Article Text

Abstract
Background Owing to the potential risks associated with missed injury, many blunt trauma patients with suspected cervical spine injury undergo some form of imaging technique which has progressed from primarily using plain radiography to relying on CT. Recently, studies have shown that in certain situations, adding MRI may improve the diagnostic accuracy over solely relying on CT.
Methods Retrospective study of 3468 adult blunt trauma patients at a level I trauma center of which 94 with an initial negative CT scan underwent subsequent MRI. These 94 patients were classified as reliable or unreliable for examination; coded as either having a positive or negative MRI result; and assessed for a change in management.
Results Of the 94 patients in the study population, 69 (73.4%) were deemed reliable and 25 (26.6%) deemed unreliable for examination. Overall, 65 (69.1%) patients had a positive MRI result—49 (71.0%) reliable and 16 (64.0%) unreliable—with some patients testing positive for more than one finding. There was no significant difference in positive MRI rates between reliable and unreliable patients. None of the 29 patients who had negative MRI had a change in management, while 31 of the 65 (47.7%) patients with positive MRI did have a change in management of either continued cervical collar immobilization or neck surgery.
Conclusions The use of CT scans should be continued as the primary imaging technique for patients with suspected cervical spine injuries. In cases where obtundation or clinical suspicion exists for a false-negative CT scan, MRI should be considered as a supplement and should not be rejected solely based on the negative result of the CT.
Level of evidence Level IV.
- cervical spine
- blunt trauma
- CT scan
- MRI
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Protocols for clearing the cervical spine (c-spine) in blunt trauma patients depend on many factors. Alert or non-obtunded patients—often defined as patients with a Glasgow Coma Scale (GCS) score 14 or higher—may be cleared by clinical examination only, thus avoiding imaging.1 ,2 However, some trauma centers perform c-spine imaging of all awake and alert blunt trauma patients, independent of the outcome of clinical examination.3 Owing to their inability to provide feedback to the treating physician, obtunded patients routinely receive some form of imaging technique and are cleared based on a negative result.1 ,2 Clearance of the c-spine has received remarkable attention in the literature over the past decade. Recently, the Eastern Association for the Surgery of Trauma (EAST) issued guidelines that recommended cervical collar removal in the obtunded adult patient after a negative high-quality c-spine CT scan only.4 In this recommendation, EAST strongly emphasized on the high negative predictive value of high-quality CT imaging in the presence of a critically important unstable c-spine injury. However, they also noted that their conclusion was based on ‘very’ low-quality evidence and the high costs of MRI.
Controversy remains on the role of MRI in clearing the c-spine of a blunt trauma patient suspected of having injury despite a negative CT scan.4 Certainly, missed unstable spinal injuries are associated with potentially devastating neurological compromise. Balanced against this is the reality that the majority of patients have a stable spinal column and that extensive imaging is expensive and delays mobility and disposition.5 Some authors have concluded that in obtunded trauma patients with negative CT of the c-spine, obtaining an MRI does not appear to significantly alter management.6 Others advocate that MRI continues to play a vital role in the work-up of such patients.7 ,8 The logic behind obtaining MRI in obtunded patients is to avoid missed injuries not detected by CT. In some cases, the added expense of MRI may be justified by detecting additional c-spine injuries and reducing the length of cervical collar immobilization.9–13
The aim of this study was to assess whether or not obtaining MRI resulted in a change in management for blunt trauma patients with a negative CT scan of the c-spine, and whether it was necessary especially for patients deemed obtunded or unreliable for examination. We hypothesized that especially among the unreliable, obtaining additional MRI testing would result in findings that lead to a change in management.
Methods
Prior to inception, this study was reviewed by the Institutional Review Board (IRB) at Hurley Medical Center, a university affiliated, level I trauma center in Flint, Michigan, and deemed exempt.
