Article Text

Abstract
Background The impact of socioeconomic deprivation and comorbidities on the outcome of patients who require emergency general surgery (EGS) admission is poorly understood. The aim of this study was to examine the effect of deprivation and comorbidity on mortality, discharge destination and length of hospital stay (LOS) in patients undergoing EGS in Scotland.
Methods Prospectively collected data from all Scottish adult patients (aged >15 years) requiring EGS admitted between 1997 and 2016 were obtained from the Scottish Government. Data included age, sex, Scottish Index of Multiple Deprivation (SIMD), 5-year Charlson Comorbidity Index (CCI), whether an operation took place and outcomes including mortality, discharge destination and LOS. Logistic regression was used for the analysis of mortality and discharge destination and Poisson regression was used for LOS.
Results 1 477 810 EGS admissions were analyzed. 16.2% were in the most deprived SIMD decile and 5.6% in the least deprived SIMD decile. 75.6% had no comorbidity, 20.3% had mild comorbidity, 2.5% had moderate comorbidity and 1.6% had severe comorbidity. 78.6% were discharged directly home. Inpatient, 30-day, 90-day and 1-year crude mortality was 1.7%, 3.7%, 7.2% and 12.4%, respectively. Logistic regression showed that severe comorbidity was associated with not being discharged directly to home (OR 0.38, 95% CI 0.37 to 0.39) and higher inpatient mortality (OR 13.74, 95% CI 13.09 to 14.42). Compared with the most affluent population, the most deprived population were less likely to be discharged directly to home (OR 0.97, 95% CI 0.95 to 0.99) and had higher inpatient mortality (OR 1.36, 95% CI 1.8 to 1.46). Poisson analysis showed that severe comorbidity (OR 1.69, 95% CI 1.68 to 1.69) and socioeconomic deprivation (OR 1.11, 95% CI 1.11 to 1.12) were associated with longer LOS.
Discussion Increased levels of comorbidity and, to a lesser extent, socioeconomic deprivation are key drivers of mortality, discharge destination and LOS following admission to an EGS service.
Level of evidence III (prospective/retrospective with up to two negative criteria).
Study type Epidemiological/prognostic.
- epidemiology
- general surgery
- socioeconomic factors
- outcome assessment, health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Health inequalities exist between the most deprived and most affluent populations.1–8 In particular, socioeconomic deprivation is associated with an increased risk of cardiovascular disease,1 poor cognitive function,2 postoperative mortality,3 5–8 morbidity4 6 7 and increased hospital stay7 for both elective and emergency operations. The reasons for this are likely multifactorial, but poorly understood. In addition, it is now recognized that many patients admitted to emergency general services are managed non-operatively,9 and it is not known whether all deprived patients, rather than only those who undergo an operation, are at a health disadvantage. Socioeconomic deprivation is not a hard barrier to healthcare access in the UK, as NHS healthcare is provided free at the point of care regardless of insurance status. However, deprivation may present a barrier to healthcare in other ‘unseen’ ways, which could lead to poorer outcomes.
Outcomes are also affected by comorbidities. Multiply comorbid patients undergoing emergency general surgery (EGS) procedures have an increased mortality risk,10 which is exacerbated if the patient undergoes a high-risk EGS procedure.8 Frailty is a predictor of perioperative complications, length of hospital stay,11 mortality, institutional discharge and cost12 in patients undergoing EGS. Although they are not synonymous, frailty and comorbidity are related in that frail patients are likely to be more comorbid.12
Although the impact of socioeconomic deprivation and comorbidity has been established, their combined impact is not known. We hypothesized that deprivation and comorbidity could have an additive or multiplicative effect on adverse outcomes. The aim of this study was to examine the impact of deprivation and comorbidity on mortality, discharge destination and length of hospital stay in patients undergoing EGS in Scotland.
Methods
This was a population-based retrospective cohort study.
