Article Text

Abstract
Introduction Since their release in 2017, standing electric motorized scooters (eScooters) have risen in popularity as an alternative mode of transportation. We sought to examine the incidence of injury, injury patterns, prevalence of helmet and drug and alcohol use in eScooter trauma.
Methods This was a multi-institutional retrospective case series of patients admitted for injuries related to operation of an eScooter following the widespread release of these devices in September 2017 (September 1, 2017 to October 31, 2018). Demographics, drug and alcohol use, helmet use, admission vitals, injuries, procedures, hospital and intensive care unit length of stay (LOS), death, and disposition were analyzed.
Results 103 patients were admitted during the study period, and monthly admissions increased significantly over time. Patients were young men (mean age 37.1 years; 65% male), 98% were not wearing a helmet. Median LOS was 1 day (IQR 1–3). 79% of patients were tested for alcohol and 48% had a blood alcohol level >80 mg/dL. 60% of patients had a urine toxicology screen, of which 52% were positive. Extremity fractures were the most frequent injury (42%), followed by facial fractures (26%) and intracranial hemorrhage (18%). Median Injury Severity Score was 5.5 (IQR 5–9). One-third of patients (n=34) required an operative intervention, the majority of which were open fixations of extremity and facial fractures. No patients died during the study. The majority of patients were discharged home (86%).
Conclusion eScooter-related trauma has significantly increased over time. Alcohol and illicit substance use among these patients was common, and helmet use was extremely rare. Significant injuries including intracranial hemorrhage and fractures requiring operative intervention were present in over half (51%) of patients. Interventions aimed at increasing helmet use and discouraging eScooter operation while intoxicated are necessary to reduce the burden of eScooter-related trauma.
Level of evidence Level IV.
- accidents
- alcohol and trauma
- head injury
- fractures
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The appearance of new means of transportation when adopted by large numbers is often followed by far-reaching changes in commerce, infrastructure, and legislation. While motorized stand up or kick scooters were first introduced as early as 1915,1 they have only recently gained mass appeal and widespread usage with the introduction of rentable dockless electric motorized kick scooters known as eScooters. Advertised as a cheap, ecologically friendly alternative mode of transportation, multiple companies have released these vehicles for rent in over 65 cities within the USA alone and have garnered hundreds of millions of dollars in investments since first appearing in 2017. The reaction at a municipal and legislative level has been mixed. Previous California law required helmet use; however, amendment AB-2989 was signed into law on September 19, 2018 and eliminated this requirement for drivers 18 years of age and older and allowed eScooters onto roads with speed limits up to 35 mph. Already a source of regulatory contention with partial or complete bans on eScooters in cities such as Santa Monica, Denver, San Francisco, and San Diego, little is known about the public health risk of this newly popularized form of transportation. With state and local governments rapidly responding to this shakeup of the transportation industry, there is a strong need for safety data to help guide this legislation. We therefore sought to examine the incidence of injury, prevalence of helmet use, presence of drug and alcohol intoxication, and injury patterns among patients admitted for eScooter-related trauma.
Methods
After institutional review board (IRB) approval, the trauma registries from three Level I trauma centers were queried for all patients admitted for injuries related to operation of an eScooter between September 1, 2017 and October 31, 2018. Chart review was performed to confirm injuries were related to eScooters. Injuries related to motorized wheelchairs or mobility devices, dirt bikes, or mopeds were excluded. Demographics, admission vitals, injuries, injury severity, procedures, intensive care unit (ICU) and hospital lengths of stay (LOS), disposition, and mortality were abstracted. Data analysis was performed using STATA/MP Version 14.2 (StataCorp, College Station, TX). Descriptive statistics included percentages and frequencies. Continuous variables were described using mean±SD if normally distributed and median (IQR) if not. Univariate analysis used the Pearson χ2 test for categorical variables and the t-test or Mann–Whitney test according to distribution as appropriate. Spearman’s rank correlation test was performed to analyze trend of non-parametric continuous variables. Multivariate analysis was used to analyze risk of needing surgical intervention during hospitalization.
