunt force, stabs/cuts, burns, and gunshots are the most prevalent intentional injury mechanisms. Teenage housewives are the lead female victims of intentional home incidents. Burns in homes and gunshots on streets and in public places are common. Community studies could be informative. Prevention needs to prioritise youths in and out of schools. Gender based violence screening in healthcare could be beneficial.
What is already known on the subject
Violence is an important cause of injury in Africa and both rural and urban Uganda.
However, violence prevention is not well prioritised in the Ugandan Public Health Policy.
What this study adds
A large proportion of Uganda's intentional injury is due to youth victimisation in both private and public places.
Youth violence prevention needs to be prioritised for youths both in and out of schools.
Youth housewives are a high risk group for intentional domestic injuries.
Acknowledgments
This paper is based on data from the ongoing hospital based Injury Surveillance Program of the Injury Control Center–Uganda. Special thanks are extended to Mulago, Mbarara, Fort Portal, Lacor, and Mbale regional referral hospitals for providing the primary data.
Footnotes
Funding The study on which this manuscript is based was funded by the Government of Uganda in 2004/05 using a World Bank facility under the 10 year Country Road Sector Improvement Program at the Ministry of Works.
Competing interests None.
Ethics approval This paper is part of the dissemination of ongoing injury surveillance that was set up in 1996 with approval from Mulago Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Correction