Case definition and data sources
Data were obtained of all Scottish EGS admissions between 1997 and 2016 involving persons aged >15 years. These data were sourced by querying the prospectively collected database held by the Information Services Division (ISD) of the Scottish Government,13 to identify all patients within our study timeframe who were admitted as an emergency to a Scottish hospital under the care of a consultant (attending) general surgeon. Patients who are over 15 years of age in Scotland are admitted under adult general surgery services. The conditions treated by general surgeons in Scotland include undifferentiated abdominal pain, oesophago-gastric, hepatico-pancreatico-biliary, colorectal and acute breast conditions, and abdominal trauma. This includes conditions such as choledocholithiasis, diverticulitis and acute pancreatitis which may, in other countries, be managed by doctors other than surgeons. Surgeons in smaller hospitals may also treat patients with urological conditions, minor head injuries and thoracic trauma. ISD data are coded using the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). Anonymised data were hosted by the University of Aberdeen Data Safehaven in an Excel database (Microsoft Corporation, Redmond, Washington, USA).
The Scottish Index of Multiple Deprivation (SIMD) is a tool created by the Scottish Government which identifies small area concentrations of multiple deprivation in a consistent way. It identifies areas of poverty, inequality and decreased opportunity based on income, employment, education, health, access to services, crime and housing domains. It divides Scotland into 6976 data zones, each with a roughly equal population (approximately 760 residents per data zone).14
Extracted data for each EGS admission included patient age, sex, SIMD deciles (1=most deprived; 10=least deprived), 5-year Charlson Comorbidity Index (CCI),15 whether patients had a surgical operation and outcome of the admission including mortality (inpatient, 30-day, 90-day and 1-year), discharge destination and length of hospital stay (LOS). CCI was described as no comorbidity (CCI 0), mild comorbidity (CCI 1 to 2), moderate comorbidity (CCI 3 to 4) and severe comorbidity (CCI >4), in a similar fashion to several other publications.16 17
Analysis of data
