
Summary
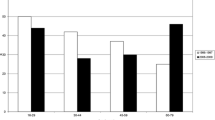
The present study compares the clinical outcome, as expressed by the Glasgow outcome scale, of two groups of severely head injured patients treated before (49 patients) and after (72 patients) the establishment of a neurosurgical intensive care (NIC) unit at the department of neurosurgery, Uppsala University Hospital. The number of “good recoveries” increased significantly after the establishment of the NIC. This was confirmed by univariate analysis (p<0.05) and by multivariate analysis using the logistic regression model to adjust for differences between the two groups of patients (p<0.05, p<0.005). The most striking improvement was found in patients with a Glasgow coma motor score (GCS M)⩾4 on admission. In this subgroup of patients the “good recoveries” increased from 15% to 52%. The object of NIC is basically to prevent or minimize secondary brain damage, and it seems logical that the effect of such care is most obvious in GCS M⩾4 patients in whom a good outcome can be anticipated if secondary damage can be prevented or minimized.
In conclusion, the present study shows that improved clinical outcome after severe head injury can be achieved by organizing an NIC unit with a well trained staff capable of providing this care 24 hours a day using established methods of surveillance and treatment.
Article PDF
Similar content being viewed by others

References
Becker DP, Miller JD, Ward JD, Greenberg RP, Young JD, Sakalas R (1977) The outcome from severe head injury with early diagnosis and intensive management. J Neurosurg 47: 491–502
Bowers SA, Marshall LF (1980) Outcome in 200 consecutive cases of severe head injury treated in San Diego County: a prospective analysis. Neurosurgery 6: 237–242
Colohan AR, Alves WM, Gross CR, Torner JC, Metha VS, Tandon PN, Jane JA (1989) Head injury mortality in two centers with different emergency medical services and intensive care. J Neurosurg 71: 202–207
Eisenberg HM, Frankowski RF, Contant CF, Marshall LF, Walker MD (1988) High-dose barbiturate control of elevated intracranial pressure in patients with severe head injury. J Neurosurg 69: 15–23
Gelpke GJ, Braakman R, Habbema Dik J, Hilden J (1983) Comparison of outcome in two series of patients with severe head injuries. J Neurosurg 59: 745–750
Gennarelli TA, Spielman GM, Langfitt TW, Gildenberg PL, Harrington T, Jane J, Marshall LF, Miller JD, Pitts LH (1982) Influence of the type of intracranial lesion on outcome from severe head injury.A multicenter study using a new classification system. J Neurosurg 56: 26–32
Gordon E, Pontén U (1976) The non-operative treatment of severe head injuries. In: Vinken PJ, Bruyn GW (eds) Handbook of clinical neurology, vol 24. North Holland Publ Co, Amsterdam, pp 599–626
Heiden JS, Weiss MH (1978) Head injury management, letter to the editor. J Neurosurg 48: 491
Jennett B, Bond M (1975) Assessment of outcome after severe brain damage.A practical scale. Lancet 1: 480–484
Jennett B, Teasdale G, Galbraith S, Pickard J, Grant H, Braakman R, Avezaat C, Maas A, Minderhoud J, Vecht CJ, Heiden J, Small R, Caton W, Kurze T (1977) Severe head injuries in three countries. J Neurol Neurosurg Psychiatry 40: 291–298
Jennett B, Teasdale G, Fry J, Braakman R, Minderhoud J, Heiden J, Kurze T (1980) Treatment for severe head injury. J Neurol Neurosurg Psychiatry 43: 289–295
Kalbag RM (1978) Head injury management, letter to the editor. J Neurosurg 48: 489–490
Langfitt TW, Gennarelli TA (1982) Can the outcome from head injury be improved? J Neurosurg 56: 19–25
Lundberg N (1960) Continuous recording and control of ventricular fluid pressure in neurosurgical practice. Acta Psych Scand [Suppl] 149: 36
Lundberg N, Kjällquist Å, Bien CH (1959) Reduction of increased intracranial pressure by hyperventilation. Acta Psych Scand 34 [Suppl] 139
Lundberg N, Troupp H, Lorin H (1965) Continuous recording of the ventricular-fluid pressure in patients with severe acute traumatic injury: a preliminary report. J Neurosurg 22: 581–590
Marshall LF, Smith RW, Shapiro HM (1979a) The outcome with aggressive treatment in severe head injuries. Part 1: The significance of intracranial pressure monitoring. J Neurosurg 50: 20–25
Marshall LF, Smith RW, Shapiro HM (1979b) The outcome with aggressive treatment in severe head injuries. Part II: Acute and chronic barbiturate administration in the management of head injury. J Neurosurg 50: 26–30
Mendelow AD, Karmi MZ, Paul KS,et al (1979) Extradural haematoma: effect of delayed treatment. Br Med J 1: 1240–1242
Miller JD (1989) Measuring ICP in patients — its value now and in the future. In: Hoff JT, Betz AL (eds) Intracranial pressure VII. Springer, Berlin Heidelberg New York Tokyo, pp 5–15
Muizelaar JP, Van Der Poel HG, Zhongchao L, Kontos H, Levasseur JE (1988) Pial arteriolar vessel diameter and CO2 reactivity during prolonged hyperventilation in the rabbit. J Neurosurg 69: 923–927
Nordström C-H, Sundberg G, Messeter K, Schalen W (1989) Severe traumatic brain lesions in Sweden. Part 2: Impact of aggressive neurosurgical intensive care. Brain Injury 3: 267–281
Reilly PL, Adams JH, Graham DI, Jennett B (1975) Patients with head injury who talk and die. Lancet 2: 375–377
Rose J, Valtonen S, Jennett B (1977) Avoidable factors contributing to death after head injury. Br Med J 2: 615–618
Seelig JM, Becker DP, Miller JD, Greenberg RP, Ward JD, Choi SL (1981) Traumatic acute subdural haematoma: Major mortality reduction in comatose patients treated within four hours. N Engl J Med 304: 1511–1518
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Wärme, P.E., Bergström, R. & Persson, L. Neurosurgical intensive care improves outcome after severe head injury. Acta neurochir 110, 57–64 (1991). https://doi.org/10.1007/BF01402049
Issue Date:
DOI: https://doi.org/10.1007/BF01402049