Patients
The inclusion criteria for the study were adult (18 years or older) blunt trauma patients with a negative CT scan of the c-spine and subsequent MRI. As part of our institution's protocol, all patients who underwent the CT had failure of any of the National Emergency X-Radiography Utilization Study (NEXUS) criteria.14 We categorized patients according to whether or not they could be reliably examined into: reliable or unreliable. Reliable patients were defined as those with a GCS score of 14 or more. Clinical findings including midline neck pain, or neurological deficit (defined as abnormal sensation or weakness) were recorded for these patients. Unreliable patients were defined as those who were obtunded, intoxicated or at suspicion for impaired judgment (eg, had distracting injuries, any form of developmental delay or similar). We used a GCS score of 13 or less on initial presentation to define obtunded patients. Similar studies have used a GCS of 13 or less,6 ,15 or a GCS score of 14 or less9 ,11 ,16 ,17 to describe patients who are obtunded or unreliable for examination. Intoxicated patients were deemed as such if they either had a recent history of ingestion of an intoxicating agent, evidence on examination or via positive laboratory testing. We used the legal driving limit in Michigan as a cut-off for alcohol intoxication (0.08% blood alcohol level).18 Clinical findings such as neck pain or neurological deficit could not be collected in obtunded or unreliable patients being clinically challenging to observe these findings in such patients.
Outcome measures
The primary outcome was to assess whether or not there was a change in management for patients included in the study, and establish whether obtaining the MRI was necessary. All patients included in the study initially arrived in a semirigid cervical collar. After initial collar placement, the following management outcomes were possible:1 c-spine clearance and collar removal,2 continued collar immobilization only, or3 neck surgery. We defined change in management as occurring after the MRI result, and if a decision was made by the attending treating physician to either continue cervical collar immobilization or if the patient underwent neck surgery.
Collection of data
The study entailed a retrospective review of the trauma registry database to identify adult blunt trauma patients who underwent CT of the c-spine from January 1, 2006 to June 30, 2014. The trauma registry was queried for reports of CT scans with fractures, malalignment, or evidence of acute injury. If at least one of the aforementioned findings was evident, the CT scan was considered positive (patients excluded). Of the remaining patients with negative CT scans, those who were found to have underwent subsequent MRI of the c-spine were identified and represented the study population.
CT imaging of the c-spine was performed using a Siemens Somatom 64-slice multidetector CT (MDCT). The imaging protocol included 2 mm cuts, and scans were performed without contrast. All MRI studies performed from January 2010 to June 2014 were performed using a General Electric Optima 450 W, 1.5 T scanner. Prior to 2010, MRIs were performed using a GE Signa 1.5 T or a GE Horizon 0.7 T scanner. During the study period, there was no specific protocol in place for obtaining the MRI on blunt trauma patients and the decision was based on the clinical judgment of the attending physician. All CT and MRI findings were recorded from interpretations of attending board certified radiologists at the time of injury and during the particular hospital encounter.
Medical records were reviewed for the study population to obtain their age, gender, mechanism of injury, initial symptoms, GCS score, injury severity score (ISS), neck and neurological examinations on initial presentation, neurosurgery and orthopedic consultations, and progress and discharge notes for information on change in management. MRI reports were reviewed for fractures, malalignment, ligamentous injury, cord contusion, spinal hematoma, bone contusion, and disc lesion. We defined disc lesions as the presence of disc/osteophyte complexes with either disc protrusion, spinal canal stenosis, neural foraminal narrowing or mass effect on the thecal sac. Patients exhibiting any of these seven findings were coded as ‘positive’ for MRI result, and otherwise coded as ‘negative’. Change in management was determined for continued cervical collar immobilization or neck surgery, and proved difficult for some patients due to incomplete documentation.
Data analysis
To assess the overall impact of MRI on management, we compared patients with positive MRI to those with negative MRI. This allowed linking the decision to obtain the MRI to patient benefit as measured by change in management. Next, we compared patients deemed reliable to those deemed unreliable for examination to evaluate whether a significant relationship existed between change in management and examination reliability. Finally, we analyzed the data for patients only with a positive MRI. For quantitative variables (eg, age), group comparisons were made using a Wilcoxon rank-sum test. For binary variables (eg, gender), group comparisons were made using Fisher's exact test. Differences between groups were deemed significant for p values <0.05. As with any statistical analysis, it is possible that any significant result could be merely be a type I error. JMP Pro V.11.2.1 was used to conduct the statistical analysis.
A propensity matching analysis was performed to evaluate the outcomes of patients who received CT and MRI versus those who received CT only. The propensity scores were developed using multivariate logistic regression with age, gender, ISS, GCS, and type of blunt trauma as the independent variables, resulting in a control group. We reviewed the charts for patients in the control group to collect data on the variables included in the study (eg, neck pain, collar removal, neck surgery, etc).
