
Abstract
Purpose
Surgical treatment is crucial in the management of necrotizing soft tissue infections (NSTIs). The aim of this study was to determine the influence of surgical procedure timing on hospital mortality in severe NSTI.
Methods
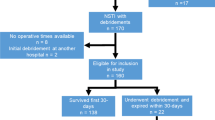
A retrospective study including 106 patients was conducted in a medical intensive care unit equipped with a hyperbaric chamber. Data regarding pre-existing conditions, intensive care and surgical management were included in a logistic regression model to determine independent factors associated with hospital mortality.
Results
Overall hospital mortality was 40.6%. In multivariate analysis, underlying cardiovascular disease, SAPS II, abdominoperineal compared to limb localization, time from the first signs to diagnosis <72 h, and time from diagnosis to surgical treatment >14 h in patients with septic shock were independently associated with hospital mortality.
Conclusion
In patients with NSTI and septic shock, hospital mortality is influenced by the timing of surgical treatment.

Similar content being viewed by others


References
Stevens DL, Bisno AL, Chambers EF, Everett ED, Dellinger P, Goldstein EJC, Gorbach SL, Hirschmann JV, Kaplan EL, Montoya JG, Wade JC (2005) Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin Infect Dis 41:1373–1406
McHenry CR, Piotrowski JJ, Petrinic D, Malangoni MA (1995) Determinants of mortality for necrotizing soft tissue infections. Ann Surg 221:558–565
Elliott DC, Kufera JA, Roy AM, Myers M (1996) Necrotizing soft tissue infections. Risk factors for mortality and strategies for management. Ann Surg 224:672–683
Liu YM, Chi CY, Ho MW, Chen CM, Liao WC, Lin PC, Wang JH (2005) Microbiology and factors affecting mortality in necrotizing fasciitis. J Microbiol Immunol Infect 38:440–445
Childers BJ, Potyondy LD, Nachreiner R, Rogers FR, Childers ER, Oberg KC, Hendricks DL, Hardesty RA (2002) Necrotizing fasciitis: a fourteen-year retrospective study of 163 consecutive patients. Am Surg 68:109–116
Korkut M, Içöz G, Dayangaç M, Akgün E, Yeniay L, Erdogan Ö, Cal C (2003) Outcome analysis in patients with Fournier’s gangrene. Report of 45 cases. Dis Colon Rectum 46:649–652
Wong CH, Chang HC, Pasupathy S, Khin LW, Tan JL, Low CO (2003) Necrotizing fasciitis: clinical presentation, microbiology, and determinants of mortality. J bone joint Surg Am 85:1454–1460
Russell JA (2006) Management of sepsis. N Engl J Med 355:1699–1713
Faucher LD, Morris SE, Edelman LS, Saffle JR (2001) Burn center management of necrotizing soft tissue surgical infections in unburned patients. Am J Surg 182:563–569
Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ (1992) Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 101:1644–1655
Le Gall JR, Lemeshow S, Saulnier F (1993) A new simplified acute physiology score (SAPS II) based on a European/North American multicenter study. JAMA 270:2957–2963
Vincent JL, Moreno R, Takala J, Willatts S, De Meendonça A, Bruining H, on behalf of the working group on sepsis related problems of the ESICM (1996) The SOFA (sepsis related organ failure assessment) score to describe organ dysfunction/failure. Intensive Care Med 22:707–710
Artigas A, Bernard GR, Carlet J, Dreyfuss D, Gattinoni L, Hudson L, Lamy L, Marini JJ, Matthay MA, Pinsky MR, Spragg R, Suter PM (1998) The American-European Consensus Conference on ARDS, part 2: ventilatory, pharmacologic, supportive therapy, study design strategies, and issues related to recovery and remodeling. Acute respiratory distress syndrome. Am J Respir Crit Care Med 157:1332–1347
Majesky JA, Alexander JW (1983) Early diagnosis, nutritional support and immediate extensive debridement improve survival in necrotizing fasciitis. Am J Surg 145:784–787
Voros D, Pissiotis C, Georgantas D, Katsaragakis S, Antoniou S, Papadimitriou J (1993) Role of early and extensive surgery in the treatment of severe necrotizing soft-tissue infections. Br J Surg 80:1190–1191
Hsiao GH, Chang CH, Hsiao CW, Fanchiang JH, Jee SH (1998) Necrotizing soft-tissue infections. Surgical or conservative treatment? Dermatol Surg 24:243–248
Hsiao CT, Weng HH, Yuan YD, Chen CT, Chen IC (2008) Predictors of mortality in patients with necrotizing fasciitis. Am J Emerg Med 26:170–175
Singh G, Sinha SK, Adhikary S, Babu S, Ray P, Khanna SK (2002) Necrotizing infections of soft tissues. A clinical profile. Eur J Surg 168:366–371
Norton KS, Johnson LW, Perry T, Perry KH, Sehon JK, Zibari GB (2002) Management of Fournier’s gangrene: an eleven year retrospective analysis of early recognition, diagnosis and treatment. Am Surg 68:709–713
Endorf FW, Supple KG, Gamelli RL (2005) The evolving characteristics and care of necrotizing soft-tissue infections. Burns 31:269–273
Anaya DA, McMahon K, Nathens AB, Sullivan SR, Foy H, Bulger E (2005) Predictors of mortality and limb loss in necrotizing soft tissue-infections. Arch Surg 140:151–157
Acknowledgments
The authors thank Tara Embleton, University Hospital Medical Editor, for her valuable advice in editing this manuscript. The authors confirm that there was no grant support.
Conflict of interest statement
The authors have no conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Boyer, A., Vargas, F., Coste, F. et al. Influence of surgical treatment timing on mortality from necrotizing soft tissue infections requiring intensive care management. Intensive Care Med 35, 847–853 (2009). https://doi.org/10.1007/s00134-008-1373-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-008-1373-4