Results
A total of 103 patients were admitted during the study period. Monthly admissions increased over time (figure 1), with the highest number (n=43) seen in October 2018. A strong upward trend in admissions over time was confirmed using Spearman’s correlation coefficient (0.934, p<0.0001).
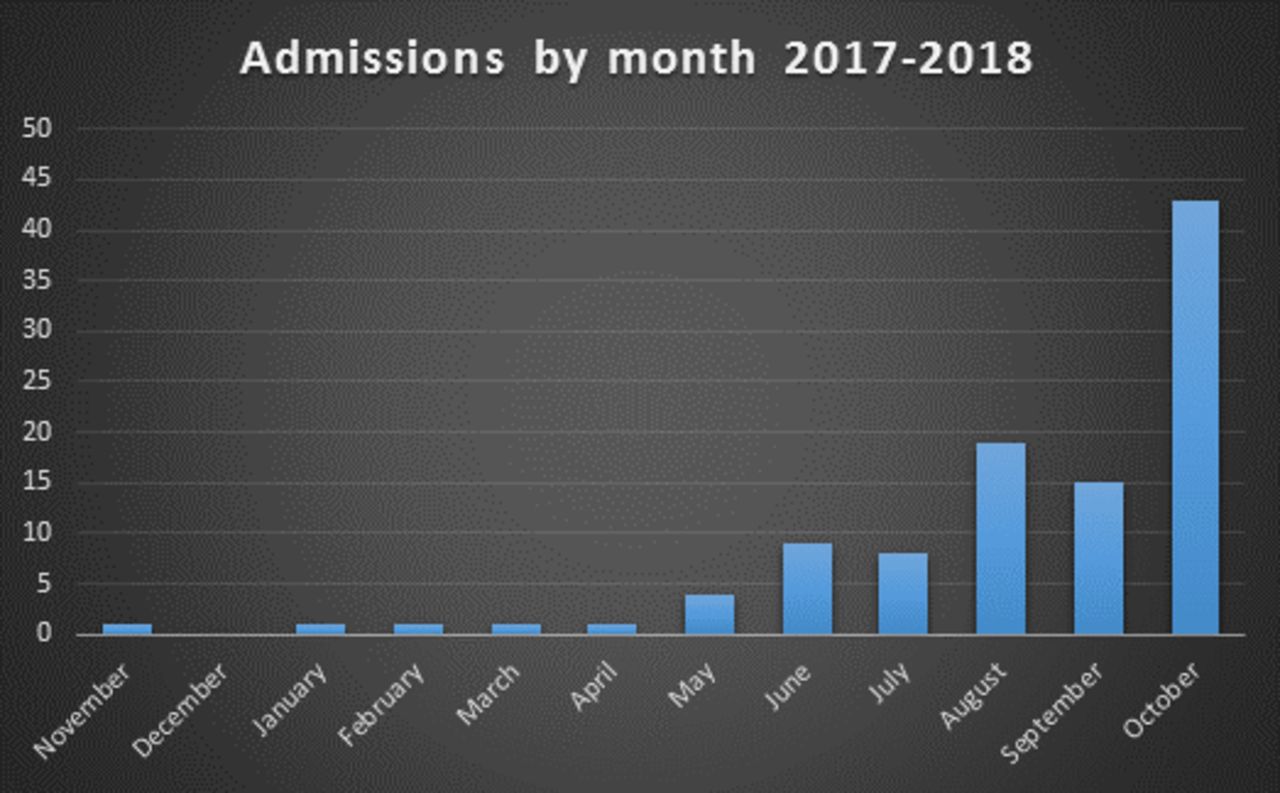
Monthly eScooter-related trauma admissions demonstrating strong trend toward increasing admissions over time (Spearman’s correlation coefficient 0.934, p<0.0001).