Binomial logistic regression was used to analyse discharge destination and inpatient, 30-day, 90-day and 1-year mortality. Poisson regression was used to analyse LOS. Statistical analysis was repeated for the subgroup of patients who underwent a surgical operation. All statistical analyses were conducted using SPSS (IBM Corporation, Armonk, New York, USA).
Ethical approval
This project was registered with the research governance department of NHS Grampian and the University of Aberdeen, and approved by the Public Benefit and Privacy Panel (PBPP) of NHS Scotland (Ref 1617–0207).
Results
Demographics
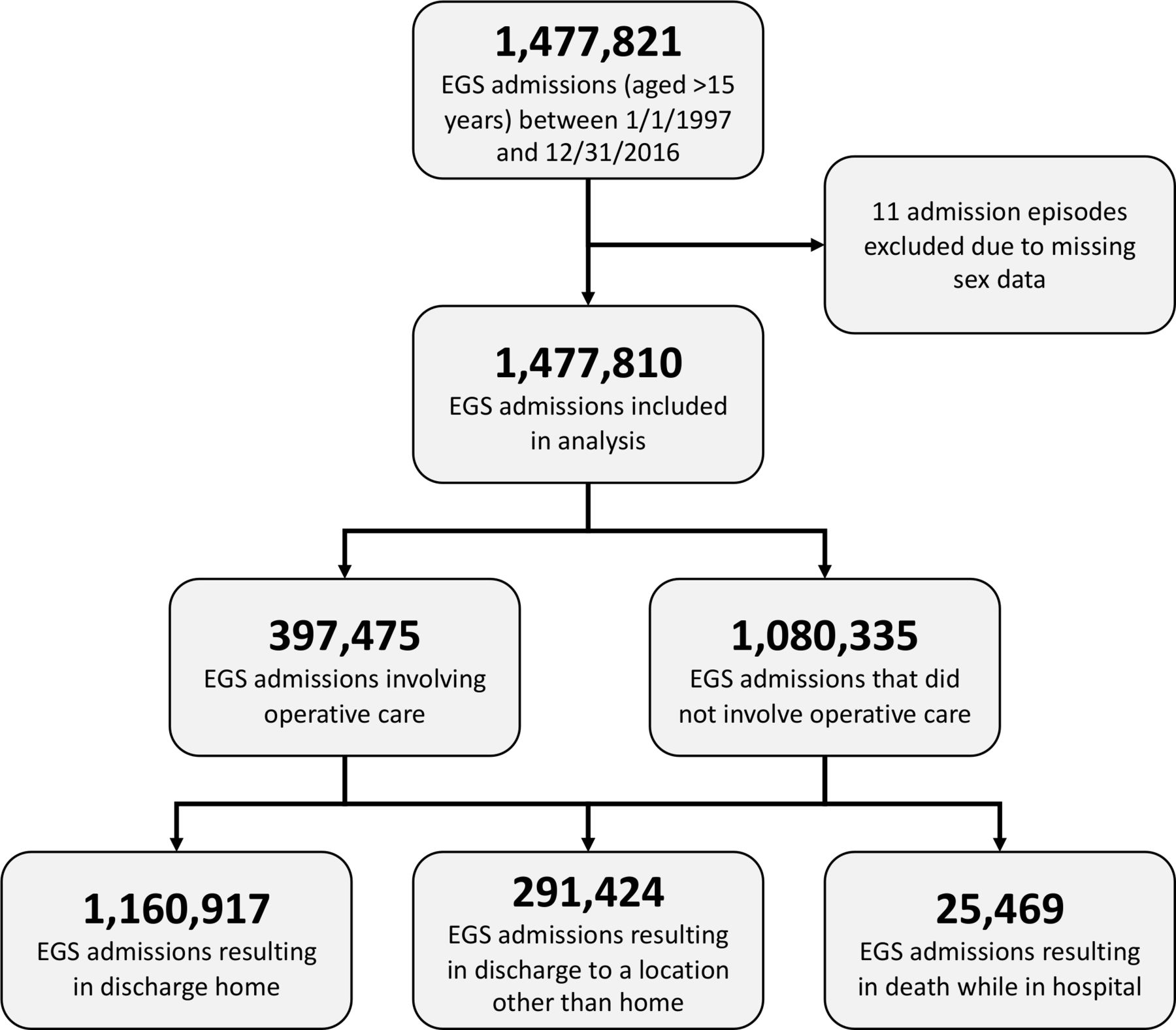
A total of 1 477 810 EGS admissions meeting our inclusion criteria were identified (figure 1); 237 824 (16.2%) were in SIMD decile 1 (most deprived) and 81 830 (5.6%) were in SIMD decile 10 (least deprived) (table 1). Of the total, 1 116 808 (75.6%) had no comorbidity (CCI 0), 299 657 (20.3%) had mild comorbidity (CCI 1 to 2), 37 558 (2.5%) had moderate comorbidity (CCI 3 to 4) and 23 787 (1.6%) had severe comorbidity (CCI >4).
{kind=link}
Flow diagram of included and excluded cases. EGS, emergency general surgery.
Demographics of all patients admitted for EGS in Scotland 1997 to 2016
The subgroup of patients who underwent an operative procedure totalled 397 475 cases (26.9% of all admissions); 55 368 (14.0%) were in SIMD decile 1 and 26 043 (6.6%) in SIMD decile 10 (table 2). A total of 299 344 (75.3%) had no comorbidity, 82 146 (20.7%) had mild comorbidity, 9673 (2.4%) had moderate comorbidity and 6312 (1.6%) had severe comorbidity (table 2). Detailed breakdowns of admissions by diagnoses have been published in our previous works, including trends over the past 20 years.9 18
Demographics of patients admitted for EGS in Scotland who underwent an operative procedure 1997 to 2016
Outcomes
A total of 1 452 341 (98.3%) patients were discharged from hospital and 25 469 (1.7%) died in hospital (table 1); 1 160 917 patients (78.6%) were discharged home, while 291 424 (19.7%) were discharged from the acute care setting to a non-home environment (table 1). The overall 30-day, 90-day and 1-year crude mortality rates were 3.7%, 7.2% and 12.4%, respectively (table 1). These figures remained unchanged depending on SIMD decile, but were greatly affected by comorbidity.