Results
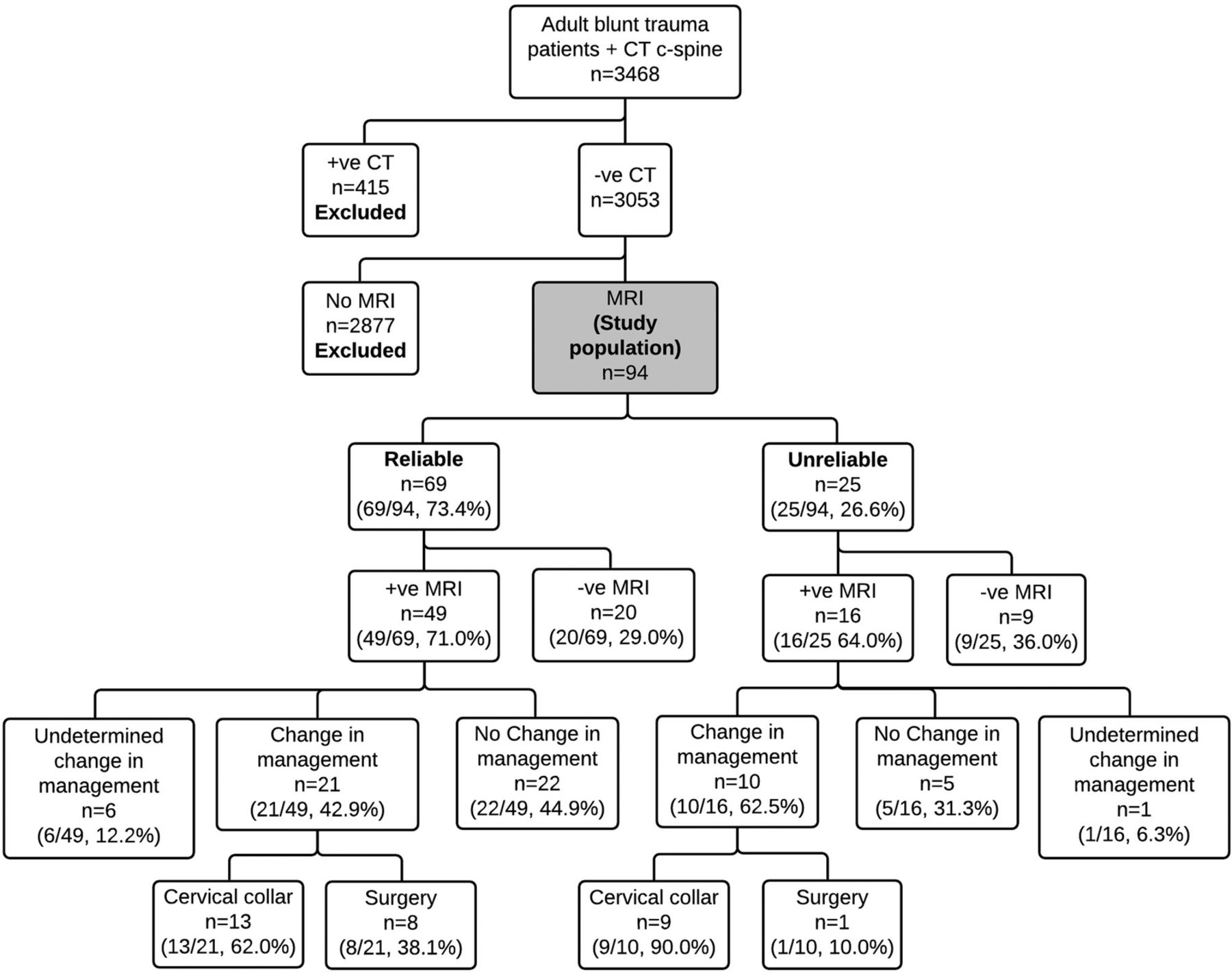
We identified 3468 adult blunt trauma patients who underwent CT of the c-spine during the study period. In 415 patients, the CT scan was positive (excluded). Of the remaining 3053 patients with negative CT scans, 94 were found to have underwent subsequent MRI of the c-spine. The top portion of figure 1 illustrates the filtering process that resulted in the study population. Table 1 contains basic demographics and the specific MRI findings for these 94 patients (69 male and 25 female). The duration between having the CT and MRI averaged 1.42 days. Overall, 65 (69.1%) patients had a positive MRI result and 29 (30.9%) had a negative result. Patients had an average of 1.1 MRI findings with the most frequently encountered finding being disc lesion in 55 (58.5%) patients, that was found either solely or in combination with other findings. The MRI findings of patients with disc lesions consisted of disc osteophyte complexes with either canal narrowing, bilateral foraminal stenosis, disc bulges, and/or flattening of the thecal sac, all of which were of mild-to-moderate severity. Thirty-one of the 65 (47.7%) patients with positive MRI had a change in management, 27 (41.5%) had no change in management, and the remaining 7 (10.8%) were undetermined for a change in management. The top two occurring mechanisms of injury among the study population were falls and motor vehicle collisions which combined accounted for 72.3% of the patients. An overview of the main study results is outlined in figure 1.