The average age was 37.1 years, with the majority (62%) in the 20 to 40 year age range. The fastest growing population was age 20 to 40 years followed by age 41 to 60 years (figure 2).

{kind=link}
{kind=link}
eScooter-related trauma admissions stratified by age group.
Sixty-five percent of patients were male. The majority of patients were non-Hispanic white (66%). Data regarding helmet use was missing for five (5%) patients; however, among those where helmet use was documented, the vast majority of patients (98%) were not wearing a helmet. Seventy-nine percent of patients were tested for alcohol at the time of admission, of which 48% were legally intoxicated with a blood alcohol level >80 mg/dL blood. The median blood alcohol level in intoxicated patients was 199 mg/dL blood (IQR 160–256). Sixty percent of patients had a urine toxicology screen performed at the time of Foley placement or first void, of which 52% were positive. The most common substances on urine toxicology were tetrahydrocannabinol (THC) at 32%, followed by methamphetamine and amphetamines at 18% (table 1).
Demographics and outcomes of patients involved in eScooter accidents
Median Injury Severity Score (ISS) was 5.5 (IQR 5–9) and 42% of patients had at least moderate (ISS >8) injuries. Extremity fractures were the most frequent injury, occurring in 43 patients (42%), of which four were open fractures. Extremity Abbreviated Injury Score (AIS) ≥3 was present in 8% of the study population. Lower extremity fractures of the tibia, fibula, and medial and lateral malleoli were the most frequent. Three patients presented with femur fractures and one with a pelvic fracture. Upper extremity fractures of the clavicle, scapula, radius, and ulna were also common (table 2). Among patients with extremity fractures, 23 (53%) required surgery with the majority being open reduction internal fixations and eight requiring intramedullary nails.
Injuries and injury severity following motorized scooter accidents
Facial fractures were the second most common injury found in this population, occurring in 27 patients (26%) of whom eight (30%) had mandible fractures. The majority of fractures were minor with only 1% of patients in the study with a face AIS ≥3. Among patients with facial fractures, six (22%) required surgical repair.
Intracranial hemorrhage (ICH) occurred in 19 patients (18%). Median Glasgow Coma Score (GCS) at arrival was 15 (IQR 14–15); one patient presented with GCS of 3. The most common ICH pattern was subarachnoid hemorrhage (SAH); 15 patients (15%) had a head-AIS ≥3 (table 2). No patients required craniotomy or craniectomy. In addition, 17 patients (16.5%) were diagnosed with concussion without ICH.
Other significant injuries included one hemothorax requiring chest tube placement, two splenic lacerations (one Grade 1, one Grade 2), one Grade 2 renal injury, and one multi-level cervical spine injury.
Thirty-four patients (33% of the total study population) required an operative intervention, with the majority of procedures being open repair of fractures. On multivariate analysis adjusting for age, ICH, illicit drugs, alcohol, helmet use, presence of facial and extremity fractures, only THC use (OR 8.76, p=0.043) and extremity fracture (OR 9.53, p=0.012) were associated with a higher risk for requiring surgical procedures (table 3).
Multivariate logistic regression for factors associated with need for surgical procedures (pseudo R2=0.291)
Intubation was required in three patients, median ventilator days 8 (IQR 4–21). Average hospital LOS was 3.1±6.9 days, median LOS 1 day (IQR 1–3). Eight patients (8%) required ICU admission; for these, the median ICU-LOS was 2.5 days (IQR 2–4.5). Six patients (7%) required transfer to long-term acute care, skilled nursing, or rehabilitation facilities. The majority of patients (86%) were discharged home, two of whom (2%) required home health assistance. Seven patients left against medical advice and disposition was missing for one patient. No patients died during the study period.