Among the operative subgroup, 319 970 (80.5%) of patients were discharged directly home and 77 505 (19.5%) were not (table 2). A total of 392 366 (98.7%) were discharged from hospital and 5109 (1.29%) died in hospital (table 2). Overall 30-day, 90-day and 1-year crude mortality rates were 3.2%, 6.7% and 11.4%, respectively (table 2). As with the overall cohort of admissions, the outcomes of operative patients were largely affected by CCI but not by SIMD (table 2).
Combined analysis
This finding is corroborated by online supplementary table 1, which shows that crude mortality and mortality risk ratios are not affected by deprivation, but are greatly affected as comorbidity increases. When the referent is set to no comorbidity (CCI 0) and the least deprivation level (SIMD 10), admissions with CCI >4 had an inpatient mortality risk 16 to 23 times and 1-year mortality risk 90 to 96 times that of the comparison group (online supplementary table 1). Similarly, for the subgroup of admissions which included a surgical operation, admissions with CCI >4 had an inpatient mortality risk 24 to 41 times (online supplementary table 2) and 1-year mortality risk 156 to 173 times that of the referent group (online supplementary table 2).
Supplemental material
Supplemental material
Statistical analysis
Logistic regression analyses showed that, compared with those with CCI 0, admissions with CCI >4 were less likely to be discharged home (OR 0.376, 95% CI 0.367 to 0.387) and had higher inpatient mortality (OR 13.741, 95% CI 13.094 to 14.42), 30-day mortality (OR 14.085, 95% CI 13.594 to 14.594), 90-day mortality (OR 14.679, 95% CI 14.258 to 15.112) and 1-year mortality (OR 9.849, 95% CI 9.586 to 10.12) (table 3).
Logistic regression analyses for discharge home and inpatient, 30-day, 90-day and 1-year mortality
Compared with the most affluent population (SIMD 10), the most deprived population (SIMD 1) were less likely to be discharged home (OR 0.974, 95% CI 0.954 to 0.994) and had higher inpatient mortality (OR 1.363, 95% CI 1.276 to 1.456), 30-day mortality (OR 1.278, 95% CI 1.221 to 1.338), 90-day mortality (OR 1.192, 95% CI 1.152 to 1.233) and 1-year mortality (OR 1.113, 95% CI 1.084 to 1.142) (table 3). Similar results are seen among those who had an operation (table 3).
Poisson analysis showed that, compared with those with CCI 0, admissions with CCI >4 had longer LOS (OR 1.685, 95% CI 1.677 to 1.694), and compared with the most affluent population (SIMD 10), the most deprived population (SIMD 1) also had a longer LOS (OR 1.11, 95% CI 1.11 to 1.12) (table 4). A similar effect occurred among admissions of patients who had an operation (table 4).
Poisson regression analyses for length of hospital stay
Discussion
This study has demonstrated, using population-level data, that increased levels of comorbidity and, to a lesser extent, socioeconomic deprivation significantly affect outcomes of EGS admissions in a free at the point of care healthcare system. Not only is this a novel finding, it is methodologically unique from a public health perspective in that we examined the whole population of EGS admissions over 20 years instead of examining the impact on a specific diagnosis or operation over a shorter time period.
These findings have implications for public health policy and service delivery planning. Patients with multimorbidity are at increased risk of in-hospital, short-term and medium-term mortality.19 They are also at higher risk of discharge to a non-home environment. Early identification of those individuals who are likely to require further care needs may need to be explored in order to ensure patient movement through the acute sectors of NHS care. Our data also show that the need for further support structures is greatest in the deprived regions.