Basic demographics and specific MRI findings for the 94 patients in the study
{kind=link}
Filtering process resulting in the study population with an overall view of study results.
Patient reliability
Of the 69 patients deemed reliable at time of initial presentation, 57 (82.6%) had neurological symptoms and 12 (17.4%) had neck pain. Comparing the 69 patients (73.4%) deemed reliable with the 25 (26.6%) deemed unreliable, we found no significant difference in age and gender but identified that on average, unreliable patients had an ISS 4.5 higher (p=0.0247) and waited 2.8 days longer to have an MRI (p=0.0047). Even though the rate of positive MRI was high and included 71.1% of those reliable for examination and 64.0% of those unreliable for examination, yet a positive result was not significantly associated with patient reliability. Each of the various MRI findings was not significantly associated with patient reliability. Among the 25 unreliable patients (table 2), 13 patients (52%) had their c-spine cleared and collar removed after obtaining the MRI. There were no data to suggest occurrence of delayed injuries among these patients.
Basic demographics and specific MRI findings for the 16 unreliable patients with positive MRI
MRI result
We compared the 31 patients with change in management (all of which had positive MRI) to the 49 patients without a change in management (with either positive or negative MRI), thus excluding 14 patients with undetermined change in management (7 with positive and 7 with negative MRI). Change in management was not significantly associated with examination reliability and gender but was highly dependent on the MRI result. On average, patients with a change in management had an ISS 2.4 higher (p0.0478), were 9.1 years older (p=0.0084), and had 1.4 more MRI findings (p<0.0001) than those without a change in management. When comparing specific MRI findings by change in management, disc lesion, cord contusion, ligamentous injury, bone contusion, and malalignment all had significantly higher incidence rates for patients with a change in management than those without. No significant differences in the mechanism of injury rates by change in management were detected.
Next, we analyzed the 58 patients (43 reliable and 15 unreliable) with a positive MRI and a definitive value (yes or no) for change in management (ie, excluding those with undetermined change in management), and noted that 31 of the 58 (53.4%) had a change in management. When comparing MRI-positive patients with and without a change in management, there were no significant differences in age, ISS, or change in management for the two groups. Twenty-one of the 43 (48.8%) reliable patients had an associated change in management (13 continued collar placement and 8 surgery) and similarly did 10 of the 15 (66.7%) unreliable patients (9 continued collar immobilization and 1 surgery). Of the aforementioned 58 patients, 28 (48.3%) had disc lesions as the only MRI finding: 23 (82%) reliable patients (18 had neurosensory deficit; 5 had neck pain), and 5 (18%) unreliable patients. Six of the 28 with disc lesions (21.4%) underwent a change in management: 4 reliable patients (1 surgery and 3 continued cervical collar immobilization), and 2 unreliable patients (both continued collar immobilization). The clinical decision for the two unreliable patients to continue collar immobilization was unclear; however, their mechanisms of injury were fall and hanging, respectively.
Propensity matching resulted in a control group consisting of 93 patients (due to one study patient missing an ISS). We compared these patients with the 94 study patients and found no significant differences in age, gender, ISS, GCS, and mechanism of injury between both groups since these variables formed the basis for the matching. Patients in the study group had a higher percentage of neck pain (93.5% vs 24.7%, p<0.0001), motor deficit (78.5% vs 2.2%, p<0.0001), and sensory deficit (8.6% vs 3.3%, p=0.1132), and a lower percentage of patients had their c-spine cleared with collar removal (55.1% vs 79.8%, p=0.0008). In terms of change in management, a higher percentage of the study group had continued cervical collar immobilization (34.2% vs 18.5%, p=0.0181), and neck surgery (9.6% vs 1.1%, p=0.0096).