Discussion
The almost overnight introduction of eScooters to major urban areas around the USA has already begun to have effects on transportation patterns and legislation. Not all new transportation technologies rise to the level of public health concerns; the Segway, for example, has had only 135 accidents reported in the literature for the last 17 years.2 eScooters, however, have been adopted at an unprecedented rate. Less than a year after their introduction, 3.6% of all US adults had ridden an eScooter,3 and by the end of 2018 two of the largest eScooter companies—Lime and Bird—reported a combined 36 million rides and are available in over 100 communities spanning five continents.4 5
These devices combine the size of a child’s push-scooter with the speed of an electric bicycle, and the injury mechanisms associated with them are largely unknown. A few studies investigating trauma related to motorized scooters, bicycles, and mopeds in Europe and Israel where such modes of transportation have become increasingly popular demonstrated a significant increase in the number of traumas related to motorized scooters and bicycles over time.6–8 Similar to the European and Israeli studies, the current study also found a significant increase in eScooter-related trauma admissions over time as the popularity and availability of the devices have increased.
A recent study published by Trivedi et al was the first to describe trauma associated specifically with eScooters in the USA, and focused on eScooter-related visits to two urban emergency departments in Southern California.9 Similar to the Trivedi study, we found that those injured in eScooter accidents were most likely to be men in their 20s to 40s. Despite similar age and gender distributions, the rates of intoxication in our study (48% for alcohol, 52% for other illicit substances) were significantly higher than the Trivedi study at 4.8%. The rate of screening was not reported in the prior study and may have been significantly lower than our relatively high screening rate (79% for alcohol, 60% for other illicit substances). The rate of intoxicating substances present in the current study is also notably higher than other previous studies of bicycle (15% to 20%)10 11 and skateboard (18% to 28%)12 13 accidents.
Both our study and that by Trivedi et al found that helmet use was exceedingly rare, and the reported rates of helmet use (current 2%, Trivedi 4.4%) were significantly lower than previous studies of bicyclists (16% to 39%)10 11 and skateboarders (~50%)14 15 in the USA. It is likely that the low rates of helmet use are related, in part, to the lack of legislation requiring helmet use with these devices. It is also interesting to note one prior study by Lustenberger et al of helmet use among skateboard injuries which found a significant decrease in rates of helmet use with increasing age. In this study the age group most consistent with the current study (>16 years) had the lowest rates of helmet use (4.4%).16 Page et al also found adults were much less likely than children to use helmets, as were males compared with females, when studying bicyclists, skateboarders, and rollerbladers,15 both of which were prevalent in the current population where the majority of patients were adult males. Helmet use has been shown to significantly decrease the risk of traumatic brain injury in motorcycle,17 bicycle,18 19 and skateboard16 accidents. After legislation was changed in Michigan removing mandatory helmet requirements for motorcycle riders, helmet use decreased dramatically and crash mortality increased fourfold.17 The effect of helmets in preventing head injury in eScooter riders is unknown, and we were unable to draw any meaningful conclusions in our study due to lack of helmet use (only two people) in the current study population. However, given prior protective effects of helmets with other types of powered and non-powered vehicles, helmet use is likely to have a beneficial effect in this population as well. Already several of the rental companies offer either free helmets or helmets at a significant discount on request. There are also collapsible helmets that may make helmet use more feasible for the occasional rider or tourist. This topic will need some further study to determine the subtypes of eScooter user (commuter, recreational, intermittent) and the best way to distribute, increase, and enforce helmet use before formal policy recommendations are made. Future laws may need to target helmet use in specific operational circumstances (on road, off road, in park/recreational areas, etc) or specific populations (children under 18 as for bicycles and skateboards).