There are also clinical applications from this work: clinicians need to better appreciate (and quantify) the impact that comorbidity and, to a lesser extent, socioeconomic deprivation have on LOS, discharge destination and both in-hospital and post-discharge mortality. This pertains to the very nature of patient–provider discussion in setting the expectations for length of hospital admissions, the likelihood of being discharged home directly or the likelihood of inpatient or post-discharge death, regardless of operative intervention. While it is not possible to suggest a 'comorbidity threshold' for involving services such as physiotherapy, occupational therapy, social work or geriatrics, clinicians should be aware that, compared with patients with no comorbidity, patients with minor comorbidity (CCI 1 to 2) are half as likely to be discharged home (all patients OR 0.57, operative patients OR 0.49), and patients with major comorbidity (CCI >4) are only one-third as likely to be discharged home (all patients OR 0.38, operative patients OR 0.37) (table 3). Interestingly, the number of patients who are discharged home is the same in both the operative and non-operative groups. This finding suggests that the barriers to discharge are not related to treatment.
Other studies have shown associations between socioeconomic deprivation and health outcomes. The Whitehall studies of British civil servants identified increased morbidity and cardiovascular risk among those working in lower employment grades, and this effect was observed to be sustained for over a decade.1 Packard et al showed that socioeconomic adversity in children negatively affects their health and cognition in adult life.2 Overall mortality was higher in the deprived population compared with the affluent population (HR 1.36, 95% CI 1.09 to 1.69) for patients who underwent resection for colorectal cancer in Scotland between 1991 and 1994.3 Deprivation was associated with increased major and minor complications following ileostomy reversal in a Scottish population.4 Socioeconomic deprivation was independently associated with higher mortality rates after kidney transplantation, with the least deprived having reduced 5-year mortality (HR 0.65, 95% CI 0.54 to 0.77).5 Taylor et al showed that, in patients undergoing coronary artery bypass graft, deprivation was independently associated with increased risk of postoperative myocardial infarction, stroke, death and prolonged hospital stay.6 Wrigley et al showed that socioeconomic deprivation was adversely associated with survival in patients with colorectal cancer,7 with HR for mortality from colorectal cancer in the most deprived areas of 1.12 (95% CI 1.00 to 1.25) and all-cause mortality 1.18 (95% CI 1.07 to 1.30). Symons et al showed that high-risk EGS patients with Carstairs score 5 (most deprived) compared with Carstairs score 1 (least deprived) had a higher 30-day mortality risk with OR 1.22 (95% CI 1.18 to 1.27).8
The relatively small effect of deprivation on outcomes may be explained by Scotland’s single-payer healthcare system. Healthcare is delivered free at the point of care, including primary care (general practitioners) and secondary/tertiary care (hospital specialists), both in the elective and emergency setting. This may reduce some financial barriers to receiving healthcare, thereby increasing access for those who in other healthcare systems may struggle to receive emergency medical care.
There is evidence in the literature that comorbidities affect the outcome of patients undergoing EGS, but most focus on patients who have had operative procedures. Patients undergoing EGS procedures who had a higher CCI had increased 30-day mortality postoperatively (adjusted OR 1.39, 95% CI 1.11 to 1.73).10 Another study showed that this effect was even greater for patients undergoing high-risk EGS procedures, as those patients with CCI >2 had a higher 30-day mortality (OR 2.61, 95% CI 2.56 to 2.67).8 Many studies have focused on elderly EGS patients, and concluded that frailty was a significant predictor of outcomes including perioperative complications, length of hospital stay,11 mortality, institutional discharge and cost.12 Frailty and comorbidity are related, in that frail patients have a higher CCI score,12 but they are not synonymous. Recent efforts have focused on these factors; in particular, the National Emergency Laparotomy Audit (NELA) identified that nearly half of all emergency laparotomies are performed on patients over 70, that their mortality rate, LOS, comorbidity and frailty are much higher than younger patients, and that only 3% of hospitals provide regular proactive assessments from geriatricians.20–22 Similarly, in Scotland, 49% of emergency laparotomies were performed in patients aged >65 years and 16% of these were frail, scoring >4 in the Rockwood Clinical Frailty Score,23 and it has been suggested that we build 'clinical relationships with geriatricians to develop targeted frailty pathways'. The UK-wide Emergency Laporatomy and Frailty study reported that, of patients aged >65 years undergoing laparotomy, 20% are frail, which is associated with increased postoperative mortality, morbidity, length of critical care stay and LOS.24
The information collected at routine assessment at time of admission (the ‘clerking in’ of patients) could be better used to inform the likely hospital course. An area of future research could be to develop a prediction score at admission based on factors which predict likelihood of various outcomes, such as LOS, discharge destination and mortality. This has been done for perioperative mortality (P-POSSUM)25 and could have clinical relevance—for example, to trigger patients’ needs assessments (physiotherapy, occupational therapy, social care requirements), review by a geriatrician, or early discussions/decisions about ceilings of care with the patient and their families.