Discussion
The main reason for adopting additional imaging after a negative CT scan result is to avoid potential catastrophic consequences of missed injury.12 On the other hand, obtaining MRI is costly, time-consuming, and carries potential risks to critically ill patients during transfer. Routinely adding MRI to all blunt trauma patients would represent a significant burden on the healthcare system and waste hospital resources. A recent study demonstrated that although the cost of MRI is substantial, over 5000 MRIs on obtunded patients would be required to match the cost of providing care for one quadriplegic patient, which far exceeded the number needed to be treated in their study.8 A review5 in 2012 indicated that since 2004, authors have conducted three meta-analyses7 ,15 ,19 on the subject, along with a review from the EAST.20 The latter EAST review concluded that due to the variability of screening performance, clinicians can clear the spine of obtunded trauma patients using MDCT alone or with MDCT followed by MRI with implications to either approach. As mentioned earlier, a recent EAST review, however, recommended cervical collar removal in the obtunded adult patient after a negative high-quality c-spine CT scan only.4 Some authors have suggested that additional testing should be evaluated on a patient-by-patient basis because MRI is more likely to detect certain types of injuries (eg, ligamentous instability) than a CT scan.10
A 7-year retrospective study—similar to ours—by Fisher et al8 advocated routine use of MRI in the evaluation of obtunded blunt trauma patients based on the observation that 5% of patients had clinically significant injuries with 3% requiring intervention. One major difference between that study and ours is the definition of ‘clinically significant’ injuries. In the Fisher et al study, change in management was assessed only after determination of clinical significance defined as the detection of specific MRI findings, regardless of their impact on management. In our study, we did not predefine injuries in order to establish ‘clinical significance’. MRI findings of patients that eventually underwent a change in management were deemed ‘clinically significant’ in retrospect, that is, only if they resulted in a change in management. A second difference between the two studies was the type of injuries encountered. In the Fisher et al study, a majority of patients had some form of ligamentous injury as opposed to disc lesions and cord contusions in our study.
One aspect that differentiates this study from others is that in addition to obtunded or unreliable patients, it incorporates the non-obtunded symptomatic or reliable patients in order to assess the value obtained from ordering the MRI on these patients. Additionally, it includes findings that may have been disregarded or often described as ‘degenerative’ or ‘non-acute’. This enables the evaluation of ‘acute on-top-of chronic’ events. Patients with chronic degenerative findings have higher vulnerability to injury following trauma, even minimal trauma. For example, patients with pre-existing disc bulges have higher vulnerability to post-traumatic disc prolapse. In addition, patients with degenerative central canal stenosis or foraminal narrowing have increased susceptibility of cord contusions or nerve compression. Finally, we note the susceptibility of osteophytes to fracture. In this study, the majority of patients with a positive MRI finding had a ‘disc lesion’. Among those, some had such finding as the only finding on the MRI and resulting in the collar being kept in place. Although these patients were all symptomatic and although the collar may have provided symptomatic relief, no evidence exists on the long-term outcomes of such practice.21 Physicians may often prescribe cervical collars by convection for patients presenting with neck pain.21 In our study, the MRI finding of disc lesions appears to have led to this practice.
Being a retrospective study, we could not directly assess the presence and severity of degenerative c-spine conditions prior to injury. Nonetheless, we were able to use the MRI findings to characterize these likely pre-existing abnormalities or those considered of a degenerative nature in relationship to the acute injury. For example, we could assess the presence and extent of osteophyte encroachment on the central canal causing narrowing. We hypothesize that the presence of such findings predisposes patients for a lower threshold to develop cord compression by having a diminished capacity to accommodate post-traumatic edema. This may render such patients more vulnerable for spinal cord compression following trauma. In this, and similar settings, the MRI was able to detect ‘acute on-top-of chronic’ events. Although the CT can detect degenerative findings, only the MRI can discern the presence, extent, and impact of injury to the spinal cord or root injury. In the acute setting, clinicians generally consider a CT scan that shows only degenerative disease as negative. A recent study has shown that the agreement of interpreting and reporting varying degenerative findings on cervical MRI has not been well assessed.22
Disc lesions were the only positive MRI finding in 45.3% of patients with positive MRI, of which only 6 patients (6/53, 11.3%) had a change in management. This raises the flag that in some patients with CT scans of the c-spine described as ‘negative’, detection of a disc lesion (usually considered ‘degenerative and non-acute’),23 may represent an acute on-top-of chronic cause that may explain post-traumatic symptoms; or represent traumatic exacerbation of existing disease that may require subsequent intervention. These findings are only more accurately assessed via MRI. Thus, a CT scan revealing chronic or degenerative changes does not necessarily exclude injury, and suspicion should be raised in blunt trauma patients with evidence of degenerative findings on the CT. MRI findings such as cord contusions, effacement of the ventral sac, or neural foraminal narrowing suggest that CT imaging alone lacks sufficient sensitivity to exclude injury. Significantly, falls in the elderly—a group of patients more likely to have chronic and degenerative c-spine conditions—represent a major proportion of admissions to emergency departments and trauma centers. We are not suggesting that every elderly patient who falls and has any sort of degenerative findings on CT should get an MRI; rather, we are trying to raise a flag that among elderly blunt trauma patients, the treating physician should maintain a high index of suspicion for injury even when they have a CT scan of the c-spine that is read as ‘negative for acute events'.