The most common injuries found in the current study were extremity fractures, facial fractures, and head injuries, similar to Trivedi et al. 9 However, the percentage of patients with these injuries was markedly higher in our study than in the study by Trivedi e t al (extremity fractures 42% vs 31.1%, facial fractures 26% vs 5.3%, and ICH 18% vs 2.2%). ICU admission was also much higher in the current study (8% vs 0.9%). Not reported in the prior study but present in a significant number of patients in the current study was the need for operative intervention (33%). The increased frequency and severity of injury found in this study is likely a product of multiple factors. Using patients only from Level 1 trauma centers may skew our data by excluding many of the less severely injured patients who were triaged to lower level trauma centers and non-trauma centers. Additionally, the current study included only patients who were triaged as major traumas or those requiring hospital admission, in contrast to the Trivedi study where only 8.8% of patients were major trauma activations and the majority of whom (93.9%) were discharged home from the Emergency Department. We also observed vastly higher rates of alcohol or drug intoxication, which have previously been linked to increased injury severity and worse outcomes with other injury mechanisms like motorcycle crashes.20
Given the unique nature of the eScooter as a powered personal transportation device, it is difficult to determine an appropriate comparator mechanism of injury. Similarities can be made to skateboards in terms of design and stability. Two analyses of skateboard-related injuries by Lustenberger et al and Tominaga et al both found extremity fractures and ICH to be common injuries.12 16 The injury pattern of eScooters in the current study appears similar to that of skateboards, with the most common injuries being extremity fractures (42%), and with ICH occurring in 18% of patients. Compared with skateboard studies where 30% to 60% of patients were under 17 years of age, the majority of patients in our study were >20 years old. Interestingly, both prior skateboard studies found older patients to be more severely injured, less likely to wear a helmet, and more likely to have a traumatic brain injury compared with their younger counterparts.12 16
It would appear that there is a subset of adult male skateboarders who are more likely than their pediatric counterparts to be severely injured, and are particularly at risk for ICH. This subpopulation appears to be more likely to engage in high-risk behaviors such as operating their devices intoxicated, in traffic, and without helmets. eScooters may be particularly attractive to this group of patients. Studies in China have found that eScooter riders are also more likely to exhibit risky driving such as riding in traffic lanes and riding against traffic compared with bicycle and electronic bicycle riders.21 Our current study also supports this hypothesis, consisting primarily of men aged 20 to 40 years with a high rate of alcohol use, drug use, and lack of helmet use. These patients presented with a high rate of head (ICH, concussion, and facial fractures) and extremity injuries which resulted in a significant use of medical resources, with 8% requiring ICU admission, 33% requiring surgery, and 9% requiring transfer to long-term care facilities or home health resources.
Limitations of this study include the retrospective nature which precludes us from drawing conclusions on causal relationships. We are also significantly limited by the small number of patients to date and hope that future multi-institutional studies can overcome this limitation and allow for more robust conclusions to be drawn. Furthermore, in order to meet the inclusion criteria, all patients in this study required admission or a formal Trauma Service consultation; as such, there is a significant selection bias toward more severely injured individuals. We may be missing a significant population of patients with more minor injuries or injuries that could be treated in a delayed fashion who require medical attention and resources but are treated and discharged from the Emergency Department or Urgent Care facilities without requiring hospitalization or Trauma Service consultation. Lastly, we lack access to data on the volume, location, and patterns of eScooter usage and so were unable to correlate volume of usage, mileage, or operator experience to risk of injury or injury severity. We hope that increased communication and cooperation between injury and epidemiology researchers and the eScooter companies will aid in future research on this important injury prevention topic.
As the popularity of alternate modes of transportation continues to rise, eScooter-related injuries are likely to increase as well. We found very few patients wearing helmets while riding eScooters and the majority of patients were intoxicated on alcohol or other illicit substances. Resource utilization in terms of H-LOS, ICU-LOS, and the need for operative procedures was high. To date there are no data on eScooter helmet laws and their effectiveness, nor is there is there much known on the impact of enforcing traffic laws against driving under the influence on eScooter operators. Early research into the safety and injury patterns of eScooters is vital to guide the public and legislators on injury prevention strategies for this evolving mode of transportation.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.References
Footnotes
Contributors LMK, EW, CVB, VB, EMC and JD conceived the study, created the study design, performed the analysis and interpretation, authored and revised the manuscript. BJE, KDC and JB all contributed to data acquisition.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.