We defined EGS as those patients who were admitted to a Scottish hospital under the care of a consultant (attending) general surgeon.9 18 19 26 There have been other methods of defining EGS,27 however this is the most pragmatic definition in the context of the UK as it defines the actual service delivered instead of only including the patients whose coded diagnosis at discharge falls within the remit of the general surgical specialism (‘ideal’ definition). This is an important distinction for two reasons: (1) because the nature of EGS service is such that diagnoses are often dependent on laboratory and radiological services, which may take time, and thus many admissions result in diagnoses which would not normally be looked after by general surgeons; and (2) clinical resources should be allocated based on actual demand, not ideal situations.
This study has strengths and limitations. Its greatest strength is the large number of hospital episodes included. The population-wide data have great advantages in that there are very few missing data, but there is also a lack of granularity. This limited the variables which could be controlled for, and thus limited interpretations of findings. For example, there is no information on the specific comorbidities which contribute to make up the CCI, so for any individual admission we do not know whether the outcome was influenced by specific comorbidities (cardiac, respiratory, immunological, extremes of body mass index, frailty) or other factors including presenting physiology, case severity, or clinical and radiological findings. Therefore, although there is little bias introduced in the dataset and the confidence intervals are narrow given the very large sample size, detailed associations related to underlying conditions could not be determined. There is also a risk of confounding factors which could not be controlled for, given the limited breadth of the dataset. Another limitation is that SIMD describes deprivation within post code regions, therefore not all individuals within a particular data zone will have the same characteristics. Data providers quality assure data for all indicators before providing them to the Office of the Chief Statistician and Performance, which then performs further checks on indicators and domains.14 Data are correlated with previous years, investigated and considered for amendment if they have changed dramatically.14 Therefore, despite not being tailored for the individual, SIMD is likely the most reliable method of characterising deprivation in Scotland. As a multicenter study, it would have been pertinent to study clustering effects by facility, but we did not have a facility variable or field in the database so it could not be performed. Further work on a representative sample of these patients using more detailed data could provide prognostic information at the point of admission, augmenting the prognostic work resulting in the NELA score and P-POSSUM score for emergency laparotomy.22 25
The generalizability of these results may be wide. Although the data came from a single nation (Scotland), it was a population-wide sample over the course of 20 years, with very few missing data, and therefore may compare to similar populations (highly developed Western nations). Lastly, because we included data from the last 20 years, if there had been a change in the direction of any effect over time the conclusions generated may be misleading.
In conclusion, increased levels of comorbidity and, to a lesser extent, socioeconomic deprivation significantly adversely affects EGS outcomes including mortality, discharge destination and length of hospital stay. Further work is warranted to determine whether prognostic scoring at EGS admission could be developed, which can help guide treatment pathways for patients.
Acknowledgments
The authors would like to thank Information Services Division of the Government of Scotland for access to the database, and to SafeHaven University of Aberdeen for hosting the data.
References
Footnotes
Presented at Presented at the 78th annual meeting of the American Association for the Surgery of Trauma, Dallas Texas on September 18-21, 2019, Sheraton Dallas Hotel, Dallas, Texas, USA.
Contributors JMW, GR and JOJ designed the study, requested the data and completed ethics application. JMW, GR, RLG and JOJ performed the analysis and interpretation of the results. JMW wrote the manuscript. JMW, GR, RLG and JOJ provided critical edits of the manuscript. JMW, GR, RLG and JOJ approved the manuscript prior to submission for publication.
Funding NHS Grampian Endowment funds were granted to allow retrieval and secure access to the data.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. Data held by Information Services Division of the Government of Scotland.