As with most studies, there were some limitations to this study. First, this is a single-institution, retrospective review. Since no protocol existed for ordering the MRI, we could not ascertain whether the presence of certain findings were the reason why the MRI was ordered. However, all patients who underwent MRI had neck pain or midline tenderness, neurological deficit, or were obtunded. We also relied on the CT and MRI reports interpreted by attending board certified radiologists, which may have carried the potential for subjective interpretation. Additionally, in retrospect, we could not ascertain the specific reasons behind the decision to change management, especially in the absence of predetermined treatment criteria or protocols. We cannot definitively conclude that the MRI findings alone led to the change in management, thus the possibility for individual spine surgeon's preference exists. Since we only included patients who had a negative CT scan followed by MRI (only 2.7% of our blunt trauma population), the potential for selection bias also exists. Because of this, it should be clear that the results of this study are to apply only to patients who are reliable yet at clinical suspicion for c-spine injury despite a negative CT scan or to those deemed unreliable for examination. Some data related to complications of prolonged cervical collar immobilization in patients with concomitant traumatic brain injuries (such as skin break down and elevated intracranial pressure even for short periods of time) were not available. Finally, estimation of radiologists' error rates or evaluation of CT films that may have been re-reviewed following the MRI results was not possible due to lack or incomplete documentation.
Even though the study/control groups were similar in age, gender, ISS, GCS, and type of blunt trauma, they had differences. Non-obtunded patients in the study group were at risk for a positive MRI because ‘clinical suspicion’ (presence of neck pain, neurological deficit, or possibly undocumented suspicion for injury or a false-negative CT) existed. This kind of ‘suspicion’ per se plays a role in determining whether the MRI should be ordered, and accordingly, represents a ‘risk’ for patients being predisposed for a positive MRI. It was almost impossible to include patients in the control group with the same ‘risk’ for a more accurate comparison because most of these type of patients would have most likely received the MRI and included in our study population. Our results demonstrate that among these groups of patients who were at this clinical suspicion or were unreliable for examination, the MRI was indeed of value as it represented a factor that contributed to alteration of patient management.
Conclusion
Our data suggest that patients benefited from the additional MRI in two ways. First, MRI improved the detection of potential missed, occult, soft tissue or ligamentous injuries of blunt trauma patients with CT results reported as normal, without injury, or ‘negative for an acute event’. Disregarding degenerative findings of the c-spine on CT as being ‘non-acute’ may deviate attention from further analysis of traumatic effects that are only discernable on MRI. Second, MRI findings may have provided explanation for some clinical presentations (neck pain or tenderness, neurological findings) not otherwise explained by the CT. The experience in our institution over the 8-year study period supports the use of MRI in adult obtunded trauma patients or those deemed unreliable for examination, or in the non-obtunded reliable patients in whom clinical suspicion exists after a negative CT scan of the c-spine. Therefore, in such patients, suspicion for injury should not be totally eliminated and MRI should be considered as a supplement and not be rejected solely based on a CT of the c-spine described as ‘negative’. To validate the value of MRI observed in this study, we suggest a prospective study that assesses the negative predictive value of CT scan, and the use of MRI as an adjunct to CT versus CT alone. A study of this nature will further verify advocacy for use of additional MRI in the assessment of the c-spine following blunt trauma.
References
Footnotes
Contributors MAM was the primary author involved and responsible for all aspects of the study. KDM analyzed the data and contributed to the writing of the manuscript. GS-D, DS, KLW, and LM revised and made significant edits to the manuscript. KME,AP, and DC were involved in data collection and revision of the manuscript. MLM revised the manuscript and provided overall supervision of the process.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.